17 Nose
Summary and Key Features
• Filler rhinoplasty is a safe and effective technique to augment and reshape the nose without social downtime
• Mild hump, short nose, saddle nose, and flat nose are good indications for filler rhinoplasty
• Augmentation of the nasal dorsum should be performed for patients with a mild hump, short nose, saddle nose, and flat nose
• Priority should be placed on enhancing the nasolabial angle and the columella in patients with plunged tip and inadequate tip projection
• In order to raise the tip of the nose, the injection should be made between the footplates of the medial crura and the anterior nasal spine or in the columella, as opposed to the nasal lobule itself
• Hyaluronic acid fillers high in viscoelasticity are recommended for filler rhinoplasty owing to the fact that any inadvertent irregularity can be readily reversible by hyaluronidase
• The use of a cannula has some benefits over using a needle in filler rhinoplasty because it can prevent risks of unwanted bruising as well as embolization
• When the cannula is used for filler rhinoplasty, the entry point for the blunt cannula should be made at the infratip lobule of the nasal tip by a 21-gauge sharp needle
• Local anesthetics containing lidocaine with 1 : 100 000 epinephrine should be injected at the entry point 3–5 minutes prior to puncture using a 21-gauge needle
The attractively proportioned nose and face
The nose is divided into several subportions including the dorsum, sidewall, nasal tip, ala nasi, and columella. Such regional subdivision helps with surgical planning and descriptions of the cosmetic procedures. In addition, there are certain topographic landmarks of the nose used for describing the cosmetic and reconstructive procedures. Recognized topographical facial landmarks are shown in Figure 17.1. Of such landmarks, the nasion, sellion (radix), rhinion, and pronasale are worthy of mention with respect to filler rhinoplasty. Although the term ‘nasion’ is sometimes confusingly used to refer to the deepest point of the nasal root, it in fact represents the median anterior tip of the nasofrontal suture. Rather, the sellion represents the deepest point of the nasal bone or the nasofrontal angle. Since the sellion is also the bony landmark, corresponding to surface anatomy, the term ‘radix’ is used for the deepest point of the nasal root or the nasofrontal angle. Rhinion refers to the osteocartilaginous junction, while pronasale is the most prominent point of the nasal tip and the subnasale represents the junction between the columella and philtrum.
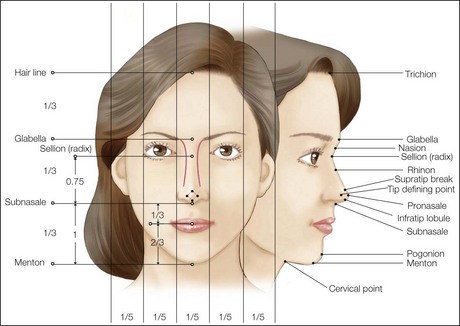
On the frontal view, a balanced face should divide into equal vertical thirds and equal horizontal fifths, as shown in Figure 17.1. The ideal length of the nose in proportion to the face is three-quarters the length of the lower one-third of the face, from the subnasale to mentum. Meanwhile, the ideal nasal width at the alar base is believed to correspond to the intercanthal distance, which equals one-fifth of the facial width. The width of the body of the nose should be 80% of the width of the nose at the alar bases. The narrowest point of the nasal dorsum is at the radix, where the width at the radix approximates the height of the palpebral fissure. A gentle curve emanating from the medial brow courses along the lateral border of the nasal dorsum to end at the ipsilateral tip-defining point. Any irregularities of this line will be easily noticeable as deviations from the contralateral line, thereby contributing to asymmetry and unsightly appearance.
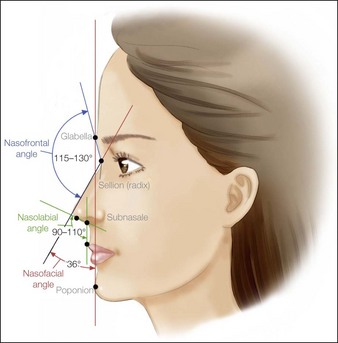
On the lateral view, there are certain facial angles related to the nose that deserve special mention in evaluating filler rhinoplasty patients (Fig. 17.2). The glabella-to-radix line intersecting with the radix-to-tip line forms the nasofrontal angle. Ideally, this angle should be within 115–130°. Meanwhile, the nasofacial angle is the angle formed by the line tangent to the nasal dorsum intersecting with the vertical facial plane, which is a two-dimensional coronal section connecting the glabella-to-pogonion line. The aesthetic ideal for the nasofacial angle is 35–40°. The nasolabial angle is defined by the line from the subnasale to the superior vermilion border of the upper lip intersecting with the line tangent to the columella from the subnasale. The ideal aesthetic range should be between 90° and 110° depending on the ethnicity and sex.


Injection techniques by nasal region
Injection techniques by each type of nose












Adverse effects
The most serious adverse effect relating to filler rhinoplasty would be embolization due to intravascular injection of fillers. It is for this reason that use of a cannula is generally recommended to guard against such risks; where the situation calls for the use of a needle, aspiration for blood should be performed before each filler injection to prevent any intravascular injection. While intravascular injection in the worst case could even lead to skin necrosis, in most cases infection can be suspected when patients present with erythematous swelling in combination with multiple pustules (Fig. 17.9). Any blanching occurring immediately after the filler injection followed by subsequent violaceous color change should be considered as an ischemic sign of embolization, for which adequate treatment must be administered.


Behrbohm H, Tardy ME. Essentials of septorhinoplasty. Philosophy – approaches – techniques. New York: Thieme; 2004.
Carruthers J, Carruthers A. Soft tissue augmentation. Philadelphia: Elsevier, 2005.
Dhong ES, Han SK, Lee CH, et al. Anthropometric study of alar cartilage in Asians. Annals of Plastic Surgery. 2002;48:386–391.
Gunter JP, Rohrich RJ, Adams WP. Dallas rhinoplasty; nasal surgery by the masters. Missouri: Quality Medical Publishing; 2007.
Larrabee WF, Makielski KH, Henderson JL. Surgical anatomy of the face. Philadelphia: Lippincott Williams & Wilkins; 2004.
Tanaka Y, Matsuo K, Yuzuriha S. Westernization of the Asian nose by augmentation of the retropositioned anterior nasal spine with an injectable filler. Eplasty. 2011;11:e7.
Tardy ME, Brown RJ. Surgical anatomy of the nose. New York: Raven Press; 1990.
Tebbetts JB. Primary rhinoplasty: redefining the logic and techniques. Philadelphia: Mosby Elsevier; 2008.






