[level-membership-for-anesthesiology-category]
35 Lumbar Somatic Block
Perspective
Lumbar somatic block is often used to complement multiple intercostal nerve blocks, thus allowing anesthesia for lower abdominal and even upper leg surgery. For example, lumbar somatic block of T12, L1, and L2 will cover most of the requirements for inguinal herniorrhaphy. Likewise, individual blocks of lumbar nerves (including block of T12 off the L1 spine) may allow differentiation of lower abdominal and post-herniorrhaphy pain syndromes. Because this nerve block is carried out in a paravertebral location, it can be considered a form of paravertebral nerve block. The paravertebral block described in Chapter 37, Paravertebral Block, is a large-volume, single-injection method.
Placement
Anatomy
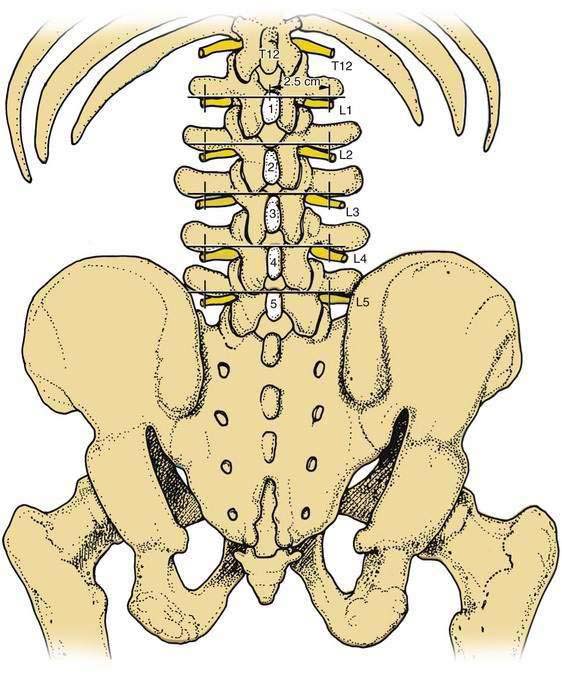
It is useful to conceptualize paravertebral lumbar somatic block as an intercostal block in miniature. Using this concept, the short vertebral transverse process (a “rudimentary rib”) becomes the principal focus and landmark for needle position. Lumbar somatic nerves leave the vertebral foramina slightly caudad and ventral to the transverse process of its respective vertebral level (Fig. 35-1).
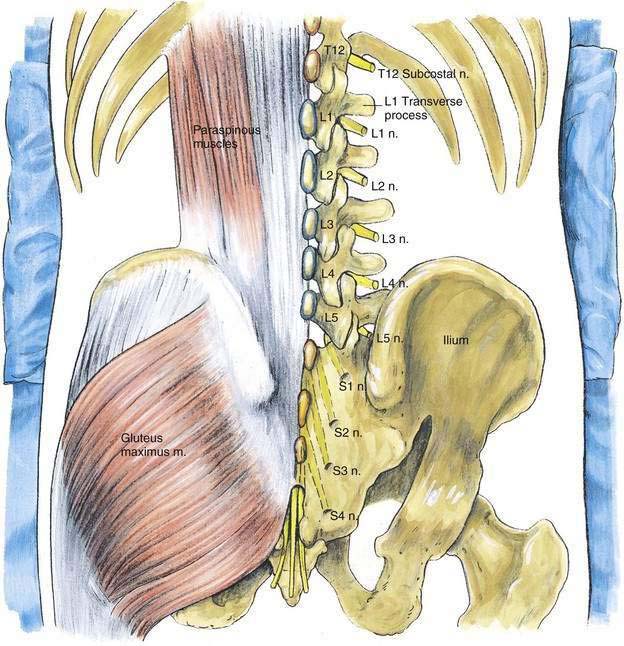
As Figure 35-2 illustrates, from the intervertebral foramina the lumbar somatic nerves angle caudad and anteriorly and hence pass anterior to the lateral extent of the transverse process of the next-lower vertebral body (see Fig. 35-1). For example, as the L1 somatic root leaves its intervertebral foramen, its route places it immediately anterior at the lateral border of the L2 transverse process. Similarly, the T12 somatic root (a subcostal nerve) is found immediately anterior at the lateral extent of the L1 transverse process.
