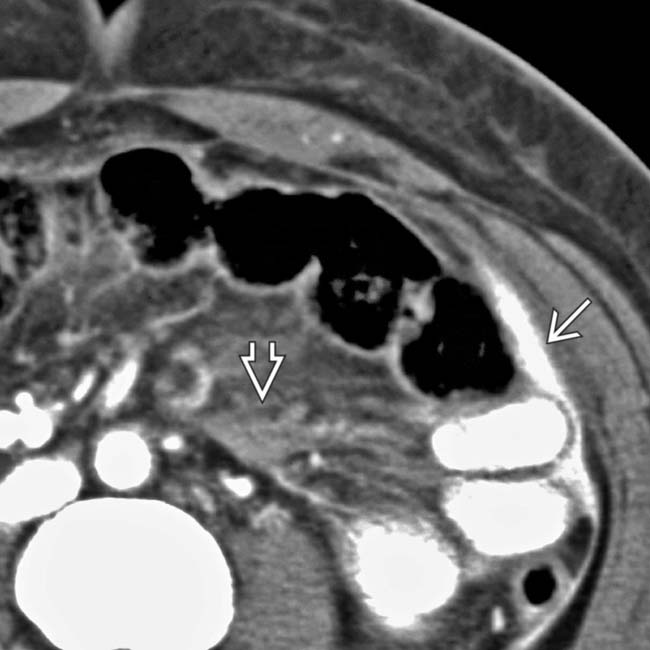
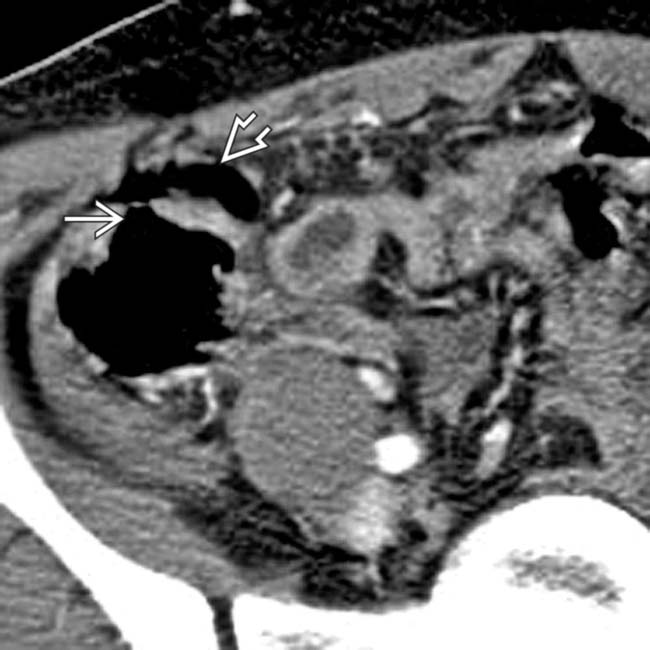
[level-membership-for-radiology-category] Polygonal fluid collections between folds of mesentery, bowel loops





 , adjacent to thick-walled jejunum, and active bleeding, as evidenced by the contrast extravasation
, adjacent to thick-walled jejunum, and active bleeding, as evidenced by the contrast extravasation  . All characteristic findings in intestinal trauma.
. All characteristic findings in intestinal trauma.
 . The mesenteric injury was surgically repaired and a segment of small intestine was resected.
. The mesenteric injury was surgically repaired and a segment of small intestine was resected.
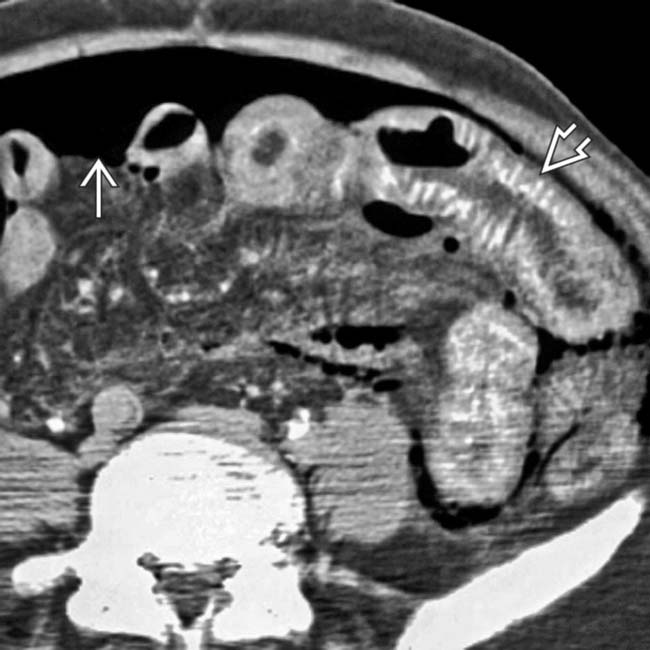
 adjacent to a thick-walled jejunal segment
adjacent to a thick-walled jejunal segment  , indicative of transmural laceration or perforation.
