[level-membership-for-orthopaedics-category]CHAPTER 12
LOWER LEG, ANKLE, AND FOOT
SELECTED MOVEMENTS

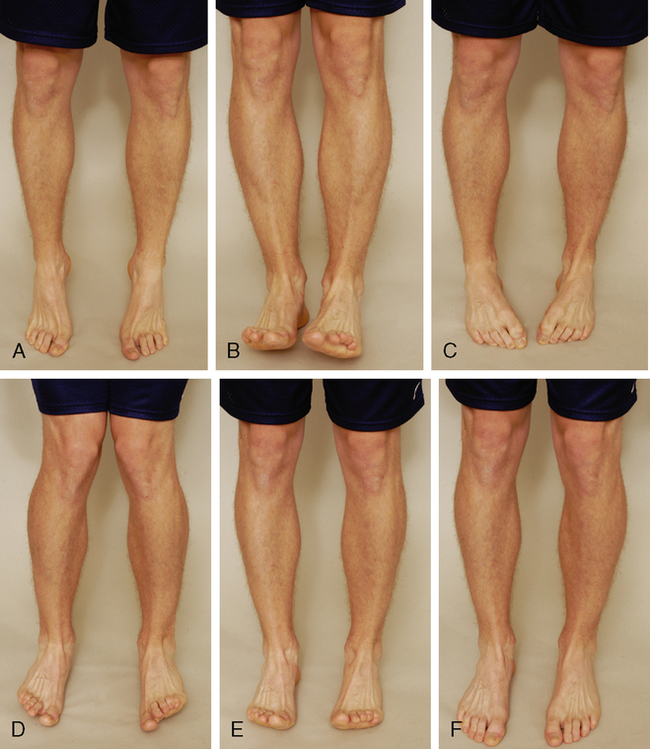
Active movements of the lower leg, ankle, and foot should be done in both weight-bearing and non-weight-bearing positions (long leg sitting or supine lying), and the examiner should note any differences, because foot deformities and deviations, in addition to decreased range of motion (ROM), can lead to injury in other parts of the lower kinetic chain and spine.1

INDICATIONS OF A POSITIVE TEST
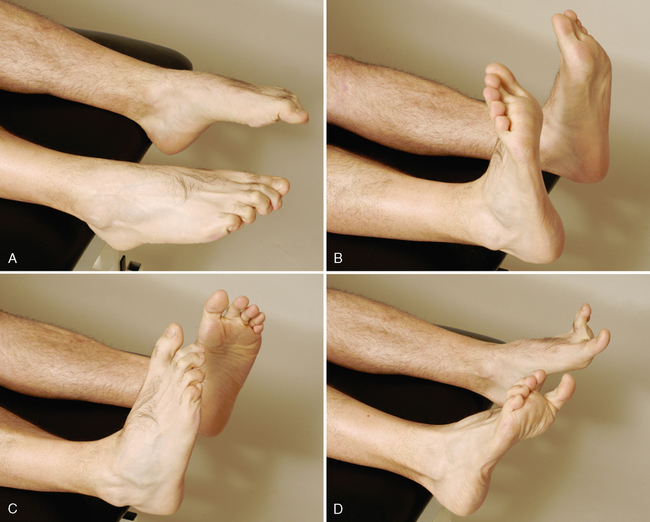
Plantar flexion of the ankle is approximately 50°. If the ROM is less than this or is less than for the unaffected leg, the movement is restricted for some reason. The patient’s heel normally inverts when the movement is performed in weight bearing. If heel inversion does not occur, the foot is unstable, or tibialis posterior weakness or tightness is present.2–4 The tibialis posterior muscle and tendon balance the pull of the peroneal muscles, protect the spring ligament, and invert and stabilize the hindfoot during toe-off.5
SPECIAL TESTS FOR NEUTRAL POSITION OF THE TALUS
Relevant Special Tests
Suspected Injury
• Talar position tests are not designed to identify specifically any particular pathological condition; rather, they identify anatomical and biomechanical abnormalities that contribute to a pathological condition. That pathology may occur locally at the foot and ankle or remotely at areas such as the back, knee, or hip.
Epidemiology and Demographics
The overall prevalence of malalignment reported in the literature ranges from 10% in the Cheshire Foot Pain and Disability Survey in the United Kingdom to 28% in the Framingham Foot Study in the United States. Clinically, it has been hypothesized that abnormal talar alignment and mechanics can result in pathological conditions of the foot. Regardless of the prevalence of foot pain, the cause-and-effect relationship between talar position and pathological conditions has yet to be definitively determined.6–10
Mechanism of Injury
RELIABILITY/SPECIFICITY/SENSITIVITY COMPARISON11–16
| Validity | Interrater Reliability | Intrarater Reliability | |
| Neutral position of the talus (weight-bearing position) | Unknown | 0.15-0.79 | 0.14-0.85 |
| Neutral position of the talus (supine) | Unknown | Unknown | Unknown |
| Neutral position of the talus (prone) | Unknown | 0.25 | 0.06-0.77 |

