CHAPTER 12 Learning Disabilities
Students with learning disabilities constitute the majority of school-age individuals with disabilities; the number of students with learning disabilities increased from 1.2 million in 1979 to 1980 to 2.9 million in 2003 to 2004.1 Learning disabilities are the most common childhood disabilities and often have lifelong consequences for health and occupational success.2 The prevalence of learning disabilities varies, depending on how learning disabilities are defined and, in the United States, may range from about 4% to 20%.3 In the past, much of the emphasis in medical and psychological pediatric practice has been placed on diagnosis and assessment; indeed, the most controversial issue in the field of learning disabilities currently concerns diagnostic and definitional issues, even though prevention and intervention are equally if not more important clinical issues.
This chapter begins with a brief historical overview of learning disabilities, followed by a discussion of current issues in the definitions and diagnosis of learning disability. What is known about the cognitive correlates of the two most common learning disabilities, reading disability and math disability, is presented, along with a selected review of research on the neurobiology of learning disabilities. The next section is devoted to research on prevention and evidence-based intervention/treatment programs for reading disability and math disability. A brief review of long-term outcomes follows. The chapter closes with a discussion of clinical management of learning disabilities with reference to diagnosis and assessment, comorbid conditions, and prevention and interventions. For further reading on these topics, we suggest peer-reviewed papers and chapters on assessment and identification,4 prevention and intervention,5 the genetics of learning disabilities,6 and comorbid conditions associated with learning disabilities.7–9
HISTORICAL OVERVIEW
Learning disabilities were defined in U.S. federal law with the Learning Disabilities Act in 1969 to address the needs of these children who were not previously well served by the education system.10 The Association for Children with Learning Disabilities, formed by parents and educators and led by the psychologist Samuel Kirk, advocated for recognition of learning disabilities and access to special education services. Lyon and associates5 proposed that, as with many other advancements in fields of medicine, psychology, education, and public policy, systematic scientific inquiry into learning disabilities followed from the identification of real-world problems experienced by children and from public advocacy on their behalf.
Despite the mobilizing influence on research of the recognition of learning disabilities, the scientific basis of learning disabilities has historical roots in the neurology of acquired language disorders studied in the 1800s. In these studies of aphasia, specific deficits in the comprehension and production of language in the context of otherwise spared cognitive function were noted in adults with acquired brain lesions. These observations proved important with regard to one of the central features of learning disabilities: namely, that learning difficulties could result in selective rather than general cognitive deficits.11
In the late 1800s and early 1900s, cases of what today would be called reading disabilities were reported by neurologists who observed children and adults with no known brain injuries who could not read despite seemingly intact general cognitive abilities.12 In the 1920s, Samuel Orton, a neurologist, proposed that in children who could not read, development of left hemisphere dominance for language functions was delayed or had failed. He was the first to address the heterogeneity of learning disabilities as disorders that could specifically affect reading, writing, speech, comprehension, or motor skills.11 In collaboration with the linguist, Anne Gillingham, he devised intervention programs for children with reading difficulties, variants of which are still in use13 and undergoing evaluation as to their efficacy.5 Another important influence in the field of learning disabilities arose from studies in which investigators attempted to understand similarities in behavioral disorders such as hyperactivity in children with brain injuries and in children with no brain injury who had learning difficulties and normal intelligence. It was inferred that this latter group had minimal brain dysfunction.11
DIAGNOSTIC AND DEFINITIONAL ISSUES
Many policymakers and school administrators are concerned about the increasing prevalence of learning disabilities, at least in part because special education is much more costly than general education: $12,000 versus $6500 per student.14 This is at least one reason why establishing acceptable criteria for learning disability identification has been the most controversial issue in the field of learning disability. At the heart of this controversy is the IQ-achievement discrepancy. Although not required by law, a severe discrepancy between achievement and intellectual ability is most frequently used for identification. It is easy to see how the IQ-achievement discrepancy grew out of the early observations that learning disabilities were deficits in specific skills in an otherwise cognitively intact individual. However, the IQ-achievement discrepancy is fraught with measurement and conceptual problems. After a review of current diagnostic guidelines, we describe these technical difficulties.