, indicative of transmural laceration or perforation.
 , a characteristic finding in the setting of intestinal trauma.
, a characteristic finding in the setting of intestinal trauma.IMAGING
General Features






CT Findings



• Intra-/retroperitoneal free fluid: Hemoperitoneum or bowel contents





































CLINICAL ISSUES
Presentation


























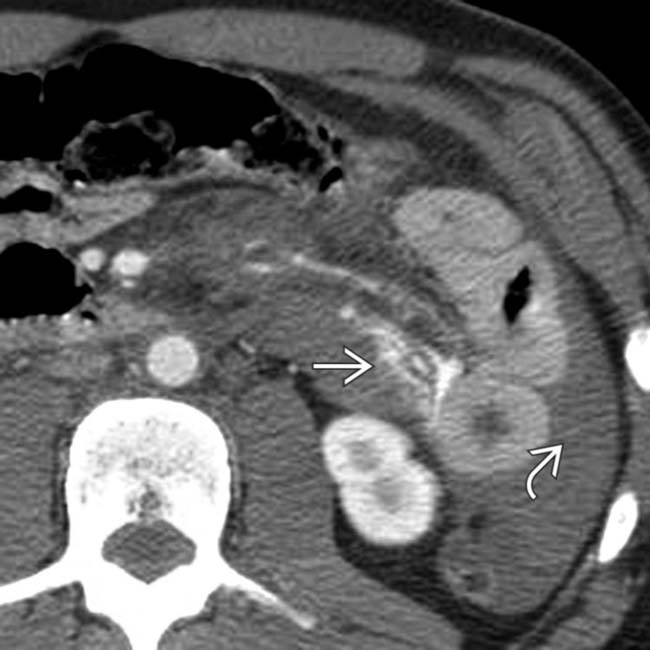
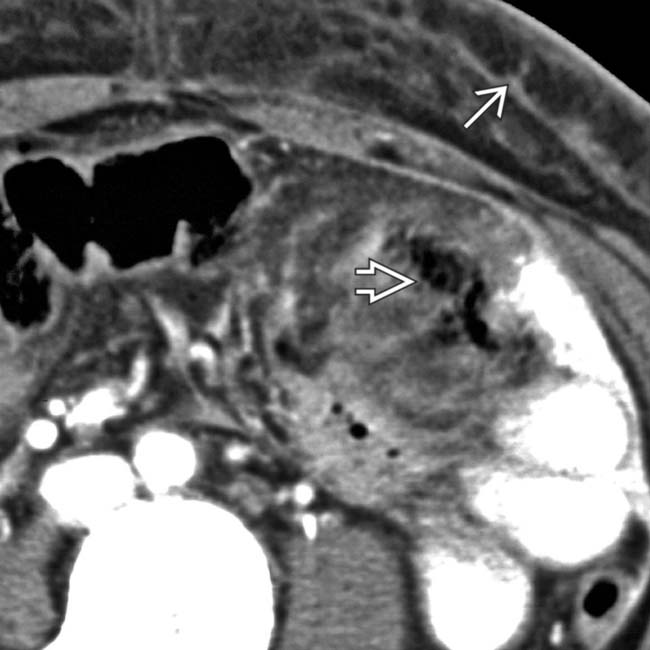
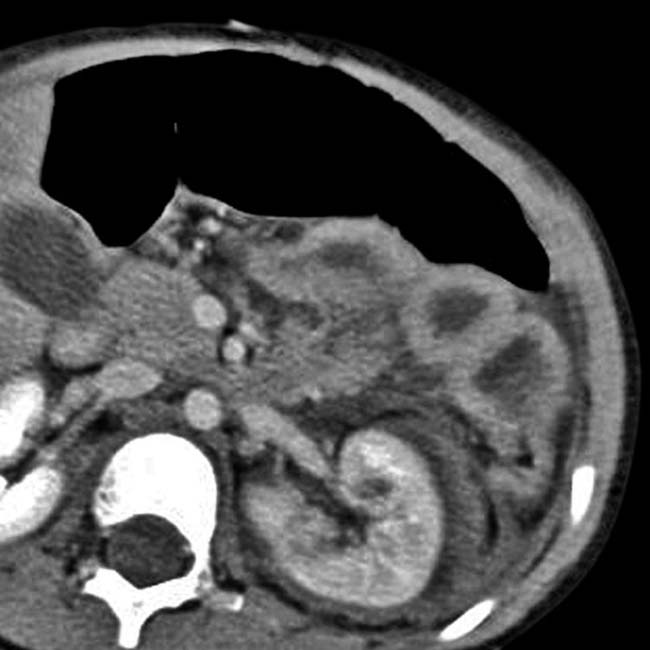
 , hyperdense thickened bowel wall
, hyperdense thickened bowel wall  , and infiltrated mesentery consistent with a hematoma
, and infiltrated mesentery consistent with a hematoma  . Jejunal perforation was revealed at surgery.
