Chapter 15
Chest Pains and Angina
1. Are most emergency room (ER) visits for chest pain caused by acute coronary syndromes (ACS)?
2. What are the other important causes of chest pains besides chronic stable angina and ACS?
The differential diagnosis for chest pains include the following:



 Coronary artery spasm (Prinzmetal angina, cocaine abuse)
Coronary artery spasm (Prinzmetal angina, cocaine abuse)


 Musculoskeletal pain and cervical radiculopathies (costochondritis)
Musculoskeletal pain and cervical radiculopathies (costochondritis)







3. Does an elevated troponin level make the diagnosis ACS?
Not necessarily. Although troponin elevations are fairly sensitive and specific for myocardial necrosis, it is well known that other conditions can also be associated with elevations in cardiac troponins. Importantly, troponin elevation can occur with pulmonary embolus and is in fact associated with a worse prognosis in cases of pulmonary embolus in which the troponin levels are elevated. Myopericarditis (inflammation of the myocardium and pericardium) may also cause elevated troponin levels. In addition, aortic dissection that involves the right coronary artery may lead to secondary MI. Further, troponins may be modestly chronically elevated in patients with severe chronic kidney disease. Troponin elevation has also been noted in patients with acute stroke. Studies to delineate the etiology of this are ongoing.
5. What are the associated symptoms that persons with angina may experience in addition to chest discomfort?




6. What are the major risk factors for CAD?







7. What symptoms and findings make it more (or less) likely that the patient’s chest pains are due to angina (or that the patient has ACS)?
The answer to this question is given in Tables 15-1 and 15-2, which are taken from an excellent review article on this subject in the Journal of the American Medical Association (JAMA). The tables summarize many of the relevant questions and the value of the chest pain characteristics in distinguishing angina and ACS-MI pain from other causes. It is important to remember, no single element of chest pain history is a powerful enough predictor to use alone to rule out ACS.
TABLE 15-1
SPECIFIC DETAILS OF THE CHEST PAIN HISTORY HELPFUL IN DISTINGUISHING ANGINAL CHEST PAIN IN PATIENTS WITH MYOCARDIAL INFARCTION FROM NONCARDIAC CAUSES
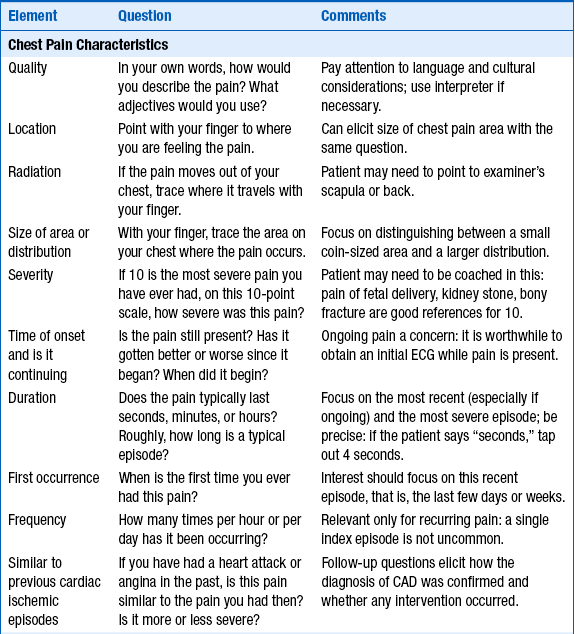
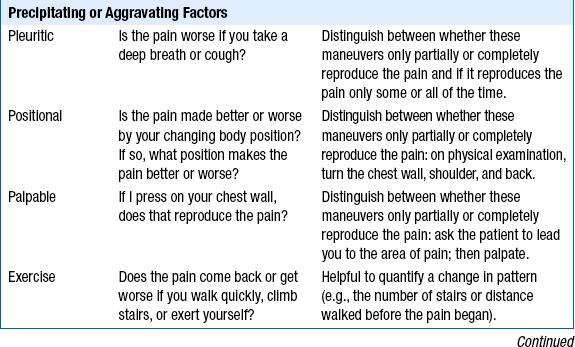
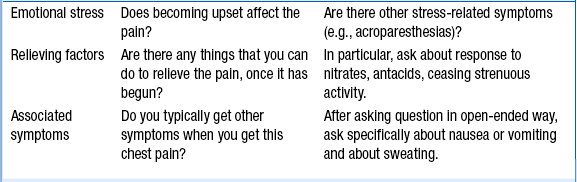
CAD, Coronary artery disease; ECG, electrocardiogram.
Modified from Swap CJ, Nagurney JT: Value and limitations of chest pain history in the evaluation of patients with suspected acute coronary syndromes, JAMA 294:2623-2629, 2005.
TABLE 15-2
VALUE OF SPECIFIC COMPONENTS OF THE CHEST PAIN HISTORY FOR THE DIAGNOSIS OF ACUTE MYOCARDIAL INFARCTION (AMI)
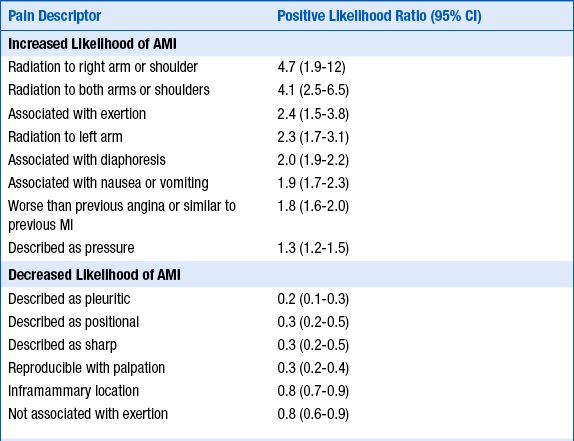
AMI, Acute myocardial infarction; CI, confidence interval.
Modified from Swap CJ, Nagurney JT: Value and limitations of chest pain history in the evaluation of patients with suspected acute coronary syndromes, JAMA 294:2623-2629, 2005.
 Quality and characteristics of chest discomfort: Patients who describe a chest tightness or pressure are more likely to have angina. Pain that is stabbing, pleuritic, positional, or reproducible is less likely to be angina and is often categorized as atypical chest pain, although the presence of such symptoms does not 100% rule out that the pain may be due to CAD. Although it is generally accepted that a more diffuse area of discomfort is suggestive of angina, whereas a coin-sized, very focal area of discomfort is more likely to be noncardiac, this distinction in itself is not enough to confidently dismiss very focal pain as noncardiac. The severity of the pain or discomfort is not helpful in distinguishing angina from other causes of chest pain. Chest pain that is sudden in onset and maximal intensity at onset is suggestive of aortic dissection. Patients with aortic dissection may describe the pain as tearing or ripping and may describe pain radiating to the back. The Levine sign (pronounced “la vine,” and no relationship to this book’s editor) is when the patient spontaneously clenches his or her fist and puts it over the chest while describing the chest discomfort.
Quality and characteristics of chest discomfort: Patients who describe a chest tightness or pressure are more likely to have angina. Pain that is stabbing, pleuritic, positional, or reproducible is less likely to be angina and is often categorized as atypical chest pain, although the presence of such symptoms does not 100% rule out that the pain may be due to CAD. Although it is generally accepted that a more diffuse area of discomfort is suggestive of angina, whereas a coin-sized, very focal area of discomfort is more likely to be noncardiac, this distinction in itself is not enough to confidently dismiss very focal pain as noncardiac. The severity of the pain or discomfort is not helpful in distinguishing angina from other causes of chest pain. Chest pain that is sudden in onset and maximal intensity at onset is suggestive of aortic dissection. Patients with aortic dissection may describe the pain as tearing or ripping and may describe pain radiating to the back. The Levine sign (pronounced “la vine,” and no relationship to this book’s editor) is when the patient spontaneously clenches his or her fist and puts it over the chest while describing the chest discomfort.