U.S. federal regulations governing special education refer to learning disabilities as disorders that can occur in one or more of the following: oral expression, listening comprehension, written expression, basic reading skill, reading comprehension, mathematics calculation, and mathematics reasoning. The federal definition of learning disabilities is notable for its emphasis on exclusionary factors in identification, including the idea of a discrepancy between IQ and achievement that is not caused by a sensory or motor handicap; by mental retardation; by emotional disturbance; or by social, cultural, and economic factors.15,16 In Canada, education is under provincial, not federal, jurisdiction. However, provincial regulations governing special education are very similar to those in the United States. For example, the Ontario Ministry of Education defines learning disabilities with discrepancy and exclusionary criteria similar to those in the U.S. federal definition.17
The Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (DSM-IV),18 and the International Classification of Diseases, 10th edition,19 provide criteria for diagnosing specific and general learning disabilities. For example, in the DSM-IV, learning disorders are classified into four categories: Reading Disorder, Mathematics Disorder, Disorder of Written Expression, and Learning Disorder Not Otherwise Specified. In the DSM-IV, Learning Disorders are also defined in an exclusionary manner. For example, a reading disorder refers to a failure to achieve at expected levels for reading accuracy or reading comprehension and would be diagnosed (1) when reading achievement, measured by standardized tests of reading accuracy and/or comprehension, is substantially below what is expected on the basis of the individual’s age, intelligence, and appropriate educational experiences; (2) when this failure interferes with academic achievement or activities of daily living that require reading; or, (3) if a sensory impairment is present, the reading deficit is in excess of what is typically expected for that impairment.20
Classification systems are fundamental in many areas of science and practice, and as such, scientific evaluation of their validity, reliability, and coverage is required in order for them to be useful.21 Such scientific evidence was unavailable at the time learning disabilities were categorized, and despite substantial subsequent research on the validity and reliability of learning disability classification, the definition of learning disabilities and their categorization have not changed much in practice. We discuss evidence pertaining to validity and reliability in learning disability classification with regard to (1) the use of the IQ-achievement discrepancy, (2) the heterogeneity of learning disabilities, and (3) exclusionary factors. Comprehensive reviews of this literature were provided by Lyon and associates11 and by Fletcher and colleagues.21
IQ-Achievement Discrepancy
The traditional learning disability diagnosis—low achievement in one or more of the learning disability domains that is significantly discrepant from intelligence—is a classification hypothesis that requires validation. Validation studies, in which groups defined by the discrepancy formula are compared with groups defined according to poor academic achievement without reference to IQ, reveal the following: First, few cognitive or affective characteristics such as memory and phonological awareness differentiate poor readers with discrepancies from those without discrepancies.22 Second, the degree of discrepancy from IQ is not meaningfully related to the severity of the learning disability.23 Third, the degree of discrepancy is predictive neither of rate of growth in reading over time nor the reading levels of children with or without IQ-achievement discrepancy over time.24 Fourth, the degree of discrepancy is not predictive of whether or how well a child will respond to intervention,25 nor does it inform instruction in important ways.26 Fifth, differences in heritability estimates for children with and without the discrepancy, although significant, are typically small even in large samples.27
In addition to problems with validity, other difficulties in the reliability of the discrepancy hypothesis concern measurement error of the intelligence and achievement tests, unreliability of difference or discrepancy scores, and use of arbitrary cutoff points to partition what is a normal distribution of skills, particularly in the absence of validation studies indicating what those clinical cutoff points should be.11 If categorization based on IQ-achievement discrepancy is reliable, then the classification of children as having a learning disability by an IQ-achievement discrepancy should be stable over time. However, there is considerable instability in classification with actual or simulated data.28,29 In sum, evidence for the validity of the discrepancy hypothesis is weak, which raises questions about its use in assessment and identification of learning disabilities and in decision making with regard to special education services. Despite technical difficulties in traditional methods for learning disability identification, few experts disagree that the construct of learning disability is a legitimate one or that learning disabilities can have heterogeneous forms.
