Chapter 135 Melanocytoma of the Optic Disc
General considerations
Melanocytoma of the optic disc, a lesion best known to ophthalmologists, has received considerable attention in the literature.1–38 Since the last edition of this textbook, there have been only a few noteworthy publications in the English language literature related to this tumor.20,34–38 Most statistical information on optic disc melanocytoma was derived from a review of 115 patients from one center, which elucidated statistically the clinical variations and chances of visual loss, tumor growth, and malignant transformation.18
The term melanocytoma was originally coined by Zimmerman to describe a tumor with specific clinical and pathological features that was located partly or completely within the optic nerve head.30–32 Since the clinical and histopathologic nature of this lesion was clarified by Zimmerman and Garron,32 tumors of similar type have been recognized in extrapapillary locations throughout the uveal tract.20,21 Melanocytoma is now best defined as a specific variant of melanocytic nevus, located in the optic disc or anywhere in the uveal tract, characterized clinically by a dark brown to black color, and composed histopathologically of deeply pigmented round to oval cells with small, round, uniform nuclei.
Historically, melanocytoma was often confused clinically and histopathologically with uveal malignant melanoma.4,31,32 An important difference between the two is that melanocytoma appears to have an equal incidence in all races, whereas uveal melanoma is uncommon in black people.20 Furthermore, it is also uncommon for melanoma to be confined to the optic disc or to secondarily invade the optic nerve.
Clinical features
Most melanocytomas do not cause severe visual impairment. However, slight visual loss related to the tumor can occur in about 26%, usually due to mild retinal exudation and subretinal fluid.18 More severe visual loss can rarely occur, secondary to central retinal vein obstruction and/or spontaneous tumor necrosis6,24,28,31,39 or malignant transformation.1,18,20–22 In some cases, such visual loss is reversible with time.28 From 10–30% of patients with optic disc melanocytomas have an afferent pupillary defect (Marcus Gunn pupil) in the involved eye.14,18 This can occur even when the visual acuity is good. It is probably due to compression of the optic nerve fibers by the melanocytoma cells, a factor that also explains the associated visual field defect. Melanocytoma is usually unilateral. Bilateral cases have been rarely reported, usually in children but these cases may not be true melanocytomas.7,17,18,27 There has been some controversy as to whether they should be called true melanocytomas or disc pigmentation in association with other congenital disc abnormalities.2,3,17
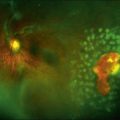
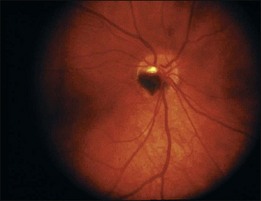
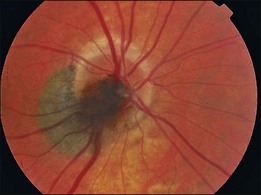
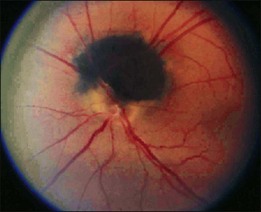
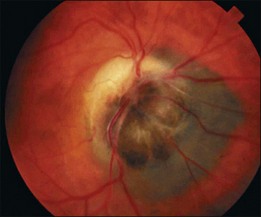
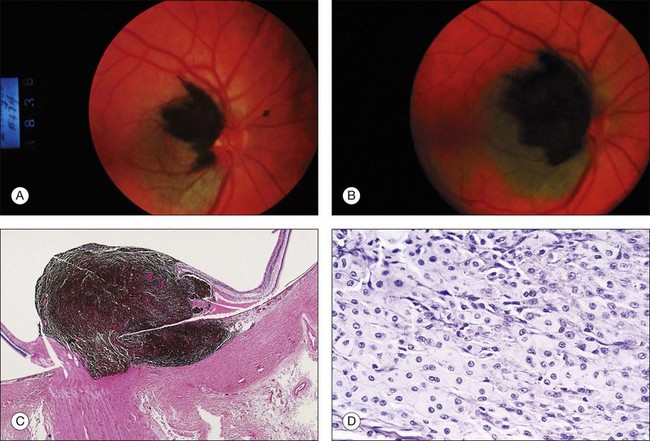
Ophthalmoscopically, optic nerve melanocytoma has typical features.15,20,21,33 It is characteristically a dark brown to black lesion that is located partly in the optic disc. It is relatively small and confined to the disc in 15% (Fig. 135.1). More characteristically, it extends over the margin of the optic disc to involve the adjacent choroid (54%) (Fig 135.2) or into the adjacent sensory retina (30%) (Fig. 135.3).18 In some cases, the choroidal component is more pronounced than the papillary component. Although optic disc melanocytoma is