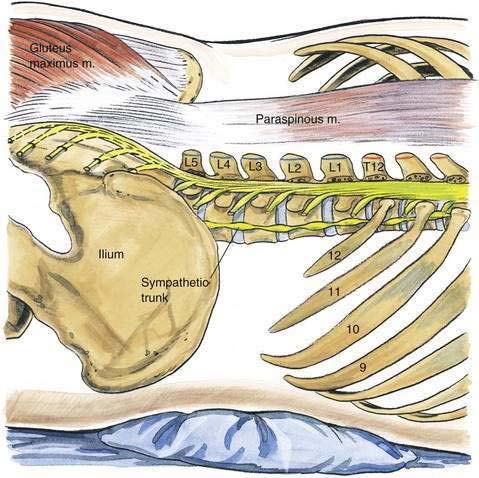
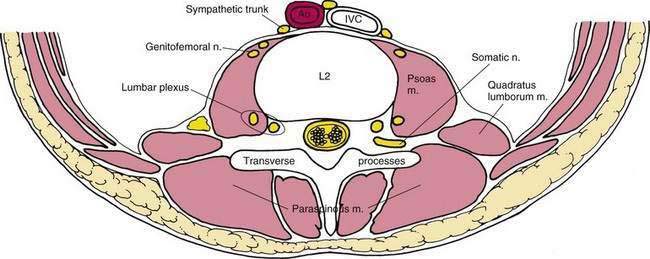
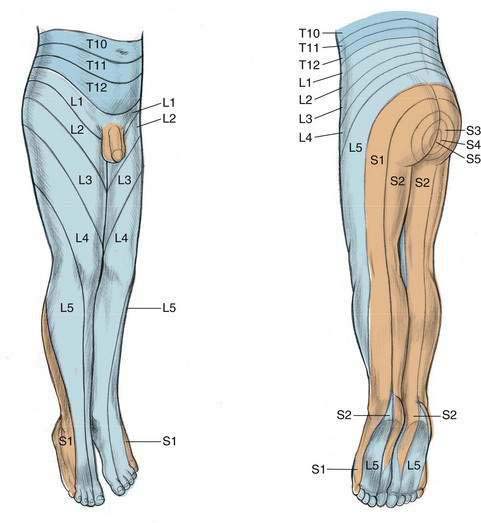
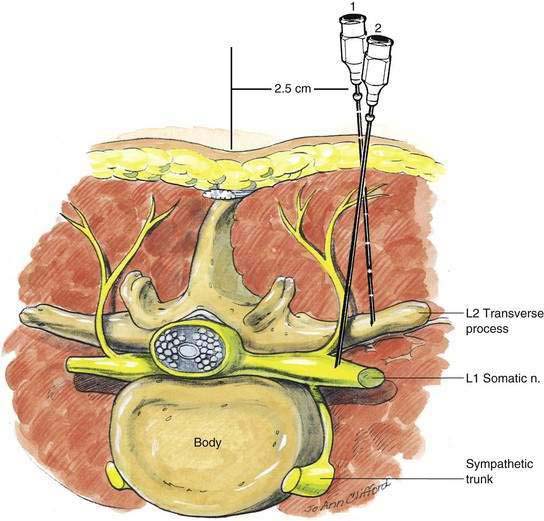
Returning to the intercostal nerve analogy, each lumbar nerve gives off an immediate posterior branch to the paravertebral muscles and skin of the back. Again, as with intercostal nerve anatomy, the lumbar somatic nerve also receives white rami communicantes from the upper two or three lumbar nerves and gives rise to gray rami communicantes to all lumbar somatic nerves. After these connections to the sympathetic nervous system, the main somatic nerve passes directly into the psoas major muscle or comes to lie in a plane between the psoas and the quadratus lumborum muscles. Here the nerves intertwine to form the lumbar plexus. Figure 35-3 highlights this cross-sectional anatomy. Figure 35-4 illustrates the cutaneous distribution of the lumbar somatic nerves.
Position
The conceptual similarity of this block to an intercostal nerve block carries through to the actual performance of the technique. The most advantageous position is to have the patient prone with a pillow under the lower abdomen to reduce lumbar lordosis. Skin markings are made as illustrated in Figure 35-5 (i.e., the lumbar spinous process of each vertebra corresponding to the roots to be blocked is identified and marked). Then, from the cephalad edge of each of these lumbar posterior spines, lines are drawn horizontally, and marks are placed on the lines 2.5 to 3 cm from the midline (paravertebral in location). The anatomic rationale behind these markings is that the cephalad edge of each lumbar posterior spine is approximately on the same horizontal plane as its own vertebral transverse process. Skin wheals are made at the site 2.5 to 3 cm from the midline on the lines overlying the lower edge of the transverse process. Through the skin wheals an 8-cm, 22-gauge needle is inserted in a vertical plane without a syringe attached (Fig. 35-6). As the needle is advanced, it will contact the transverse process at a depth of 3 to 5 cm in the average adult (needle position 1). Failure to contact the transverse process at that depth implies that the needle has passed between the two transverse processes.
[/level-membership-for-anesthesiology-category][not-level-membership-for-anesthesiology-category]
35 Lumbar Somatic Block
Perspective
Lumbar somatic block is often used to complement multiple intercostal nerve blocks, thus allowing anesthesia for lower abdominal and even upper leg surgery. For example, lumbar somatic block of T12, L1, and L2 will cover most of the requirements for inguinal herniorrhaphy. Likewise, individual blocks of lumbar nerves (including block of T12 off the L1 spine) may allow differentiation of lower abdominal and post-herniorrhaphy pain syndromes. Because this nerve block is carried out in a paravertebral location, it can be considered a form of paravertebral nerve block. The paravertebral block described in Chapter 37, Paravertebral Block, is a large-volume, single-injection method.
Placement
Anatomy
It is useful to conceptualize paravertebral lumbar somatic block as an intercostal block in miniature. Using this concept, the short vertebral transverse process (a “rudimentary rib”) becomes the principal focus and landmark for needle position. Lumbar somatic nerves leave the vertebral foramina slightly caudad and ventral to the transverse process of its respective vertebral level (Fig. 35-1).
As Figure 35-2 illustrates, from the intervertebral foramina the lumbar somatic nerves angle caudad and anteriorly and hence pass anterior to the lateral extent of the transverse process of the next-lower vertebral body (see Fig. 35-1
[/not-level-membership-for-anesthesiology-category]