NEUTRAL POSITION OF THE TALUS (PRONE)11–13,17–20 


NEUTRAL POSITION OF THE TALUS (WEIGHT-BEARING POSITION)11,13,16,18,21,22 

• Mueller et al.13 described a progression of neutral talus positions in standing (i.e., the navicular drop test) to quantify midfoot mobility and its effect on other parts of the kinetic chain. With a small, rigid ruler, the examiner first measures the height of the navicular from the floor in the neutral talus position, using the most prominent part of the navicular tuberosity; the height of the navicular in normal relaxed standing then is measured. The difference, called the navicular drop, indicates the amount of foot pronation or flattening of the medial longitudinal arch during standing. Any measurement greater than 10 mm is considered abnormal.
SPECIAL TESTS FOR ALIGNMENT
Relevant Special Tests
Epidemiology and Demographics
Few population-based studies have examined the prevalence of foot pain in the general population. Causal relationships between specific malalignments and injuries have been difficult to verify. In a random sampling of people in Australia, foot pain affected nearly 1 in 5 individuals. The pain was associated with increased age, female gender, obesity, and pain in other body regions, and it had a significant detrimental impact on health-related quality of life. The overall prevalence reported in this study was higher than that reported in the Cheshire Foot Pain and Disability Survey in the United Kingdom (10%). However, it was lower than the prevalence rates reported in two studies in the United States: the National Health Interview Survey in the United States (24%) and the Framingham Foot Study (28%).6–10
Mechanism of Injury
RELIABILITY/SPECIFICITY/SENSITIVITY COMPARISON23,24
| Leg-Rearfoot (Heel) Alignment | Forefoot-Rearfoot (Heel)Alignment | |
| Validity | Unknown | Unknown |
| Interrater reliability | Unknown | 0.86 |
| Intrarater reliability | 0.86 | 0.88 |
| Specificity | Unknown | Unknown |
| Sensitivity | Unknown | Unknown |




SPECIAL TEST FOR TIBIAL TORSION
Relevant Special Test
Epidemiology and Demographics
Tibial torsion usually is first noticed in children as they approach 2 years of age. Some tibial medial rotation is normal in newborns. This medial rotation usually straightens during the first year of life. In the case of excessive tibial torsion, the tibial rotation fails to straighten or the amount of rotation is too great to correct totally. It becomes more apparent as the child begins to walk, although it usually is present before then. No gender preference is apparent; males and females are equally affected. It is more common for patients to be affected bilaterally. Two-thirds of patients with tibial torsion are affected in both tibias.25–27
Relevant Signs and Symptoms
Tibial torsions usually are painless. Functionally, severe in-toeing or out-toeing may result in abnormal gait mechanics. Patients may appear “knock-kneed,” “pigeon-toed,” or “bow-legged.” Over time, the abnormal mechanics alter the forces placed on associated joints and structures, resulting in a pathological condition. At this point, the patient’s signs and symptoms reflect the resultant condition.28,29
Mechanism of Injury