Heterogeneity of Learning Disabilities
Several types of learning disabilities are identified in classification systems, these types of learning disabilities frequently co-occur, and learning disabilities are often accompanied by other childhood disorders such as attention disorders and problems in social and emotional domains.8,30
How well do the classifications in federal law and the DSM-IV capture what is known about heterogeneity of learning disabilities? There is strong evidence for the existence of at least two types of reading disability—one in word reading and one in reading comprehension—and perhaps a third in reading fluency.21 When reading decoding accuracy and fluency are intact, the deficit in reading comprehension parallels that observed in listening comprehension,31 which suggests that disabilities in reading comprehension and listening comprehension may be indistinguishable. In a similar way, some evidence substantiates at least two forms of math disability, one in arithmetic calculations and another in word problems,32 but there is little evidence, at present, of a disability in math reasoning.11 Evidence of a specific learning disability in written expression in the absence of other learning disabilities is also weak.21 In most cases, comorbidity (e.g., reading disability with math disability or reading disability with attention-deficit/hyperactivity disorder [ADHD]) is associated with greater impairment in academic domains than when disorders occur independently.21 In addition, there is some evidence that the nature of math disabilities and their cognitive characteristics differ in some ways, depending on whether there is a comorbid reading disability.33
Exclusionary Criteria
The hypothesis that learning disability reflects “unexpected” low achievement—as opposed to low achievement as a result of emotional disturbance, social or economic disadvantage, cultural factors, or inadequate instruction—was not based on empirical validation of these factors. There is currently no evidence that children who suffer from emotional disorders such as depression or anxiety differ in any important way from children with learning disability without emotional disorders in terms of the causes of the learning disorder or their response to intervention.21
Environmental factors influence the developmental precursors important for learning how to read and perform math. Particularly striking are studies showing that children who are socially and economically disadvantaged have vocabularies half the size of those of nondisadvantaged children at school entry34; enter kindergarten knowing only one letter of the alphabet35; and begin school with less informal number and quantitative knowledge than do their middle-income peers.36 However, provision of high-quality language and literacy instruction improves academic preparedness in children graduating from Head Start,37 as do mathematical interventions with disadvantaged preschool-aged children.38 Interventions based on phonological and alphabetical instruction also yield positive effects for older disadvantaged children.39 In sum, socially and economically disadvantaged children develop in environments that may provide less than optimal support for the growth of cognitive skills that are important precursors for later academic skill learning, but they respond to high-quality interventions in similar ways as do their nondisadvantaged peers with learning disabilities. In view of these observations, the validity of exclusion on social and economic bases seems unwarranted.
At the time learning disabilities were defined, there was little consensus about what constituted adequate instruction. This knowledge base, at least for reading, is now substantive.39,40 The definition implies that the child’s response to adequate instruction should be assessed before the learning disability label is applied,21 and yet the adequacy of instruction is often assumed rather than measured.
One promising model for reconceptualizing learning disability is in terms of a failure to respond to validated intervention.41–43 Responsiveness to intervention (RTI) as an approach to identifying learning disability was first proposed in a 1982 National Research Council report.44 Three criteria were suggested for judging the validity of a special education classification: (1) whether the quality of the general education program is such that adequate learning might be expected; (2) whether the special education is of sufficient value to improve student outcomes and thereby justify the classification; and (3) whether the assessment process used for identification is accurate and meaningful. When all three criteria are met, a special education classification is deemed valid. RTI links multiple short assessments over time to intervention and has been shown to have stronger validity and reliability than other identification models. Because identification of a learning disability under RTI is based on lack of response to high-quality instruction, intervention is attempted before the learning disability label is applied. This approach is quite different from all other models, in which diagnosis is applied before intervention.45 However, for classification, there is still a need to be able to identify a child according to some criterion score, and this criterion score needs to be linked directly to functional outcome.45
How Should Learning Disabilities Be Identified?
To summarize, several of the original criteria for identification of a learning disability and classification of learning disabilities have proved to be invalid or unreliable, although these research findings are only just beginning to have an influence on assessment and diagnosis. Furthermore, none of the current classification systems takes relations between learning disabilities or between learning disabilities and other developmental disorders into account. Despite the problems with current diagnostic and classification criteria, the reality is that many jurisdictions use discrepancy formulas and exclusionary criteria to determine who has a learning disability, and this has consequences for who receives special education services. Hybrid models that take into account both low achievement and response to instruction may better identify children who truly have “unexpected” low achievement despite exposure to high-quality instruction.28 As an example, the current means of diagnosing a learning disability is typically based on a single formal assessment point, followed by treatment (the test-and-treat model), whereas the review just presented suggests that a better model would involve the use of high-quality intervention for low academic achievement (identified by teachers and/or parents and assessed by valid and reliable achievement tests), followed by assessment of response to intervention (the treat-and-test model4). It is important to note that the 2004 reauthorization of the Individuals with Disabilities Education Act provides the field of learning disabilities with RTI as an option to the IQ-achievement discrepancy for identifying learning disability. The implications of the critique of current assessment and identification systems and of changes to the Individuals with Disabilities Education Act for the practice of the developmental-behavioral pediatrician are addressed in the final section of this chapter.