generally believed to have few local complications, a recent study showed that there is some degree of disc edema (25%) (Fig. 135.4), intraretinal edema (16%), subretinal fluid (14%), yellow intraretinal exudation (12%), focal hemorrhage (5%), vitreous seeds (4%), and retinal vein obstruction (3%). These local complications can produce visual symptoms or visual loss in 26% of cases.18 This is generally mild, and severe visual loss is exceptional. Vitreous seeds from necrosis of the melanocytoma can extend into the anterior chamber, sometimes producing a black pseudohypopyon.29 The statistical risk factors for visual loss include retinal extension of the tumor and the presence of subretinal fluid. There have been recent reports of choroidal neovascularization adjacent to optic disc melanocytoma.37,38
Melanocytoma of the optic disc traditionally was recognized to be a stable lesion with no tendency to grow. However, serial fundus photographs have documented that 11–15% of them show subtle enlargement over several years. This mild growth should not be misconstrued as malignant transformation.5,10,18 In one report, an eye with a progressively growing melanocytoma underwent enucleation and the lesion proved to be benign, despite progressive growth.12 Multivariate analysis has shown that the main predictive risk factor for growth is an initial thickness of ≥1.5 mm at the time of first diagnosis.18 Some tumors can grow slowly and produce ischemic optic neuropathy associated with tumor necrosis, resulting in severe visual loss.9,26,28 Others can cause central retinal vein obstruction and visual loss.6,24,30 In rare cases the tumor can present as neovascular glaucoma secondary to retinal vein obstruction.6
There are usually no systemic associations with optic disc melanocytoma. It has been reported in association with intracranial meningioma27 and type 2 neurofibromatosis,23 but it is still uncertain whether such associations are coincidental.
The differential diagnosis of melanocytoma of the optic disc includes juxtapapillary choroidal melanoma, choroidal nevus, hyperplasia of the RPE, hypertrophy of the RPE, and combined hamartoma of the retina and RPE and adenoma of the RPE.20 Although extremely rare, malignant melanoma can occur in the optic nerve and may be difficult to impossible to differentiate clinically from melanocytoma.8 Juxtapapillary adenoma of the RPE can also closely resemble melanocytoma.19 The clinical features of these conditions, described in other chapters, should help to differentiate them from melanocytoma in most instances.
Pathology and pathogenesis
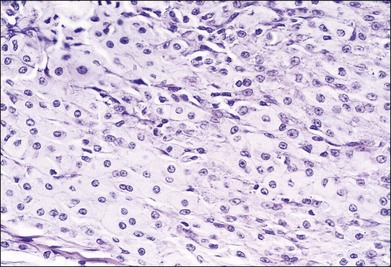
On low-power microscopy, a melanocytoma of the optic nerve has a characteristic appearance. It is a deeply pigmented mass that occupies the optic disc and extends for a variable distance into the optic nerve itself (Fig. 135.5). Cytologically, the most distinguishing characteristics are the dense pigmentation and the uniform appearance. Although the dense pigment prevents visualization of cell detail, bleached preparations reveal the cells to be oval or round with abundant cytoplasm, relatively small nuclei, and few prominent nucleoli, similar to those which occur throughout the uvea in patients with ocular melanocytosis (Fig. 135.6).20,21,30,31 Tumors composed of similar cells have also been recognized in the iris, ciliary body, choroid, and even in the conjunctiva.20,21
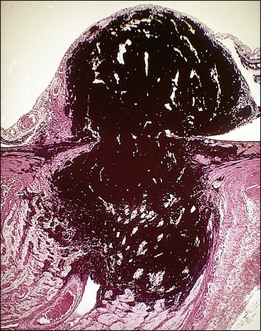
Fig. 135.5 Low magnification photomicrograph of optic disc melanocytoma (H&E ×10).
(Courtesy of Armed Forces Institute of Pathology.)