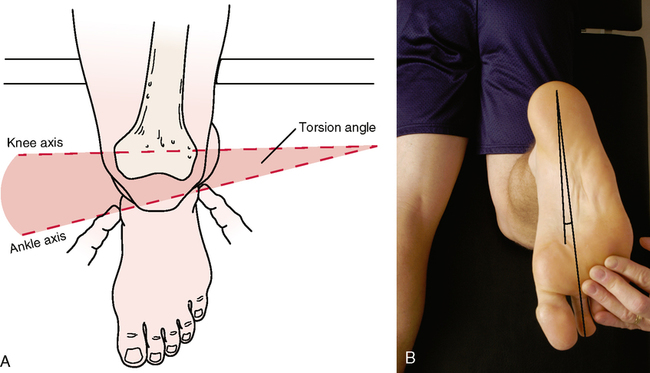
• Tibial torsion may also be tested with the patient in the prone position. The patient lies prone with the knee flexed to 90°. The examiner views from above the angle formed by the foot and thigh after the subtalar joint has been placed in the neutral position, noting the angle the foot makes with the tibia. This method most often is used in children, because it is easier to observe the feet from above.
• The examiner must remember the midline of the foot is considered, by convention, to go through the second toe.
SPECIAL TESTS FOR LIGAMENTOUS INSTABILITY
Relevant Special Tests
Definition
Ankle sprains are classified into three categories:32–35
• Lateral (low ankle) sprains occur when the ligaments on the lateral portion of the ankle are injured. The most common ligaments injured are the anterior talofibular ligament and the calcaneofibular ligament.
• Syndesmotic (high ankle) sprains are synonymous with anterior tibiofibular ligaments sprains. These sprains occur when the ligaments between the two major bones of the lower leg (the tibia and the fibula) are injured at the level of the ankle.
• Medial ankle sprains are the rarest and occur when the deltoid ligament is injured.
Mechanism of Injury
Lateral (low ankle) sprain: Lateral ankle ligament injuries usually are the result of a rapid inversion movement at the ankle. The patient commonly reports that the ankle “rolled,” or the person states that a pop was heard during activities such as planting the foot when running, stepping up or down, or stepping or landing on an uneven surface.
Syndesmosis (high ankle) sprain: Syndesmotic sprains are believed to occur when the ankle is planted in dorsiflexion with lateral rotation of the lower leg. Most syndesmotic ankle sprains are believed to be the result of direct contact between individuals.
Medial ankle sprain: Medial ankle sprains occur with plantar flexion with eversion.

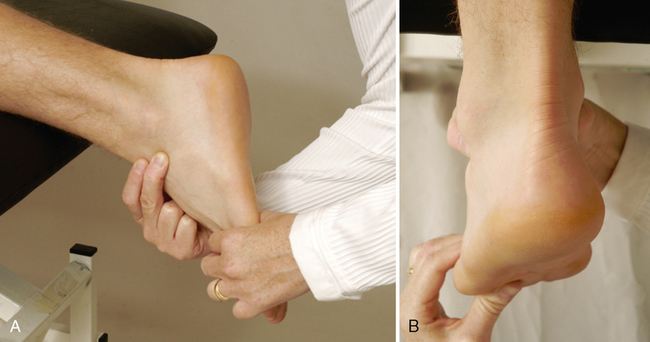
• In the plantar flexed position, the anterior talofibular ligament is perpendicular to the long axis of the tibia. By adding inversion, which gives an anterolateral stress, the examiner can increase the stress on the anterior talofibular ligament and the calcaneofibular ligament.
• Ideally, the knee should be placed in 90° of flexion to alleviate tension on the Achilles tendon. The test should be performed in plantar flexion and in dorsiflexion to test for straight and rotational instabilities.
• The test also may be performed by stabilizing the foot and talus and pushing the tibia and fibula posteriorly on the talus (method 2). In this case, excessive posterior movement of the tibia and fibula on the talus indicates a positive test result.