. Jejunal perforation was revealed at surgery.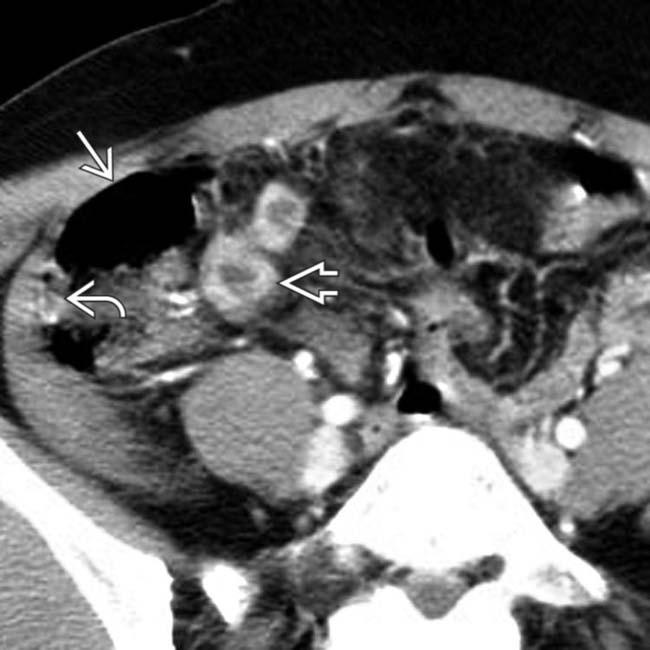
 adjacent to the thickened and collapsed cecum
adjacent to the thickened and collapsed cecum  . Note adjacent bowel wall thickening
. Note adjacent bowel wall thickening  of the terminal ileum. Cecal and distal ileal perforations were confirmed at surgery.
of the terminal ileum. Cecal and distal ileal perforations were confirmed at surgery.
 and a sentinel clot from a mesenteric laceration. A torn mesenteric artery was revealed at surgery, but no bowel injury.
and a sentinel clot from a mesenteric laceration. A torn mesenteric artery was revealed at surgery, but no bowel injury.
 within an interloop compartment. Note the angular margins of the mesenteric collection. There were no signs of bowel injury and the patient recovered without surgery.
within an interloop compartment. Note the angular margins of the mesenteric collection. There were no signs of bowel injury and the patient recovered without surgery.
 . Seat belt contusions are highly associated with bowel and mesenteric injuries.