CORE COGNITIVE CORRELATES AND NEUROBIOLOGICAL FACTORS
Reading Disability
WORD READING: ACCURACY AND FLUENCY
Core Cognitive Characteristics
Most children who receive special education services in the learning disability category are children with reading disabilities, and these disabilities have also received the most research attention in terms of developmental, cognitive, and neurobiological studies and interventions. Two core cognitive skills have been identified as being causally connected both to the ability to acquire word reading skills and to difficulties in learning how to read: phonological awareness and rapid retrieval of names for visual symbols, or rapid naming.
Although reading requires the decoding of print, it is actually the ability to gain awareness of the sound structure of language at the level of the phoneme, which is essential for learning how to read.46 Unlike letters, which are discrete visual symbols, phonemes in syllables and words sound undifferentiated in normally paced speech. Phonological awareness is measured by tasks that tap the ability of the child to distinguish and manipulate language at the level of the phoneme, such as the abilities to listen to a word and to match sounds in words on the basis of phonemes, to segment words on the basis of phonemes, to blend sounds to form words, and to isolate phonemes in spoken words.47 Longitudinal studies of the reading acquisition process show that phonological awareness at school entry is a potent and unique predictor of word reading ability well into the middle elementary grades.48,49
Phonological measures are also quite accurate for predicting which young children are at risk for reading failure,50 and there is a wealth of research supporting the idea that deficits in phonological processing are at the core of word reading disabilities.51 Researchers who have attempted to identify reading disability subtypes have shown that almost all subtypes identified are characterized by deficits in phonological awareness.52 The use of interventions that address phonological awareness and word recognition are most effective for beginning readers considered to be at high risk for reading failure, and the severity of the deficit in phonological awareness is an important predictor of how easy or difficult it is to remediate reading.53,54
Longitudinal studies also show that the ability to rapidly access names for series of visual symbols such as numbers, objects, and, in particular, letters at school entry is predictive of word reading independently of phonological awareness, although these skills become less predictive past the early elementary grades.48,55 There is some evidence that performance on these rapid naming tasks is more strongly related to fluency and reading comprehension than is performance on phonological awareness tasks56 (see Vukovic & Siegel57 for an alternative view on rapid visual naming as a unique predictor of reading ability).
Subtyping studies show that some children with reading disability have a specific deficit in rapid naming that is not accompanied by deficits in phonological awareness.52 Lovett and colleagues58,59 demonstrated that children who have specific disabilities in reading rate have more circumscribed deficits in reading connected text, in spelling, and in some aspects of reading comprehension in comparison with children who have difficulty in phonological skills and word reading accuracy. Children who have deficits in both phonological awareness and rapid naming are reported to be more severely impaired in terms of their reading than are children with a deficit in only phonological awareness or rapid naming.59,60
The research literature on reading is replete with studies that relate reading skill to many other cognitive variables. The weakest of these predictors tends to be sensory and motor skills such as visual-perceptual processes and speech perception.50 More contemporary studies of sensory processes and reading61–63 have been criticized on several grounds, including the criteria used to classify children as reading disabled, the insensitivity of these measures for identifying children with reading disabilities or subtypes of reading disability, and the failure of this research to explain how sensory deficits are related to learning how to read or to difficulties in learning how to read.11,13 It remains to be seen whether newer proposals that combine theories of visual and auditory sensory processes to argue that reading disability reflects a general deficit in neuronal timing62 have validity.13
Between 15% and 40% of children identified as having a reading disability also have ADHD,64,65 and 25% to 40% of samples with children identified as having ADHD also have reading disability.66,67 Comorbid reading disability and ADHD leads to greater impairment in both reading-related and attention-related measures.68 Results of a large-scale study of comorbid conditions9 suggest that children with reading disability alone and those with ADHD alone can be distinguished by different cognitive characteristics, which is consistent with previous findings.30 Reading disability is strongly linked to deficits in phonological awareness, whereas ADHD is not.30 However, children with reading disability only, those with ADHD only, and those with reading disability and ADHD had a common deficit in slow and variable processing speed.9 It remains to be seen whether this common cognitive deficit is replicated in other samples, whether it is related to shared genetic effects, and whether it has consequences for intervention.