The pathogenesis of optic disc melanocytoma is unknown. It is generally assumed to be a congenital lesion, but, like most uveal nevi, it is rarely seen in young children. It has developed in an adult fundus that was previously documented photographically to be normal, raising speculation that it is either acquired or occurs as an amelanotic lesion that later becomes pigmented and clinically visible.25
Diagnostic approaches
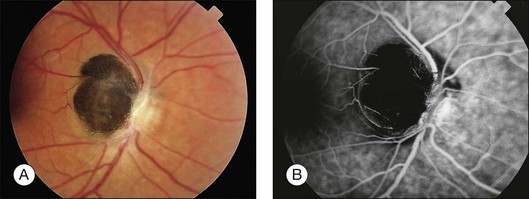
In most cases, fluorescein angiography of a melanocytoma of the optic nerve demonstrates hypofluorescence throughout the angiogram (Fig. 135.7).20,21 This is presumably because the cells are deeply pigmented and closely compact with relatively little vascularity. In cases with optic disc edema, there is hyperfluorescence of the optic disc edema adjacent to the tumor. Indocyanine green angiography also shows the lesion to be generally hypofluorescent.11 Visual fields of eyes with melanocytomas can be variable, depending on the size and extent of the lesion. Visual field defect are relatively common and include arcuate scotoma, enlarged blind spot and others.14,18
If a melanocytoma is greater than 0.5 mm in elevation, it can often be demonstrated with ultrasonography or computed tomography (CT) but these techniques cannot easily differentiate melanocytoma from other elevated lesions of the optic disc. Furthermore, ultrasonography cannot detect microscopic extension of the tumor into the retrolaminar portion of the optic nerve. However, high-resolution ultrasonography has been reported to be of some value in diagnosis.34 Magnetic resonance imaging (MRI) can help determine the extent of melanocytic involvement in the retrolaminar portion of the optic nerve. Extensive involvement in the optic nerve with severe visual loss suggests malignant transformation of the lesion (Fig. 135.8).1,13,16,18,22 Optical coherence tomography has been studied in cases of optic disc melanocytoma, but the findings are not specific.35,36 Malignant change is estimated to occur in about 1–2% of cases.18 Only a few convincing cases of transformation into melanoma with histopathologic confirmation have been reported.1,13,22
1 Apple DJ, Craythorn JM, Reidy JJ, et al. Malignant transformation of an optic nerve melanocytoma. Can J Ophthalmol. 1984;19:320–325. 22
2 Brodsky M. Melanocytoma or congenital optic disc pigmentation. Letter. Am J Ophthalmol. 2004;137:208–209.
3 Brodsky M, Phillips PH. Optic nerve hypoplasia and congenital hypopituitarism. J Pediatr. 2000;136:850.
4 Cordes FC, Hogan MJ. Primary malignant melanoma of the optic disc. Am J Ophthalmol. 1949;32:1037–1047.
5 Costa J, Vargas E, Mendonca AP, et al. Growing optic disc melanocytoma: what to do? Neuro-Ophthalmol. 2002;27:39–43.
6 Croxatto JO, Ebner R, Crovetto L, et al. Angle closure glaucoma as initial manifestation of melanocytoma of the optic disc. Ophthalmology. 1983;90:830–834.
7 Demirci H, Shields CL, Shields JA. Bilateral optic disc melanocytoma in a 10 month old infant. Am J Ophthalmol. 2003;136:190–192.
8 DePotter P, Shields CL, Eagle RC, Jr., et al. Malignant melanoma of the optic nerve. Arch Ophthalmol. 1996;114:608–612.
9 Garcia-Arumi J, Salvador F, Corcostegui B, et al. Neuroretinitis associated with melanocytoma of the optic disc. Retina. 1994;14:173–176.
10 Joffe L, Shields JA, Osher R, et al. Clinical and follow-up studies of melanocytomas of the optic disc. Ophthalmology. 1979;86:1067–1078.
11 Kadayifcilar S, Akman A, Aydin P. Indocyanine green angiography of optic nerve head melanocytoma. Eur J Ophthalmol. 1999;9:68–70.
12 Mansour AM, Zimmerman LE, LaPiana FG, et al. Clinicopathologic findings in a growing optic nerve melanocytoma. Br J Ophthalmol. 1989;73:410–415.
13 Meyer D, Ge J, Blinder KJ, et al. Malignant transformation of an optic disc melanocytoma. Am J Ophthalmol. 1999;127:710–714.
14 Osher RH, Shields JA, Layman PR. Pupillary and visual field evaluation in patients with melanocytoma of the optic disc. Ophthalmology. 1979;97:1096–1099.
15 Reidy JJ, Apple DJ, Steinmetz RL, et al. Melanocytoma: Nomenclature, pathogenesis, natural history and treatment. Surv Ophthalmol. 1985;29:319–327.