. Seat belt contusions are highly associated with bowel and mesenteric injuries.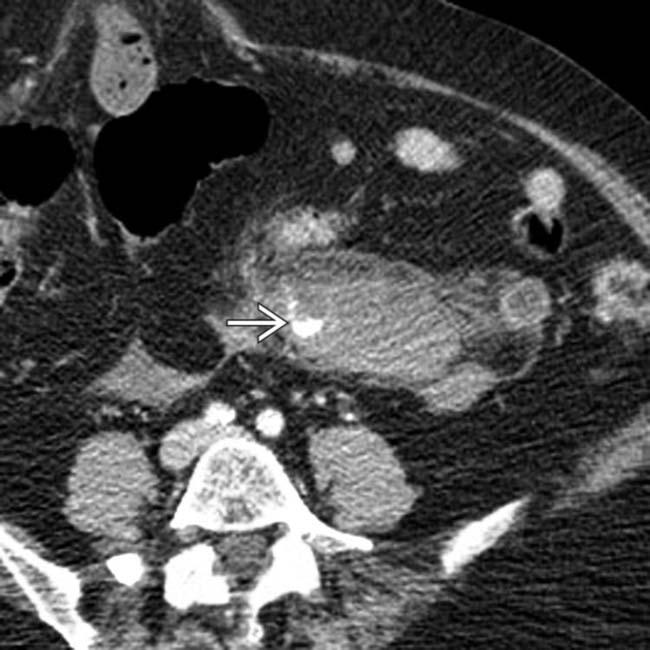
 within a mesenteric hematoma. The adjacent bowel was also found to be injured at surgery. Active mesenteric bleeding from trauma generally demands surgical intervention.
within a mesenteric hematoma. The adjacent bowel was also found to be injured at surgery. Active mesenteric bleeding from trauma generally demands surgical intervention.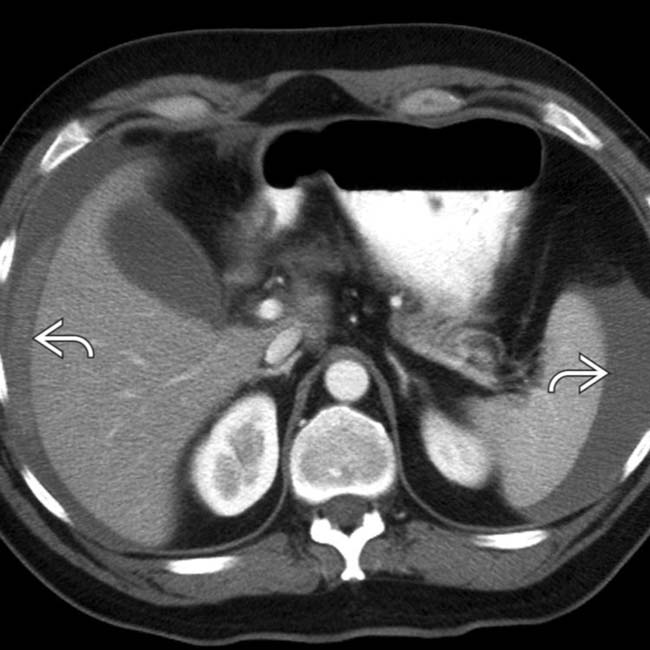
 (45-50 HU) in the upper abdomen without an apparent hepatic or splenic injury.
(45-50 HU) in the upper abdomen without an apparent hepatic or splenic injury.
 and left paracolic
and left paracolic  collections. Mesenteric laceration without bowel injury was confirmed at surgery.
collections. Mesenteric laceration without bowel injury was confirmed at surgery.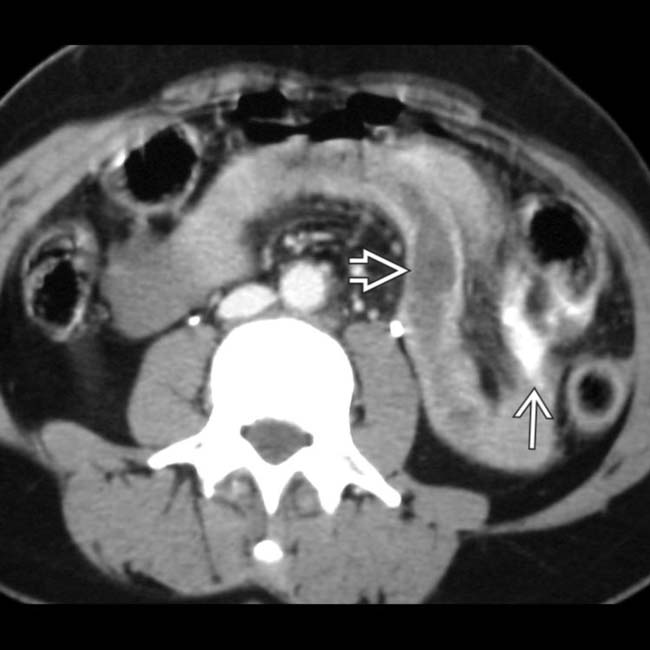
 and active bleeding
and active bleeding  into the mesentery, with fluid isodense to enhanced blood vessels.
into the mesentery, with fluid isodense to enhanced blood vessels.
