Chapter 51 Management of Hyperglycemia in the Critically Ill
4 What is the relationship between hyperglycemia and acute illness?
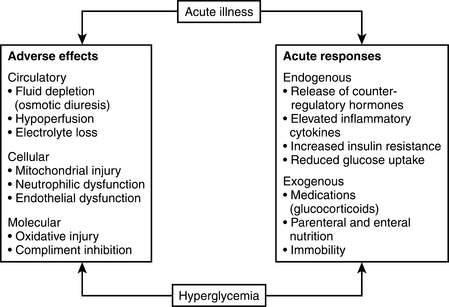
The relationship between hyperglycemia and acute illness is complex. Severe hyperglycemia (>250 mg/dL) has been shown to have a negative impact on the vascular, hemodynamic, and immune systems. Hyperglycemia can also lead to electrolyte imbalance, mitochondrial injury, and both neutrophil and endothelial dysfunction. Acute illness increases the risk for hyperglycemia through the release of counterregulatory hormones, increased insulin resistance, and immobility. Figure 51-1 illustrates the relationship between acute illness and hyperglycemia.
9 What is the appropriate glycemic target for critically ill patients?
Recognizing the importance of glycemic control in critically ill patients, a number of professional societies have developed treatment guidelines and/or consensus statements that provide evidence-based glycemic targets. Although the glycemic targets are not identical, all of the groups advocate for good glycemic control while avoiding hypoglycemia (see Table 51-1).
Table 51-1 Summary of glycemic targets from the medical literature
| Professional society/consensus statement | Glycemic target for critically ill patients |
|---|---|
| American Diabetes Association | 140-180 mg/dL |
| American Association of Clinical Endocrinologists | 140-180 mg/dL |
| Surviving Sepsis Campaign | 150-180 mg/dL |
| American College of Physicians | 140-200 mg/dL |
| American Thoracic Society | <180 mg/dL (in patients undergoing cardiac surgery) |
12 How should patients be transitioned from an intravenous insulin infusion to subcutaneous insulin therapy?
16 Is intensive treatment of hyperglycemia cost-effective?
Key Points Management of hyperglycemia in critically ill patients
1. Hyperglycemia is common in critically ill patients and has been independently associated with increased ICU mortality.
2. Oral medications and noninsulin injectable therapies should not be used to treat hyperglycemia in critically ill patients.
3. An intravenous insulin infusion is the safest and most effective way to treat hyperglycemia in critically ill patients.
4. A glycemic target of 140 to 180 mg/dL is recommended for critically ill patients.
5. Early recognition and treatment of mild hypoglycemia can prevent the adverse outcomes associated with severe hypoglycemia.
1 Clement S., Braithwaite S., Magee M., et al. Management of diabetes and hyperglycemia in hospitals. Diabetes Care. 2004;27:856.
2 Cryer P., Davis S., Shamoon H. Hypoglycemia in diabetes. Diabetes Care. 2003;26:1902–1912.
3 Dellinger R., Levy M., Carlet J., et al. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock. Crit Care Med. 2008;36:1394–1396.
4 Egi M., Bellomo R., Stachowski E., et al. Hypoglycemia and outcomes in critically ill patients. Mayo Clin Proc. 2010;85:217–224.
5 Egi M., Finfer S., Bellomo R. Glycemic control in the ICU. Chest. 2011;140:212–220.
6 Finfer S., Chittock D., Su S., et al. Intensive versus conventional glucose control in critically ill patients. N Engl J Med. 2009;360:1283–1297. NICE-SUGAR Study Investigators;
7 Insucchi S. Management of hyperglycemia in the hospital setting. N Engl J Med. 2006;355:1903–1911.
8 Lazar H., McDonnnell M., Chipkin S., et al. The Society of Thoracic Surgeons practice guideline series: blood glucose management during adult cardiac surgery. Ann Thorac Surg. 2009;87:663–669.
9 Levetan C., Salas J., Wilets I., et al. Impact of endocrine and diabetes team consultation on hospital length of stay for patients with diabetes. Am J Med. 1995;99:22–28.
10 McCowen K., Malhotra A., Bistrian B. Stress-induced hyperglycemia. Crit Care Clin. 2001;17:107–124.
11 Moghissi E., Korytkowski M., DiNardo M., et al. AACE/ADA consensus statement on inpatient glycemic control. Endocr Pract. 2009;15(4):1–17.
12 Qaseem A., Humphrey L.L., Chou R., et al. Use of intensive insulin therapy for the management of glycemic control in hospitalized patients: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2011;154:260–267.
13 Umpierrez G., Smiley M., Zisman A., et al. Randomized study of basal-bolus insulin therapy in the inpatient management of patients with type 2 diabetes (RABBIT 2 Trial). Diabetes Care. 2007;30:2181–2186.
14 Van den Berghe G., Wouters P., Weekers F., et al. Intensive insulin therapy in the critically ill patients. N Engl J Med. 2001;345:1359–1367.
15 Wiener R., Wiener D., Larson R. Benefits and risk of tight glucose control in critically ill adults: a meta-analysis. JAMA. 2008;300:933–944.