8. If one is still in doubt as to the diagnosis of CAD, should a stress test be obtained?
Yes. Stress testing for diagnostic purposes is best in patients who, after initial evaluation, have an intermediate probability of having CAD. For example, in a patient with a pretest probability of having CAD of 50%, a positive exercise stress test makes the posttest probability of CAD 85%, whereas a negative exercise stress test makes the posttest probability of CAD just 15%. Stress testing may also be used for prognostic purposes. Stress testing is discussed in greater detail in the chapters on exercise stress testing (Chapter 6), nuclear cardiology (Chapter 7), echocardiography (Chapter 5), and magnetic resonance imaging (Chapter 10). Coronary computed tomography (CT) angiography is an emerging alternate form of diagnosis and is discussed in Chapter 9.
9. Are there exceptions to the classic presentations of anginal pain?
10. Who first described angina, and when?
11. What is Prinzmetal angina?
Bibliography, Suggested Readings, and Websites
1. Alaeddini, J. Angina Pectoris. Available at http://www.emedicine.com.
2. Cohn, J.K., Cohn, P.F. Chest pain. Circulation. 2002;106:530–531.
3. Delehanty, J.M. Cardiac syndrome X: angina pectoris with normal coronary arteries. Available at http://www.utdol.com.
4. Delehanty, J.M. Variant Angina. Available at http://www.utdol.com.
5. Haro, L.H., Decker, W.W., Boie, E.T., et al. Initial approach to the patient who has chest pain. Cardiol Clin. 2006;24:1–17.
6. Higginson, L.A.J., Chest pain. Porter R.S., Kaplan J.L., eds. The Merck Manual Online. Merck Sharp & Dohme Corp.: Whitehouse Station, N.J., 2012 Available at http://www.merck.com/mmpe Accessed March 27, 2013
7. Lanza, G.A. Cardiac syndrome X: a critical overview and future perspectives. Heart. 2007;93:159–166.
8. Mayer, S., Hillis, L.D. Prinzmetal variant angina. Clin Cardiol. 1998;21:243–246.
9. Meisel, J.L. Diagnostic Approach to Chest Pains in Adults. Available at http://www.utdol.com.
10. Ringstrom, E., Freedman, J. Approach to undifferentiated chest pain in the emergency department: a review of recent medical literature and published practice guidelines. Mt Sinai J Med. 2006;73:499–505.
11. Swap, C.J., Nagurney, J.T. Value and limitations of chest pain history in the evaluation of patients with suspected acute coronary syndromes. JAMA. 2005;294:2623–2629.
12. Tanser, P.H., Approach to the cardiac patient. Porter R.S., Kaplan J.L., eds. The Merck Manual Online. Merck Sharp & Dohme Corp.: Whitehouse Station, NJ, 2012 Available at http://www.merck.com/mmpe Accessed March 27, 2013
13. Warnica, J.W., Angina Pectoris. Porter R.S., Kaplan J.L., eds. The Merck Manual Online. Merck Sharp & Dohme Corp.: Whitehouse Station, NJ, 2012 Available at http://www.merck.com/mmpe Accessed March 27, 2013