 , diagnostic of transmural laceration. The active mesenteric bleeding alone would have warranted surgical intervention in this case.
, diagnostic of transmural laceration. The active mesenteric bleeding alone would have warranted surgical intervention in this case.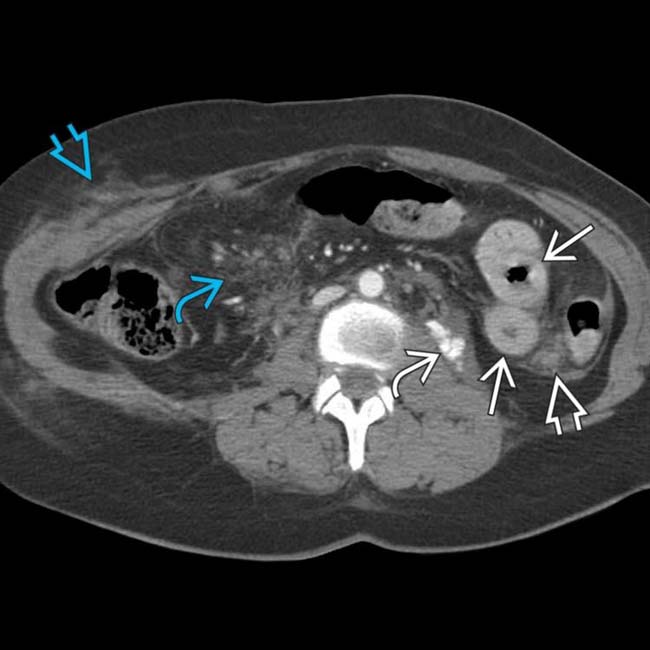
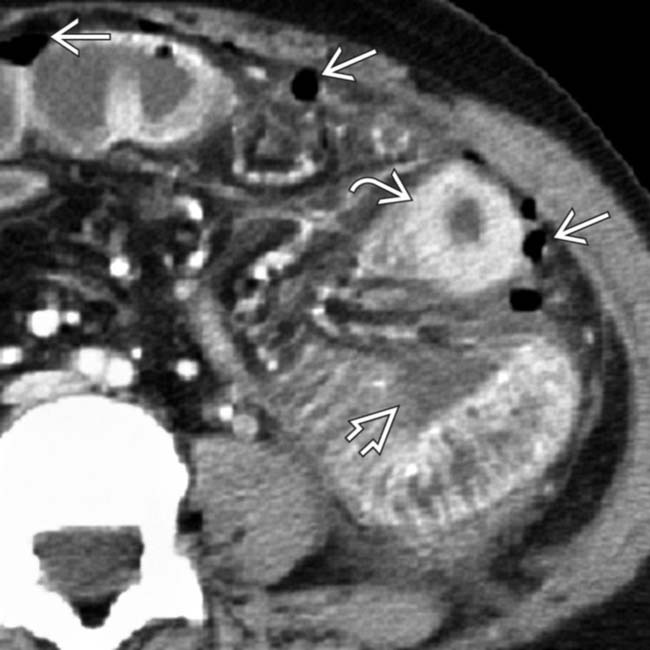
 , hyperenhancing, thickened SB wall
, hyperenhancing, thickened SB wall  , and interloop hematoma
, and interloop hematoma  . Also seen is an abdominal wall hematoma from the seat belt impact
. Also seen is an abdominal wall hematoma from the seat belt impact  and diffuse mesenteric infiltration
and diffuse mesenteric infiltration  .
.
 . At surgery, serosal avulsion and transmural laceration of the small bowel were confirmed.
. At surgery, serosal avulsion and transmural laceration of the small bowel were confirmed.
 .
.
 measuring about 20 HU, likely representing a mixture of blood and extraluminal bowel contents.
measuring about 20 HU, likely representing a mixture of blood and extraluminal bowel contents.
