Chapter 25 Miscellaneous supportive therapies for stress, ageing, cancer and debility
Cancer chemoprevention
Cancer chemoprevention can be defined as ‘the prevention of cancer in human populations by ingestion of chemical agents that prevent carcinogenesis’. It is also important to differentiate between cancer prevention (e.g. cessation of cigarette smoking) and cancer chemotherapy (the use of cytotoxic drugs after cancer diagnosis). Cancer chemoprevention has now developed into a well-defined discipline. Several recent epidemiological studies have demonstrated that dietary factors may reduce the incidence of cancers. In one study, involving 250,000 people, an inverse correlation was found between the incidence of lung cancer among people who smoke and consume carotene-rich foods. As well as carotenoids, there was a similar finding for vitamin C and oesophageal and stomach cancers; selenium and various cancers; and vitamin E and lung cancer. Epidemiological studies may help to find leads for chemopreventive agents, which can then be tested in laboratory experiments. Almost 600 ‘chemopreventive’ agents are known and they are usually classified as: inhibitors of carcinogen formation (ascorbic acid, tocopherols, phenols), inhibitors of initiation (phenols, flavones) and inhibitors of postinitiation events (β-carotene, retinoids, terpenes). Many are items of food or beverages (e.g. tea) and are sometimes called ‘functional foods’ or ‘nutraceuticals’. Those that are used purely as foods are not covered here, but some others can be found in the chapters for which they are most useful (e.g. ginger, Chapter 14; garlic, Chapter 15). Further examples are given in Table 25.1.
| Group | Examples |
|---|---|
| Micronutrients | Vitamins A, C and E, selenium, calcium, zinc |
| Food additives | Antioxidants |
| Non-nutritive molecules | Carotenoids, coumarins, indoles, alkaloids |
| Industrial reagents | Photographic developers, herbicides, UV-light protectors |
| Pharmaceuticals | Retinoids, antiprostaglandins, antithrombogenic agents, non-steroidal antiinflammatory drugs |
| Hormones and antihormones | Dehydroepiandrosterone, tamoxifen |
Chemopreventive agents may even work in synergy, with several components contributing to the overall effect, which may be the case with plant drugs. This approach has great promise, with both natural products and synthetics being potentially useful. Dietary campaigns by government bodies, the American Cancer Society and others recommend that 5–7 servings of vegetables be consumed daily to function as a source of cancer chemopreventive agents. However, it is not reasonable to assume that chemopreventive agents will safeguard humans from known carcinogenic risks such as smoking. As knowledge of these agents increases they will play an increasing role in cancer prevention. Chemoprevention will not be covered further, apart from tea, as it is a vast subject in its own right. However, there are some useful recent reviews which discuss compounds, mechanisms and future directions available, such as Shu et al (2010), Gullett et al (2010) and Cerella et al (2010). Some data on the chemopreventive effects of garlic, anthocyanins (bilberry) and others can be found in the monographs of these plants.
Tonics, stimulants, adaptogens and supportive therapies
Açai berry, euterpe oleracea mart. (euterpe fructus)
Therapeutic uses and available evidence
This botanical drug has become very popular despite a lack of scientific evidence. Clinical data are lacking. The high content of polyphenols has been linked to a range of reported (mostly in vitro) antioxidant, antiinflammatory, antiproliferative and cardioprotective properties. Açai demonstrates promising potential with regard to antiproliferative activity and cardioprotection, but further studies are required (Heinrich et al In press).
Ashwagandha, withania somniferum (L.) dunal
Constituents
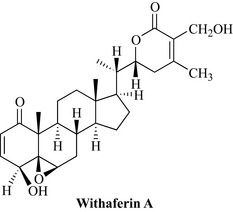
The root contains steroidal lactones (the withanolides A–Y), withaferin A (Fig. 25.1), withasomniferols A–C and others, phytosterols (such as the sitoindosides) and the alkaloids anahygrine, cuscohygrine, ashwagandhine, ashwagandhinine, withasomnine, withaninine, somniferine and others.