Neurobiological Factors
Research on reading disability has revealed that (1) there are subtle differences in several brain structures between individuals with reading disability and those without reading disability; (2) the brains of individuals with reading disability show different patterns of brain activation than those of nonaffected individuals during tasks requiring reading; and (3) intensive evidence-based reading intervention “normalizes” these patterns of activation in the brains of children with reading disability or in those at risk for reading disability. Also, genetic studies have revealed that there is a susceptibility to inherit varying levels of word reading ability. These findings are reviewed as follows.
Structural imaging studies of differences in brain structure in individuals with and without reading disability have produced mixed results. Despite difficulties associated with structural magnetic resonance imaging (MRI) studies including the use of different imaging methods, methods of analysis, and so forth, the data generally support the notion that there are subtle differences between children with and without reading disability and these differences are most likely to be found in those left hemisphere regions that support language.11,69
In contrast to anatomical studies with MRI, functional neuroimaging studies have yielded reliable differences in patterns of activation during phonological and reading tasks in the brains of individuals with and without reading disability that indicate impaired processing and disrupted connectivity mostly in regions of the left hemisphere, including the inferior frontal gyrus, the middle and superior temporal gyrus, and the angular gyrus.70 In studies of children using magnetic source imaging (MSI), Simos and colleagues71 demonstrated that children with and without reading disability did not differ in brain activation when listening to words but did differ when they read words. In children with no learning disability, occipital areas were activated, followed by ventral visual association cortices in both cerebral hemispheres and then particular areas in the left temporoparietal region (angular gyrus, Wernicke’s area, and superior temporal gyrus). When children with reading disability read words, the same time course of events was observed, but the temporoparietal areas of the right rather than the left hemisphere were activated. Such results suggest that it is not specific areas of brain that are “damaged” in reading disability but rather that the problem resides in the functional connectivity within the left hemisphere.72
Perhaps the most interesting findings in the functional imaging literature concern the effects of intervention on these patterns of brain activation. Simos and colleagues73 provided 80 hours of intensive phonologically based reading instruction to children and youth with significant word reading disabilities. MSI before intervention revealed the same pattern discussed previously for reading pronounceable nonwords. After intervention, word reading improved significantly, and there was increased activation in left hemisphere circuits for each child, as well as some reduction in right hemisphere activity (Aylward et al74 obtained similar findings with functional MRI and shorter intervention). Similar “normalization” of brain activation patterns have been found for young children considered at high risk for reading disability who responded to an early intervention program.75
Reading problems have long been observed to run in families, and the risk for a reading disability in a child with a reading-disabled parent is eight times that in the general population.76 Twin, family studies, and linkage studies all suggest that reading skill has a strong heritable component but that environmental influences are also significant.77 Of importance is that heritability estimates for reading skill are quite high both in individuals with and in those without reading disability78 and for several components of reading, including phonological and orthographic skills.79 A review of linkage findings is beyond the scope of this chapter, as is new research on unique and shared genetic effects for reading disability and ADHD, as well as other childhood disorders.6,80,81
READING COMPREHENSION
Core Cognitive Characteristics
The cognitive characteristics of reading comprehension have been studied in both typically developing children and in children with difficulties in reading comprehension. However, less is known about the core processes involved in learning how to comprehend what is read than about learning how to read words.40 It is clear that word reading and comprehension are dissociable in both typical and atypical development,82,83 although learning disabilities in both word reading and comprehension can be present simultaneously. Disabilities in word reading are easily identified before third grade, but disabilities in reading comprehension are more likely to be identified after third grade.84 Leach and colleagues84 showed that after third grade, of children identified with reading disability, about one third had specific word reading disability, one third had problems with both word reading and listening comprehension, and one third had problems with comprehension but not word reading. Some investigators have estimated rates of specific reading comprehension difficulties at between 5% and 10%.85
