[level-membership-for-radiology-category] Can arise from or involve virtually any structure
• Circumscribed cystic mass with variable density







 . The mass is near water density and has small foci of calcification in its septa and peripheral walls
. The mass is near water density and has small foci of calcification in its septa and peripheral walls  . The soft nature of the mass is indicated by the absence of bowel obstruction.
. The soft nature of the mass is indicated by the absence of bowel obstruction.
 , which, like the peripheral walls, are thin.
, which, like the peripheral walls, are thin.
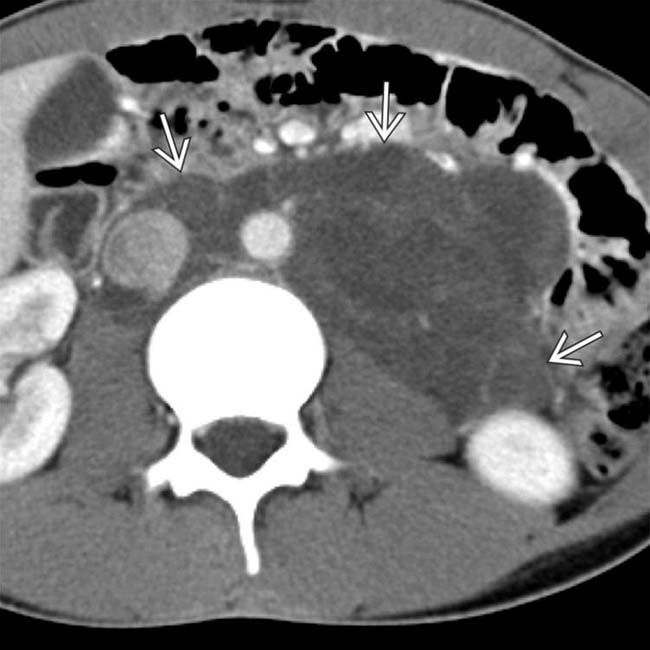
 filling much of the lower abdomen. Note the calcifications
filling much of the lower abdomen. Note the calcifications  in the septa and the peripheral walls.
in the septa and the peripheral walls.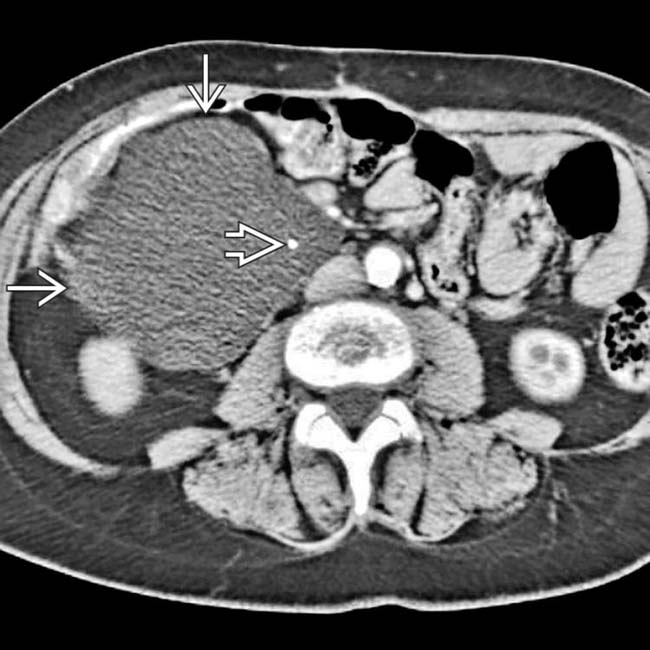
 with subtle septa and a small focus of calcification
with subtle septa and a small focus of calcification  . The mass was resected and found to contain chylous fluid (typical of a lymphangioma) and an epithelial lining, features that help account for the variety of names for this tumor.
. The mass was resected and found to contain chylous fluid (typical of a lymphangioma) and an epithelial lining, features that help account for the variety of names for this tumor.IMAGING
General Features


