Therapeutic uses and available evidence
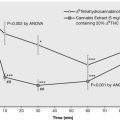
Extracts are antioxidant, immunomodulatory and sedative but, despite their wide usage, much of the clinical knowledge is still anecdotal. The few clinical trials which have been carried out are of doubtful quality and cannot be used to confirm efficacy, but they do show that the herb is generally safe. Many of the pharmacological effects have been substantiated in animal studies: for example, the adaptogenic and antistress activity was found to be comparable to that of ginseng, in mice and rats, and immunomodulatory activity has been confirmed. The extract has sedative activity and is reported to be anxiolytic, acting via the GABA-ergic system (Bhattarai et al 2010) and numerous other actions have been documented (for review, see Kulkarni and Dhir 2008). The usual dose of powdered root is 3–6 g daily. Side effects are rare but high doses can cause gastrointestinal irritation.
Centella, centella asiatica (L.) urban (centellae herba)
The herb has already been described in Chapter 22 (Skin). In addition to the wound healing effects, the plant is considered a ‘rasayana’ in Ayurvedic medicine; it enhances the immune system and is considered to have a rejuvenating, neurological ‘tonic’ and mild sedative effect. The immunomodulating effects of the herb have been shown in vitro and in vivo in mice. Studies in rats have shown that asiatic acid has some benefits on memory and learning (Nasir et al 2011), and that the extract can protect against certain types of neurodegeneration (Haleagrahara and Ponnusamy 2010), but in general, evidence for this use is lacking. A small double-blind, placebo-controlled, randomized trial in healthy elderly volunteers in Thailand found that their health-related quality of life was improved and lower extremity strength increased after taking centella extract for 3 months (Mato et al 2009). It may be taken orally, often as an infusion, and applied topically. Other reported effects for the herb include anti-ulcer activity and spasmolytic effects. The powdered leaf is taken at an internal dose of 0.5–1 g daily, or the equivalent in the form of an extract.
Ginseng, panax ginseng C.A. meyer (panax radix), eleutherococcus senticosus (rupr. & maxim.) maxim. and related ‘ginseng’ species
Constituents
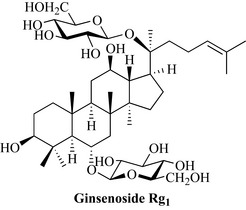
All types contain saponin glycosides (the ginsenosides Ra, Rb, Rg1, Rg2, Rs, etc.; Fig. 25.2). The ginsenosides are sometimes referred to as the panaxosides, but this nomenclature uses the suffixes A–F, which do not correspond to those of the ginsenosides. In Siberian ginseng (Eleutherococcus), the saponins (eleutherosides A–F) are chemically different, but have similar properties. Glycans (panaxans) also occur in P. ginseng. The actual composition of ginseng extracts depends upon the species and method of preparation.
Therapeutic uses and available evidence
Ginseng is taken as a tonic for debility, insomnia, natural and premature ageing, to increase alertness and improve sexual inadequacy, and for diabetes, as well as an adaptogen to relieve stress and improve stamina and concentration. It has been suggested that these effects are due to changes in cholinergic activity and also neuro-protection, as well as antioxidant activity (Wang et al 2007). The adaptogenic effect may be due to the elevation of serum levels of corticosteroids and the reduction of catecholamines, which results in homoeostasis. Ginsenoside Rb1 acts as a central nervous system sedative and Rg1 has antifatigue and stimulant properties. In animals, an extract increases the capacity of skeletal muscle to oxidize free fatty acids in preference to glucose to produce cellular energy, which would support the antifatigue activity seen in conventional exhaustion tests. Ginseng also has a traditional use in diabetes, and the glycans (panaxans A–E) are hypoglycaemic in mice. Other documented effects include immunomodulatory activity, potentiation of analgesia and anticancer effects (by ginsenosides Rs3 and Rs4).
Trials of ginseng for improving ‘quality of life’, including mental health parameters, show beneficial effects for up to 8 weeks of treatment, but as far as cognition is concerned, a recent Cochrane review concludes that further, better quality studies are needed (Geng et al 2010). Since that review, the results of a placebo-controlled, double-blind, randomized, crossover study assessing the effects of Panax ginseng on subjective mood and aspects of ’working’ memory processes in healthy young adults, following both single dose and sub-chronic (7 days) ingestion, has been published. Dose-related treatment effects were found: 200 mg slowed a fall in mood, but also slowed responding on a mental arithmetic task across day 1, whereas the 400 mg dose also improved calmness (restricted to day 1) and improved mental arithmetic across days 1 and 8. No evidence of additional benefits, nor attenuation of acute effects, was found with repeated ingestion (Reay et al 2010). The dose is very variable but, in general, for a short course in the young and healthy, 0.5–1 g daily is recommended for up to 20 days; for long-term treatment in the sick or elderly, 0.4–0.8 g daily is more usual. Ginseng is taken widely, and side effects are well documented. They include oestrogenic effects, hypertension and irritability. A ‘ginseng abuse’ syndrome has been described.