TALAR TILT TEST37,44,45,47,50,51 

INDICATIONS OF A POSITIVE TEST
Excessive motion or pain (or both) compared to the unaffected side indicates a positive test result.
• The patient’s gastrocnemius muscle may be relaxed by flexion of the knee.
• If the foot is plantar flexed, the anterior talofibular ligament is more likely to be tested (inversion stress test).
• On a radiograph, the talar tilt may be measured by obtaining the angle between the distal aspect of the tibia and the proximal surface of the talus.
EXTERNAL ROTATION STRESS TEST (KLEIGER TEST)38,44,52–58 

• On a stress radiograph, if the lateral malleolus is intact, an increase in the medial clear space suggests rupture of the ligament.
• The test also may be performed with the patient lying prone and the knee flexed to 90°. The examiner holds the foot in plantigrade and applies a passive lateral rotation stress to the foot and ankle.
OTHER SPECIAL TESTS


INDICATIONS OF A POSITIVE TEST
If the asymmetry is corrected by “correcting” the position of the limb, the leg is structurally normal (the bones have the proper length), but abnormal joint mechanics (a functional deficit) are producing a functional leg length difference (see Table 9-1). Therefore, if the asymmetry is corrected by proper positioning, the test result is positive for a functional leg length difference.
THOMPSON’S (SIMMONDS’) TEST (SIGN FOR ACHILLES TENDON RUPTURE)60–63 
JOINT PLAY MOVEMENTS


LONG AXIS EXTENSION AT THE METATARSOPHALANGEAL AND INTERPHALANGEAL JOINTS 

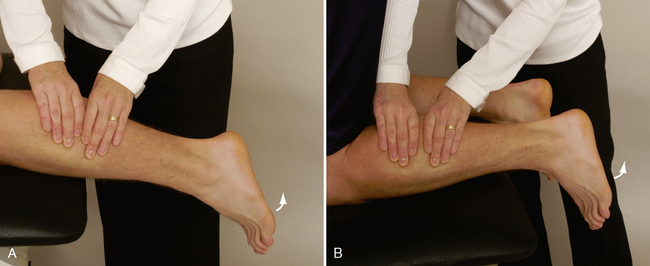
ANTERIOR-POSTERIOR GLIDE AT THE ANKLE JOINT 

• During the anterior movement, the foot should move in an arc into plantar flexion.
• During the posterior movement, the foot should move in an arc into dorsiflexion.
• Although this test is similar to the anterior drawer test, the movements are not the same, because the joint play involves an arc of movement.
• The ankle should be placed in slight plantar flexion for testing. If the ankle is dorsiflexed, which locks the talocrural joint, or if tension is placed upon the Achilles tendon, joint play will be restricted.
ANTERIOR-POSTERIOR GLIDE AT THE MIDTARSAL AND TARSOMETATARSAL JOINTS 

• Step 1: The examiner stabilizes the navicular, talus, and calcaneus with one hand by grasping the bones in the web space, thumb, and fingers of the examiner’s hand. The examiner’s other hand is placed around the distal row of tarsal bones (cuneiforms and cuboid). If the hands are positioned properly, they should touch. An anteroposterior gliding movement of the distal row of tarsal bones is applied while the proximal row of tarsal bones is stabilized. The two feet are compared.
• Step 2: The examiner’s hands then are moved distally so that the stabilizing hand rests over the distal row of tarsal bones and the mobilizing hand rests over the proximal aspect of the metatarsal bones. Again, the hands should be positioned so that they touch. An anteroposterior gliding movement of the metatarsal bones is applied while the distal row of tarsal bones is stabilized. The two feet are compared.
ANTERIOR-POSTERIOR GLIDE AT THE METATARSOPHALANGEAL AND INTERPHALANGEAL JOINTS 





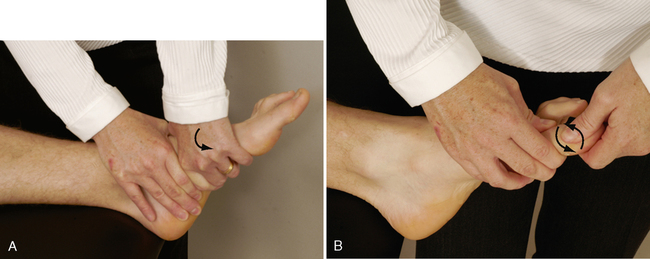
ROTATION AT THE MIDTARSAL, TARSOMETATARSAL, METATARSOPHALANGEAL AND PHALANGEAL JOINTS 