Studies of children with reading comprehension disabilities, but no word reading disability, suggest that phonological skills are not deficient86 but difficulties with inference making, text integration, metacognitive skills, and verbal working memory are common.87 In children with learning disabilities in word reading and comprehension, both phonological skills and these comprehension and memory skills may be deficient.88 In some children, more basic language deficits in both vocabulary knowledge and understanding of syntax limit comprehension of both oral and written language.89 Some researchers question whether children who read words well but have language comprehension problems actually have specific language impairment rather than reading comprehension disability per se. However, the majority of children with good word reading and poor comprehension do not meet the diagnostic criteria for specific language impairment.86 Reading comprehension disabilities were reviewed by Lyon and associates11 and Fletcher and colleagues.90
Math Disability
Math disabilities are as common as reading disabilities, and about half of all children with reading disability also have math disability.91 However, knowledge about the typical development of math skills, math disability, math interventions, and neurobiological factors related to math disability have not been as well studied as the same aspects of reading. One possibility for this imbalance is that reading disabilities have traditionally been considered to be of more cost to society in terms of both school achievement and general health and employment.92 However, human resource studies show that mathematical ability is as predictive of occupational success, productivity, and wages as is literacy.93
CORE COGNITIVE CHARACTERISTICS
The models and methods applied to the understanding of development of mathematical skills are the same models that are being applied to understand math disability, which reflects the beginning of a theoretical and methodological convergence in the field of math disabilities similar to that experienced earlier in the field of reading disabilities.33,94 The two most prominent theoretical positions about math disability arise from very different ways of explaining the origins of mathematical abilities.
One position95,96 arises from the view that, in contrast to reading, which is a relatively recent human achievement, an ability to understand magnitude or quantities and compare numbers is an ability that human and even nonhuman animals are born with. Although there is debate over the interpretation of some of the infant research, very young infants are sensitive to differences in the numerical values of small sets.97 Five-month-olds also appear sensitive to changes in very small set sizes involving adding and taking away.98 Preschoolers can judge whether one set or number is bigger or smaller than another set or number.99 Butterworth95 suggested that this sensitivity to number is the infant’s “starter kit” for later mathematical development and that deficits in these very basic mathematical abilities that are not influenced by environment or schooling underlie math disability. Proponents of this view do not argue that this is the only source of children’s difficulty in mathematics. For example, mathematical tasks that require language, such as word problem solving, would be influenced by language skills.
The second view is that mathematical skills in different domains are built from other, more basic or general cognitive systems, such as the language system,100 the visual-spatial system,101 and the central executive or attentional and working memory systems. Geary’s framework33,102 is the most comprehensive example of this view. In this framework, the skills that are important for the development of mathematical competence are the same ones proposed to be deficient in the development of math disabilities. According to this view, difficulties in math could arise in the language system, the visual-spatial system, the central executive system that sustains attention and inhibits irrelevant information, or any combination of these general cognitive systems. At present, there is some preliminary evidence for the framework,102 but there is as yet no coherent body of literature that would allow researchers to fully test the model or that pits this model against another math disability model.