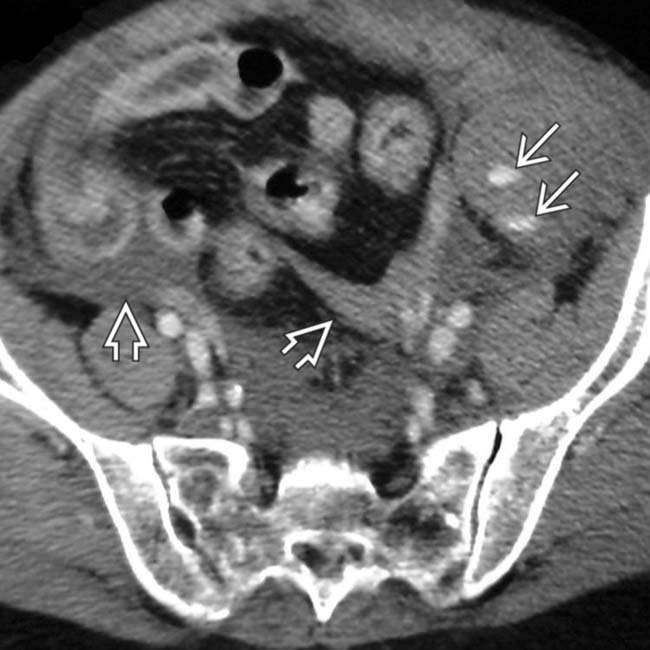
 adjacent to jejunum and cecum, and more free air
adjacent to jejunum and cecum, and more free air  .
.
 . No solid visceral injuries were evident.
. No solid visceral injuries were evident.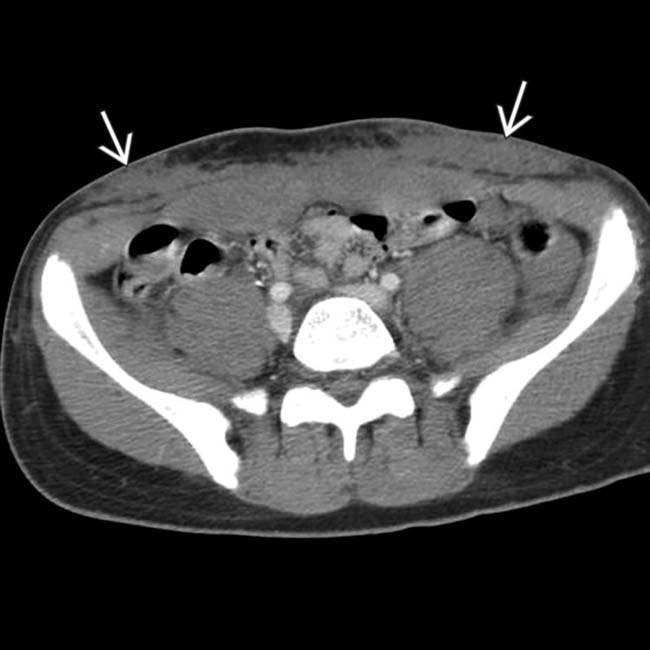
 in the subcutaneous fat of the abdominal wall at the level of the iliac crests. This is a classic seat belt sign.
in the subcutaneous fat of the abdominal wall at the level of the iliac crests. This is a classic seat belt sign.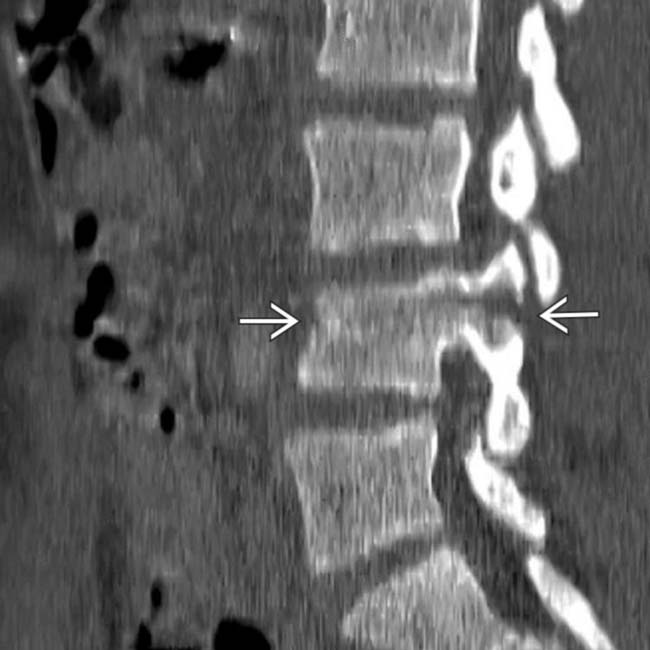
 through the L3 vertebral body and posterior elements, a classic Chance fracture. This and the seat belt contusion are highly associated with bowel and mesenteric injuries. Jejunal and cecal lacerations were confirmed at surgery.
