[level-membership-for-anesthesiology-category]
22 Mandibular Block
Placement
Anatomy
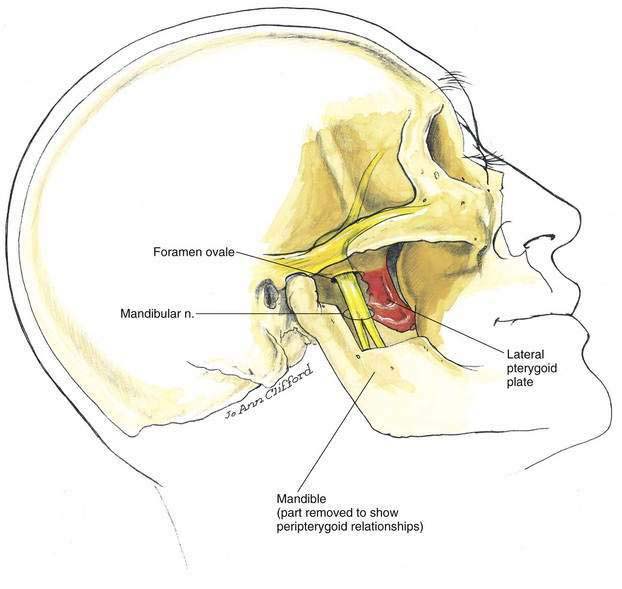
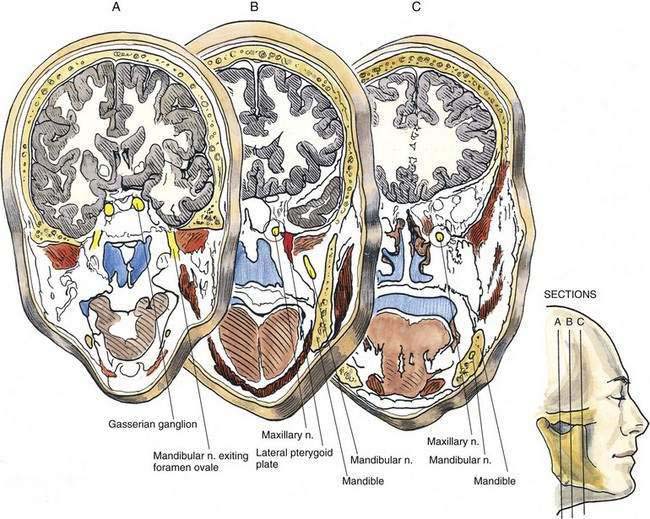
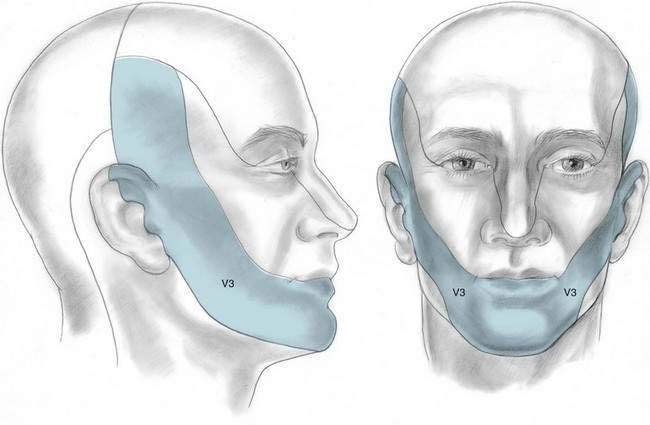
The mandibular nerve is a mixed motor-sensory nerve, although it is primarily sensory. It exits from the cranium through the foramen ovale and parallels the posterior margin of the lateral pterygoid plate as it descends inferiorly and laterally toward the mandible (Figs. 22-1 and 22-2). The anterior division of the mandibular nerve is principally motor and supplies the muscles of mastication, whereas the posterior division is principally sensory and supplies the skin and mucous membranes overlying the lower jaw and skin anterior and superior to the ear (Fig. 22-3).
Needle Puncture
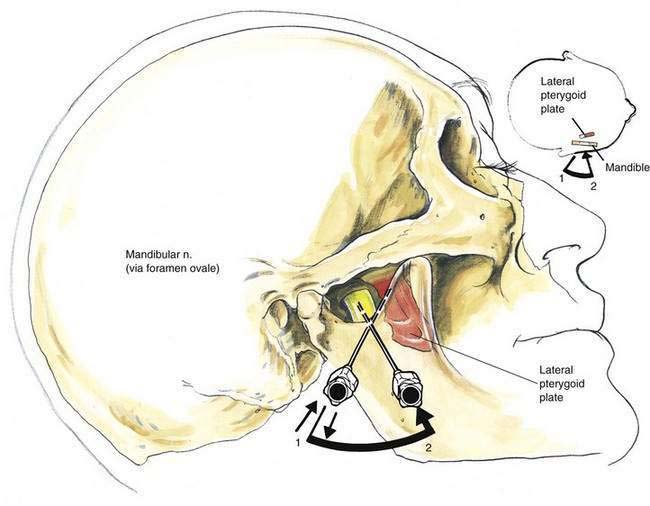
The needle is inserted in the midpoint of the mandibular notch and directed to reach the lateral pterygoid plate by taking a slightly cephalomedial angle through the notch, as shown in Figure 22-4. The 22-gauge, 8-cm needle will impinge on the lateral pterygoid plate at a depth of approximately 5 cm (needle position 1). The needle is then withdrawn and redirected in small steps to “walk off” the posterior border of the lateral pterygoid plate in a horizontal plane (needle position 2), as shown in Figure 22-4. The needle should not be advanced more than 0.5 cm past the depth of the pterygoid plate because the superior constrictor muscle of the pharynx is easily pierced; thus, the needle will enter the pharynx if it is inserted more deeply. Once the needle tip is appropriately positioned, 5 mL of local anesthetic is administered.
[/level-membership-for-anesthesiology-category][not-level-membership-for-anesthesiology-category]
22 Mandibular Block
Placement
Anatomy
The mandibular nerve is a mixed motor-sensory nerve, although it is primarily sensory. It exits from the cranium through the foramen ovale and parallels the posterior margin of the lateral pterygoid plate as it descends inferiorly and laterally toward the mandible (Figs. 22-1 and 22-2). The anterior division of the mandibular nerve is principally motor and supplies the muscles of mastication, whereas the posterior division is principally sensory and supplies the skin and mucous membranes overlying the lower jaw and skin anterior and superior to the ear (Fig. 22-3).