Lingzhi or reishi mushroom, ganoderma spp
Therapeutic uses and available evidence
Lingzhi is used as an adaptogen and general tonic, in the hope of prolonging life, retarding ageing and generally improving wellbeing and mental faculties. The most common indication is to enhance the immune system, and various animal and clinical studies support such a use. More recently, reishi has been applied as an adjunctive treatment to chemotherapy and radiation in cancer patients, to support immune resistance. The active principles are considered to be the triterpenes and polysac-charides. Extracts inhibit angiotensin-converting enzyme and produce hypotensive effects; cholesterol-lowering effects have been seen in animals. It is also a sedative, liver protectant and cholesterol-lowering agent (for review, see Sanodiya et al 2009). Clinical studies to support the uses are few and some are of doubtful quality.
Rosenroot, rhodiola rosea L. (rhodiolae roseae rhizoma)
Therapeutic uses and available evidence
Rhodiola rhizome preparations exhibit adaptogenic effects, and these include neuroprotective, cardioprotective, anti-fatigue, antidepressive, anxiolytic and CNS stimulating activity. A number of small clinical trials demonstrate that repeated administration of a Rhodiola rosea extract (SHR-5) may exert an anti-fatigue effect and increase mental performance in healthy subjects (measured as an ability to concentrate), and reduce burnout in patients with mild fatigue syndrome. Rhodiola may help in mild to moderate depression and generalized anxiety. Mechanisms of action which may contribute to the clinical effect include interactions with the HPA-system (reducing cortisol levels) and defense mechanism proteins (some heat shock proteins). It does not seem to interact with other drugs and appears to be safe, with only minor adverse effects. For review, see Panossian et al 2010, Panossian and Wikman 2009.
Schisandra, schisandra chinensis (turcz.) baill. (schisandrae chinensis fructus)
Constituents
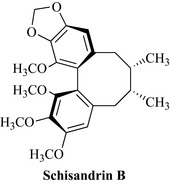
The active constituents are lignans, including schizandrin A (= deoxyschisandrin or wuweizu A), schizandrin B (= wuweizu B or γ-schizandrin B; Fig. 25.3), schizandrol A (= schizandrin), schizandrol B (= gomisin A), schisandrin C, schisantherin A (= gomisin C), schisantherin B (= gomisin B), gomisins H, K, L, M, N, schizanhenol, wuweizu C, schisantherin C and others.
Therapeutic uses and available evidence
Schisandra has been used in China since ancient times to prolong life and increase energy (‘qi’) and act as a general and sexual tonic, especially for men. It is also used to reduce sweating, detoxify the liver, enhance kidney function and suppress cough in lung disease. The adaptogenic and antifatigue properties have been tested in several animal studies; for example, the effect on the physical recovery of racehorses was found to be beneficial, as well as producing a general improvement in performance. Schizanhenol and schizandrin B protect against peroxidative damage associated with ageing and ischaemia in the rat brain, and a human study has suggested that intellectual activity can be enhanced. Many pharmacological studies support the use of schisandra, although few good clinical trials have been performed. Hepatoprotective effects have been documented in animal and cell culture studies. Schizandrin B, schisandrin C and gomisin A reduced liver enzyme levels and prevented histological damage in experimental models of liver injury, inhibited lipid peroxidation and stimulated glycogen synthesis in the liver. Antioxidant and free radical scavenging effects have also been described in vivo and in vitro. Deoxyschisandrin, gomisin A, B and C increase liver cytochrome P450 enzymes, which supports the detoxifying and anticancer properties attributed to the plant. Antitumour-promoting and antiinflammatory properties have also been shown in skin and the lignans are known to be platelet activating factor antagonists. For review, see Panossian and Wikman (2008, 2009). Daily doses of powdered berry are usually 1.5–6 g or higher if used to treat kidney disease.
Constituents
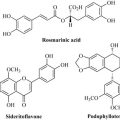
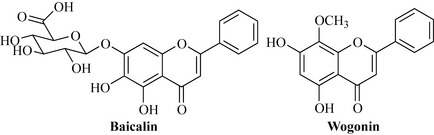
The root contains flavonoids including baicalin, baicalein, wogonin, chrysin, oroxylin A, skullcapflavones I and II, and others (Fig. 25.4).