through the L3 vertebral body and posterior elements, a classic Chance fracture. This and the seat belt contusion are highly associated with bowel and mesenteric injuries. Jejunal and cecal lacerations were confirmed at surgery.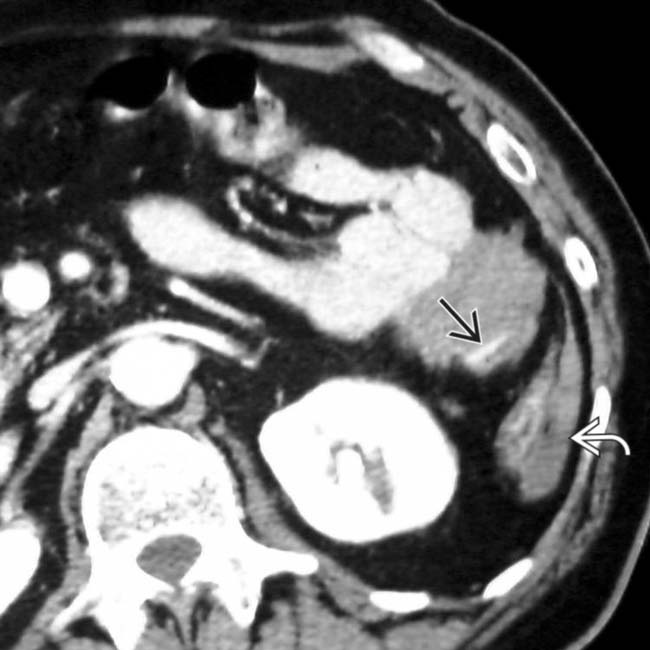
 in mesentery and blood in the left paracolic gutter
in mesentery and blood in the left paracolic gutter  .
.
 . Also note the “triangular” and interloop collections of blood
. Also note the “triangular” and interloop collections of blood  , another sign of bowel or mesenteric injury.
, another sign of bowel or mesenteric injury.
 .
.
 .
.
 associated with a mesenteric hematoma
associated with a mesenteric hematoma  .
.
 from a seat belt injury and pneumoperitoneum
from a seat belt injury and pneumoperitoneum  .
.
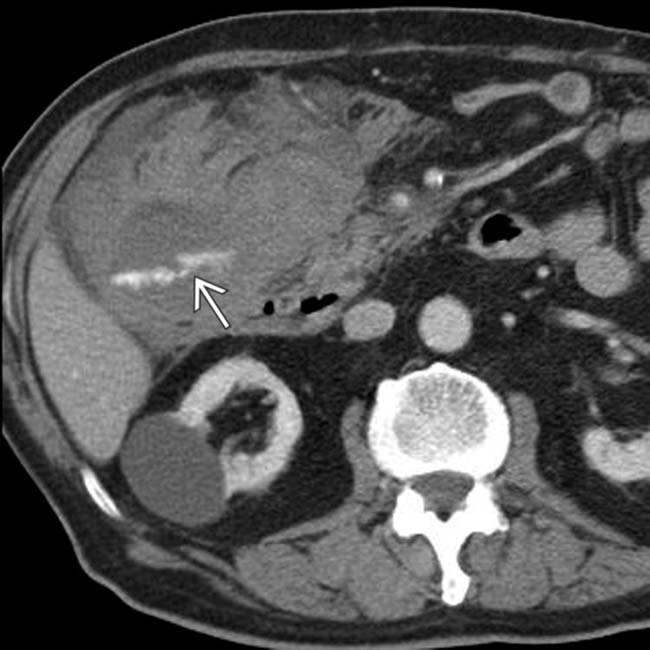
 surrounded by a large hematoma
surrounded by a large hematoma  .
.
 . At surgery, a right hemicolectomy was required to stop bleeding.
. At surgery, a right hemicolectomy was required to stop bleeding.
 , water density in the left paracolic gutter
, water density in the left paracolic gutter  , and an intraloop compartment
, and an intraloop compartment  .
.