 throughout the retroperitoneum. The lesions surround major vasculature without mass effect or narrowing.
throughout the retroperitoneum. The lesions surround major vasculature without mass effect or narrowing.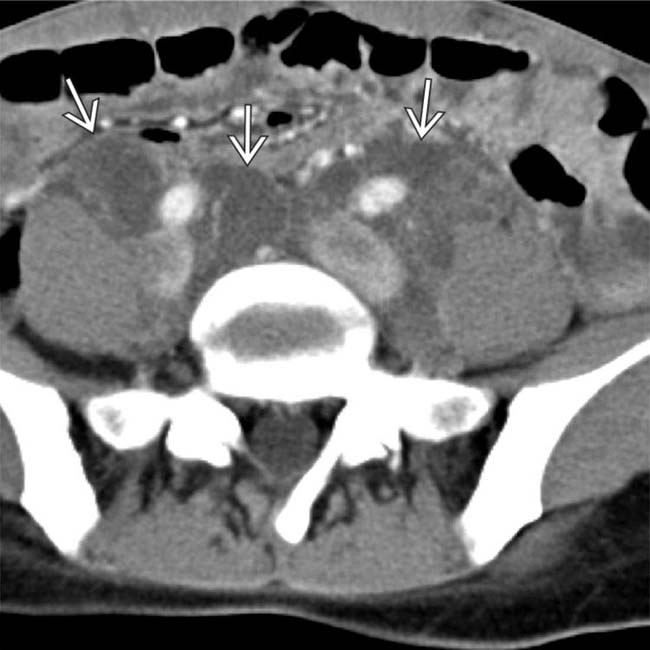
 along the iliac chains in the pelvis. Patients with lymphangiomatosis, as in this case, can have innumerable lymphangiomas anywhere in the body.
along the iliac chains in the pelvis. Patients with lymphangiomatosis, as in this case, can have innumerable lymphangiomas anywhere in the body.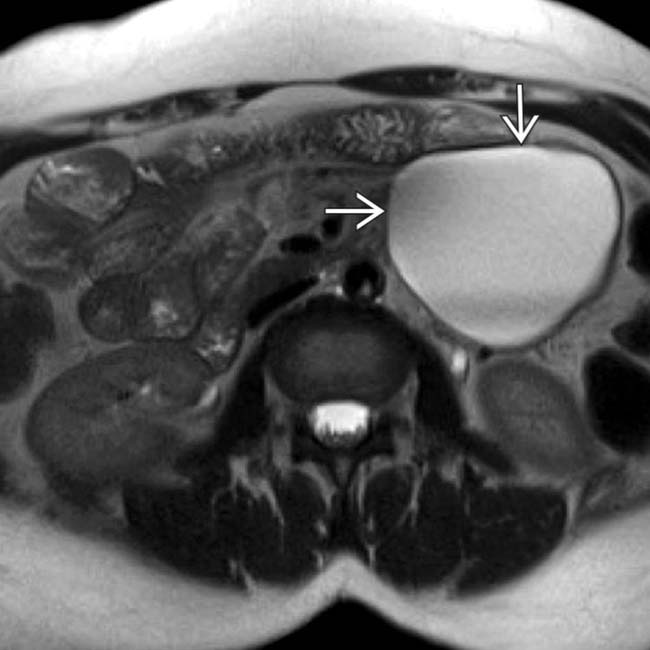
 in the left pelvic retroperitoneum. As in this case, most lymphangiomas are uniformly T2 hyperintense, although intralesional hemorrhage, debris, or fat can result in a more intermediate T2 signal.
in the left pelvic retroperitoneum. As in this case, most lymphangiomas are uniformly T2 hyperintense, although intralesional hemorrhage, debris, or fat can result in a more intermediate T2 signal.
 , features that would cast doubt on the diagnosis of a lymphangioma.
, features that would cast doubt on the diagnosis of a lymphangioma.
 in the retroperitoneum. Notice the lack of any internal enhancing soft tissue or mural nodularity.
in the retroperitoneum. Notice the lack of any internal enhancing soft tissue or mural nodularity.
 envelops vasculature
envelops vasculature  without appreciable mass effect or narrowing (characteristic of lymphangiomas).
without appreciable mass effect or narrowing (characteristic of lymphangiomas).
 in the left retroperitoneum. The lesion abuts the pancreatic tail and left colon without appreciable mass effect.
in the left retroperitoneum. The lesion abuts the pancreatic tail and left colon without appreciable mass effect.
 . This appearance is quite common with lymphangiomas, which frequently appear to have multiple internal discrete components or locules.
. This appearance is quite common with lymphangiomas, which frequently appear to have multiple internal discrete components or locules.
 in the left retroperitoneum. The lesion envelops multiple arteries and veins
in the left retroperitoneum. The lesion envelops multiple arteries and veins  , which do not appear deviated or narrowed.
, which do not appear deviated or narrowed.
 , which has several discrete cystic components and appears multiloculated. These lesions are characteristically soft, and while they abut adjacent structures, there is typically no mass effect.
, which has several discrete cystic components and appears multiloculated. These lesions are characteristically soft, and while they abut adjacent structures, there is typically no mass effect.
 in this patient with cystic lymphangioma.
in this patient with cystic lymphangioma.
 .
.

[/level-membership-for-radiology-category][not-level-membership-for-radiology-category] Can arise from or involve virtually any structure
• Circumscribed cystic mass with variable density
. The mass is near water density and has small foci of calcification in its septa and peripheral walls . The soft nature of the mass is indicated by the absence of bowel obstruction., which, like the peripheral walls, are thin. filling much of the lower abdomen. Note the calcifications in the septa and the peripheral walls. with subtle septa and a small focus of calcification . The mass was resected and found to contain chylous fluid (typical of a lymphangioma) and an epithelial lining, features that help account for the variety of names for this tumor.IMAGING
General Features
CT Findings
• Circumscribed cystic mass with variable density
 Typically water density (near 0 HU) or chylous (< -20 HU), with lesions rarely demonstrating hemorrhagic contents
Typically water density (near 0 HU) or chylous (< -20 HU), with lesions rarely demonstrating hemorrhagic contents
Typically water density (near 0 HU) or chylous (< -20 HU), with lesions rarely demonstrating hemorrhagic contentsBuy Membership for Radiology Category to continue reading. Learn more here
[/not-level-membership-for-radiology-category]