Therapeutic uses and available evidence
Skullcap is used for a wide variety of ailments, particularly fevers, infections, jaundice, thirst and nosebleeds, and as an antidote and sedative. Baicalin is antiinflammatory and anti-allergic; it inhibits the formation of lipoxygenase products and, to a lesser extent, cyclo-oxygenase products in leukocytes. It also inhibits the generation of inflammatory cytokines and is synergistic with β-lactam antibiotics against methicillin-resistant Staphylococcus aureus in vitro. Extracts of S. baicalensis inhibit lipid peroxidation in rat liver and the herb has been clinically tested in China in patients with chronic hepatitis, where it improved symptoms in over 70% of patients, increasing appetite, relieving abdominal distension and improving the results of liver function tests. Wogonin also suppresses production of hepatitis B virus surface antigen. The flavones interact with the benzodiazepine-binding site of the GABAA receptor, with wogonin and baicalein being the most potent; this supports the sedative use of the herb. Baicalein is antigenotoxic in vitro and inhibits adhesion molecule expression induced by thrombin and cell proliferation of several types of cells. Wogonin inhibits nitric oxide production in activated C6 rat glial cells, acting via NF-κB inhibition and thus suppressing cell death. It also reduces skin inflammation in mice (induced by phorbol ester expression of COX-2) and inhibits monocyte chemotactic protein-1 gene expression in human endothelial cells. Antioxidant and antibiotic activities have also been reported for extracts. These activities all support the antiinflammatory and other uses of skullcap, although clinical trial evidence is sparse (for review, see Li-Weber 2009, Wang et al 2007). The daily dose of skullcap root is usually 5–8 g. Generally, baical skullcap is well tolerated, but little information as to side effects and contraindications is available.
Tea, camellia sinensis (L.) kuntze (green tea leaves: theae viridis folium; black tea leaves: theae nigrae folium)
Constituents
Tea contains caffeine, and much smaller amounts of other xanthines such as theophylline and theobromine. The polyphenols are the antioxidant constituents [in green tea these are mainly (−)-epigallocatechin; Fig. 25.5], together with theogallin, trigalloyl glucose. In black tea, they have been oxidized to form the ‘tea pigments’, the theaflavins, thearubigens and theaflavic acids.
Therapeutic uses and available evidence
Tea is a stimulant, diuretic, astringent and antioxidant. Green tea is used medicinally more frequently than black tea. The stimulant and diuretic properties are due to the caffeine content, and the astringency and antioxidant effects to the polyphenols (Wang et al 2007).
Tea is useful in diarrhoea, and in China is used for many types of dysentery. The polyphenols in green tea have cancer chemopreventive properties due to their antioxidant capacity. Habitual consumption of green tea is generally associated with a lower incidence of cancer (for review, see Lambert and Elias 2010) and black tea is now known to have similar health benefits, which are ascribed to the tea pigments (for review, see Kumar et al 2010). Anti-inflammatory and antitumour effects have been described, and attributed to inhibition of the transcription factor NF-κB, and the risk of breast and stomach cancers appears to be lower for green tea drinkers. Black tea consumption is associated with a lower risk of death from ischaemic heart disease and has been shown to reverse endothelial dysfunction in coronary heart disease. Tea is also antimicrobial and anticariogenic, and is even reputed to help weight loss. Tea is drunk in nearly every country in the world for its refreshing, mildly stimulating and analgesic effects. There is no recommended dose for tea, and consumption varies widely.
Tea as a beverage is non-toxic in the usual amounts ingested, although it can cause gastrointestinal upsets and nervous irritability, due to the caffeine content. However there is now some concern about the safety of concentrated preparations or excessive consumption of green tea. Cases of hepatotoxicity have been associated with consumption of high doses of green tea-containing dietary supplements (10–29 mg/kg/d p.o.). In most cases, patients presented with elevated serum alanine aminotransferase (ALT) and bilirubin levels and in some cases liver biopsies were performed, and periportal and portal inflammation were observed. All cases resolved following cessation of supplement consumption, and re-injury was observed in some studies when the subject began reusing the same preparations, suggesting a causative effect of the green tea. There is also a case report of a 45-year-old man who developed jaundice and elevated serum ALT following consumption of 6 cups/d green tea infusion for 4 months (reviewed by Mazzanti et al 2009).