[/level-membership-for-orthopaedics-category][not-level-membership-for-orthopaedics-category]CHAPTER 12
LOWER LEG, ANKLE, AND FOOT
SELECTED MOVEMENTS
Active movements of the lower leg, ankle, and foot should be done in both weight-bearing and non-weight-bearing positions (long leg sitting or supine lying), and the examiner should note any differences, because foot deformities and deviations, in addition to decreased range of motion (ROM), can lead to injury in other parts of the lower kinetic chain and spine.1
INDICATIONS OF A POSITIVE TEST
Plantar flexion of the ankle is approximately 50°. If the ROM is less than this or is less than for the unaffected leg, the movement is restricted for some reason. The patient’s heel normally inverts when the movement is performed in weight bearing. If heel inversion does not occur, the foot is unstable, or tibialis posterior weakness or tightness is present.2–4 The tibialis posterior muscle and tendon balance the pull of the peroneal muscles, protect the spring ligament, and invert and stabilize the hindfoot during toe-off.5
SPECIAL TESTS FOR NEUTRAL POSITION OF THE TALUS
Relevant Special Tests
Suspected Injury
• Talar position tests are not designed to identify specifically any particular pathological condition; rather, they identify anatomical and biomechanical abnormalities that contribute to a pathological condition. That pathology may occur locally at the foot and ankle or remotely at areas such as the back, knee, or hip.
Epidemiology and Demographics
The overall prevalence of malalignment reported in the literature ranges from 10% in the Cheshire Foot Pain and Disability Survey in the United Kingdom to 28% in the Framingham Foot Study in the United States. Clinically, it has been hypothesized that abnormal talar alignment and mechanics can result in pathological conditions of the foot. Regardless of the prevalence of foot pain, the cause-and-effect relationship between talar position and pathological conditions has yet to be definitively determined.6–10
Mechanism of Injury
RELIABILITY/SPECIFICITY/SENSITIVITY COMPARISON11–16
| Validity | Interrater Reliability | Intrarater Reliability | |
| Neutral position of the talus (weight-bearing position) | Unknown | 0.15-0.79 | 0.14-0.85 |
| Neutral position of the talus (supine) | Unknown | Unknown | Unknown |
| Neutral position of the talus (prone) | Unknown | 0.25 | 0.06-0.77 |
NEUTRAL POSITION OF THE TALUS (PRONE)11–13,17–20
NEUTRAL POSITION OF THE TALUS (WEIGHT-BEARING POSITION)11,13,16,18,21,22
• Mueller et al.13 described a progression of neutral talus positions in standing (i.e., the navicular drop test) to quantify midfoot mobility and its effect on other parts of the kinetic chain. With a small, rigid ruler, the examiner first measures the height of the navicular from the floor in the neutral talus position, using the most prominent part of the navicular tuberosity; the height of the navicular in normal relaxed standing then is measured. The difference, called the navicular drop, indicates the amount of foot pronation or flattening of the medial longitudinal arch during standing. Any measurement greater than 10 mm is considered abnormal.
SPECIAL TESTS FOR ALIGNMENT
Relevant Special Tests
Epidemiology and Demographics
Few population-based studies have examined the prevalence of foot pain in the general population. Causal relationships between specific malalignments and injuries have been difficult to verify. In a random sampling of people in Australia, foot pain affected nearly 1 in 5 individuals. The pain was associated with increased age, female gender, obesity, and pain in other body regions, and it had a significant detrimental impact on health-related quality of life. The overall prevalence reported in this study was higher than that reported in the Cheshire Foot Pain and Disability Survey in the United Kingdom (10%). However, it was lower than the prevalence rates reported in two studies in the United States: the National Health Interview Survey in the United States (24%) and the Framingham Foot Study (28%).6–10