 . Note the hyperdense small bowel with visualization of the vasa recta in the thickened bowel wall
. Note the hyperdense small bowel with visualization of the vasa recta in the thickened bowel wall  from a reperfusion injury.
from a reperfusion injury.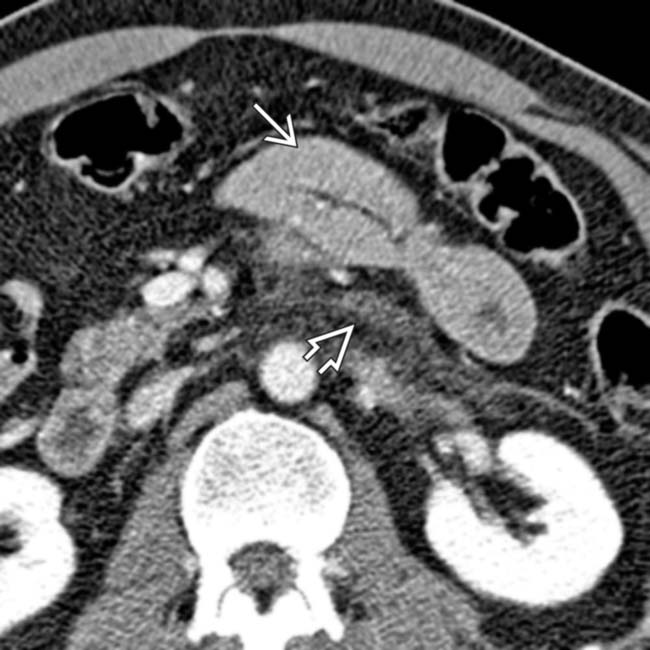
 with adjacent mesenteric hematoma
with adjacent mesenteric hematoma  .
.
 . Adjacent ectopic gas is present
. Adjacent ectopic gas is present  , confirming perforation.
, confirming perforation.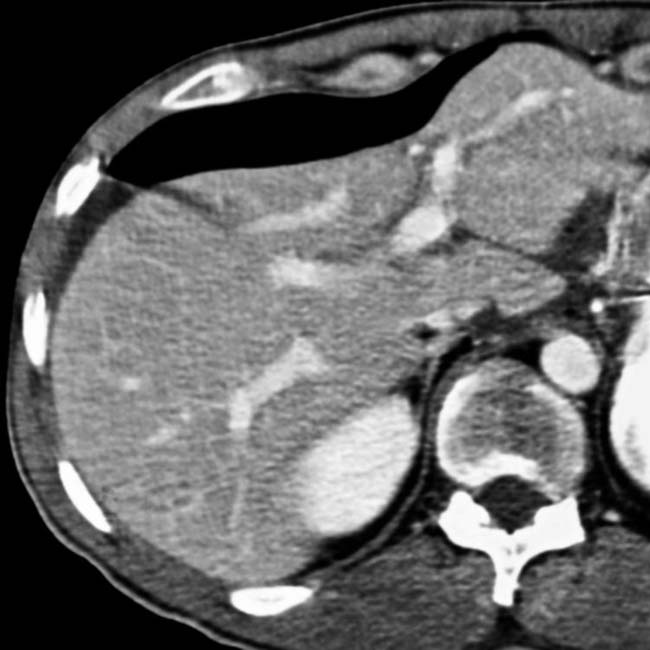

 in this transected small bowel.
in this transected small bowel.
 from jejunal transection.
from jejunal transection.
 , mesenteric infiltration, bowel wall thickening, and free air
, mesenteric infiltration, bowel wall thickening, and free air  in this jejunal transection.
in this jejunal transection.

 , and 2 sites of active mesenteric bleeding
, and 2 sites of active mesenteric bleeding  .
.
[/level-membership-for-radiology-category][not-level-membership-for-radiology-category] Polygonal fluid collections between folds of mesentery, bowel loops
, adjacent to thick-walled jejunum, and active bleeding, as evidenced by the contrast extravasation . All characteristic findings in intestinal trauma.. The mesenteric injury was surgically repaired and a segment of small intestine was resected. adjacent to a thick-walled jejunal segment , indicative of transmural laceration or perforation., a characteristic finding in the setting of intestinal trauma.IMAGING
General Features
CT Findings
• Intra-/retroperitoneal free fluid: Hemoperitoneum or bowel contents
DIFFERENTIAL DIAGNOSIS
Shock Bowel
Coagulopathy
• Barium studies, CT of SB
 Uniform, regular thickening of valvulae conniventes with symmetric, spike-like configuration, decreased luminal diameter simulating “stack of coins”
Uniform, regular thickening of valvulae conniventes with symmetric, spike-like configuration, decreased luminal diameter simulating “stack of coins”
Uniform, regular thickening of valvulae conniventes with symmetric, spike-like configuration, decreased luminal diameter simulating “stack of coins”Buy Membership for Radiology Category to continue reading. Learn more here
[/not-level-membership-for-radiology-category]