Bhattarai J.P., Ah Park S., Han S.K. The methanolic extract of Withania somnifera acts on GABAA receptors in gonadotropin releasing hormone (GnRH) neurons in mice. Phytother. Res.. 2010;24:1147-1150.
Cerella C., Sobolewski C., Dicato M., Diederich M. Targeting COX-2 expression by natural compounds: a promising alternative strategy to synthetic COX-2 inhibitors for cancer chemoprevention and therapy. Biochem. Pharmacol.. 2010;80:1801-1815.
Geng J., Dong J., Ni H., et al. Ginseng for cognition. Cochrane Database Syst. Rev. 12, 2010. CD007769
Gullett N.P., Ruhul Amin A.R., Bayraktar S., et al. Cancer prevention with natural compounds. Semin. Oncol.. 2010;37:258-281.
Haleagrahara N., Ponnusamy K. Neuroprotective effect of Centella asiatica extract (CAE) on experimentally induced parkinsonism in aged Sprague-Dawley rats. J. Toxicol. Sci.. 2010;35:41-47.
Heinrich, M., Dhanji, T., Casselman, I., In press. Açai (Euterpe oleracea Mart.) – a phytochemical and pharmacological assessment of the species’ health claims. Phytochemistry Letters 4: 10–21. doi: 10.1016/j.phytol.2010.11.005
Kulkarni S.K., Dhir A. Withania somnifera: an Indian ginseng. Prog. Neuropsychopharmacol. Biol. Psychiatry. 2008;32:1093-1105.
Kumar G., Pillare S.P., Maru G.B. Black tea polyphenols-mediated in vivo cellular responses during carcinogenesis. Mini Rev. Med. Chem.. 2010;10:492-505.
Lambert J.D., Elias R.J. The antioxidant and pro-oxidant activities of green tea polyphenols: a role in cancer prevention. Arch. Biochem. Biophys.. 2010;501:65-72.
Li-Weber M. New therapeutic aspects of flavones: the anticancer properties of Scutellaria and its main active constituents Wogonin, Baicalein and Baicalin. Cancer Treat. Rev.. 2009;35:57-68.
Mato L., Wattanathorn J., Muchimapura S., et al. Centella asiatica improves physical performance and health-related quality of life in healthy elderly volunteer. Evidence-based Complementary and Alternative Medicine. 2009. [Epub ahead of print 2009 Oct 30]
Mazzanti G., Menniti-Ippolito F., Moro P.A., et al. Hepatotoxicity from green tea: a review of the literature and two unpublished cases. Eur. J. Clin. Pharmacol.. 2009;65:331-341.
Nasir M.N., Habsah M., Zamzuri I., Rammes G., Hasnan J., Abdullah J. Effects of asiatic acid on passive and active avoidance task in male Spraque-Dawley rats. J. Ethnopharmacol.. 2011;134:203-209.
Panossian A., Wikman G. Pharmacology of Schisandra chinensis Bail.: An overview of Russian research and uses in medicine. J. Ethnopharmacol.. 2008;118:183-212.
Panossian A., Wikman G. Evidence-based efficacy of adaptogens in fatigue, and molecular mechanisms related to their stress-protective activity. Current Clinical Pharmacology. 2009;4:198-219.
Panossian A., Wikman G., Sarris J. Rosenroot (Rhodiola rosea): traditional use, chemical composition, pharmacology and clinical efficacy. Phytomedicine. 2010;17:481-493.
Sanodiya B.S., Thakur G.S., Baghel R.K., Prasad G.B., Bisen P.S. Ganoderma lucidum: a potent pharmacological macrofungus. Curr. Pharm. Biotechnol.. 2009;10:717-742.
Reay J.L., Scholey A.B., Kennedy D.O. Panax ginseng (G115) improves aspects of working memory performance and subjective ratings of calmness in healthy young adults. Hum. Psychopharmacol.. 2010;25:462-471.
Shu L., Cheung K.L., Khor T.O., Chen C., Kong A.N. Phytochemicals: cancer chemoprevention and suppression of tumor onset and metastasis. Cancer Metastasis Rev.. 2010;29:483-502.
Wang C.Z., Mehendale S.R., Yuan C.S. Commonly used antioxidant botanicals: active constituents and their potential role in cardiovascular illness. Am. J. Chin. Med.. 2007;35:543-558.