16 Sharma PM, Sangal K, Malik P, et al. Malignant transformation of optic disc melanocytoma? A clinical dilemma at presentation with a review of the literature. Ophthalmologica. 2002;216:292–295.
17 Shields JA, Demirci H, Shields CL. Melanocytoma or congenital optic disc pigmentation. Letter. Am J Ophthalmol. 2004;137:209–210.
18 Shields JA, Demirci H, Shields CL, et al. Melanocytoma of the optic disc in 115 cases. The 2004 Samuel Johnson Lecture. Ophthalmology. 2004;111:1739–1746.
19 Shields JA, Eagle RC, Jr., Shields CL, et al. Pigmented adenoma of the optic nerve head simulating a melanocytoma. Ophthalmology. 1992;99:1705–1708.
20 Shields JA, Shields CL, Eagle RC, Jr. Melanocytoma (hyperpigmented magnocellular nevus) of the uveal tract. The 34th G. Victor Simpson Lecture. Retina. 2007;27:730–739.
21 Shields JA, Shields CL. Melanocytoma of the optic disc and posterior retina. Intraocular tumors. Shields JA, Shields CL. An atlas and textbook. Philadelphia: Lippincott Williams and Williams; 2008:324–325.
22 Shields JA, Shields CL, Eagle RC, Jr., et al. Malignant melanoma associated with melanocytoma of the optic disc. Ophthalmology. 1990;97:225–230.
23 Shields JA, Shields CL, Lavrich J. Melanocytoma of optic disc in a patient with type 2 neurofibromatosis. Retina. 2002;22:222–223.
24 Shields JA, Shields CL, Eagle RC, Jr., et al. Central retinal vascular obstruction secondary to melanocytoma of the optic disc. Arch Ophthalmol. 2001;119:129–133.
25 Shields JA, Shields CL, Piccone M, et al. Spontaneous appearance of an optic disc melanocytoma. Am J Ophthalmol. 2002;134:614–615.
26 Usui T, Shirakashi M, Kurosawa A, et al. Visual disturbance in patients with melanocytoma of the optic disc. Ophthalmologica. 1990;201:92–98.
27 Walsh TJ, Packer S. Bilateral melanocytoma of the optic nerve associated with intracranial meningioma. Ann Ophthalmol. 1971;3:885–888.
28 Wiznia RA, Price J. Recovery of vision in association with a melanocytoma of the optic disc. Am J Ophthalmol. 1974;78:236–238.
29 Yamaguchi K, Shiono T, Mizuno K. Pigment deposition in the anterior segment caused by melanocytoma of the optic disc. Ophthalmologica. 1987;194:191–193.
30 Zimmerman LE. Pigmented tumors of the optic nervehead (abstr). Am J Ophthalmol. 1960;50:338.
31 Zimmerman LE. Melanocytes, melanocytic nevi and melanocytomas. Invest Ophthalmol. 1965;4:11–41.
32 Zimmerman LE, Garron LK. Melanocytoma of the optic disc. Int Ophthalmol Clin. 1962;2:431–440.
33 Zografos L, Uffer S, Gailloud C, et al. Le melanome de la papille, nouvelle observation. Klin Manatsbl Augenheilk. 1982;180:503–509.
34 Gologorsky D, Schefler AC, Ehlies FJ, et al. Clinical imaging and high-resolution ultrasonography in melanocytoma management. Clin Ophthalmol. 2010;9:855–859. 4
35 Finger PT, Natesh S, Milman T. Optical coherence tomography: pathology correlation of optic disc melanocytoma. Ophthalmology. 2010;117:114–119.
36 Shields CL, Perez B, Benavides R, et al. Optical coherence tomography of optic disk melanocytoma in 15 cases. Retina. 2008;28:441–446.
37 Chalam KV, Gupta SK, Shah GY, et al. Successful management of melanocytoma-associated choroidal neovascularization with photodynamic therapy. Eur J Ophthalmol. 2006;16:776–778.
38 Tran HV, Bovey EH, Uffer S, et al. Peripapillary choroidal neovascularization associated with melanocytoma of the optic disc: a clinicopathologic case report. Graefes Arch Clin Exp Ophthalmol. 2006;244:1367–1369.
39 Shields JA, Shields CL, et al. Total blindness from presumed optic nerve melanocytoma. Am J Ophthalmol. 2005;139:1113–1114.