Despite these theoretical differences in the field of math development and math disability, consensus has begun to emerge from studies about the core math skills that are consistently deficient in children with math disability. Regardless of whether there is a comorbid reading disability or an acquired or congenital brain injury in childhood, children with math disability have difficulties in the accuracy and speed with which they can compute answers to single-digit problems.103–105 This is often referred to as deficit in math fact retrieval. Before formal schooling, children learn to solve simple everyday problems through the use of counting strategies, such as adding two things to four things by counting 1, 2, 3, 4 and 5, 6 either on fingers or verbally. Practice with computing typically leads to a more developmentally sophisticated strategy in which the child counts up from the largest number (4, then 5, 6). Eventually, the child comes to associate the problem with the answer in memory such that he or she knows that 4 plus 2 is 6 (direct retrieval from memory). Accurate and fluent single-digit arithmetic is thought to be important for freeing cognitive resources during the learning and application of more complex procedures such as carrying and borrowing, and fluency in math fact retrieval is strongly related to accurate performance in multiple-digit arithmetic.104 In view of the evidence of deficits in math fact retrieval in math disabilities, current research on the early identification of math disability is focusing on the developmental precursors of math fact retrieval.106
As noted earlier, the combination of reading disability and math disability results in more severe symptoms in some areas of mathematics than does math disability alone. Young children with both reading disability and math disability make more counting errors when computing answers to single-digit problems than do children with only math disability,107 and they also have greater deficits in word problem solving.108,109
NEUROBIOLOGICAL FACTORS
Risk of math disorders in families with a child who has a math disability appears to be about 10 times that expected in the general population.110,111 Twin and adoption studies on math disabilities have yielded heritability estimates between 0.20 and 0.90.76 A large study of 7-year-old twins112 revealed that monozygotic twin correlations for mathematics performance indicated both substantial genetic influence and moderate environmental influence. The genetic correlations between mathematics and reading were high, which suggests that many of the genes that are predictive of individual differences in one academic domain are also predictive of individual differences in the other. Plomin and Kovas6 suggested a “generalist genes” theory of learning abilities and disabilities whereby genes that affect learning in an academic skill such as reading are largely, although not completely, the same genes that affect learning in mathematics. This theory is compatible with what is known about the substantial overlap in the two disorders. However, progress in understanding the cognitive phenotype of math ability and disability (e.g., similarities and differences in core cognitive correlates associated with math disability only versus both reading disability and math disability; potentially different types of math disability in different domains of mathematics), is crucial for informing behavioral genetic studies of mathematical skills.
Neuroimaging studies of math and math interventions in children with and without math disability are in the early stages. Different types of mathematical processing exhibit clear dissociations in adults with brain lesions and in functional neuroimaging studies with normal adults.113 These studies suggest that different neural circuits are involved in different types of mathematical processing. Dehaene and colleagues113,114 proposed that circuits in the parietal lobe are implicated in mathematical function and dysfunction: a bilateral intraparietal system for core quantitative processing, a region of the left angular gyrus for verbal processing of numbers, and a posterior superior parietal system for mathematical processing such as estimation that may require spatial attention. It is unknown whether the developing brain adheres to these same neural divisions during the acquisition of math skills, whether any or all of these neural circuits are involved in math disabilities, and whether math interventions that target different aspects of mathematical skill affect the operation of those circuits.
PREVENTION AND INTERVENTION
Prevention
As is true for many diseases and disorders, prevention is preferable to intervention or treatment in terms of costs both to individuals and to societies. Advances made in the science of learning disabilities since the 1990s have increasingly made prevention a viable and attractive option because children at high risk for reading disability (and perhaps math disability, too) can be identified in the preschool and very early school years. But are they identified? In addition to the conceptual and methodological limitations of the discrepancy method for identifying learning disabilities, the psychometric or measurement limitations of the tools used to assess discrepancies in intelligence and achievement render IQ-achievement discrepancy formulas unreliable before third grade. The consequence of these measurement limitations is that many affected children are not identified until third grade or later. Lyon and associates10 labeled this approach to the diagnosis and treatment of learning disabilities the “Wait to Fail” model. Early identification of children at risk for learning disabilities means that prevention can also be initiated earlier to narrow the achievement gap.5,10,115 Learning disability prevention programs have four main advantages over treatment programs that are instituted later in schooling. First, prevention can substantially reduce, although not eliminate, learning disabilities.39,116 Second, prevention programs are more effective for treating some components of learning disabilities. When evidence-based reading programs are used in kindergarten for at-risk students, many children learn to read both accurately and fluently. In contrast, when intervention programs, even those of high quality, begin in or after third grade, the ability to read words accurately can improve considerably, but fluency continues to lag behind.116 The third advantage of prevention over intervention programs is that prevention programs are less expensive because they can often be carried out in the general education classroom or in conjunction with general education programming. Fourth, prevention programs reduce the length of time that individual children struggle academically and emotionally with learning difficulties. The developmental-behavioral pediatrician has a very important role to play in the prevention of learning disabilities; this is discussed in the final section of the chapter.
Conceptual Approaches to Remediating Learning Disabilities
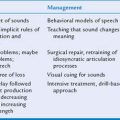
Since the 1990s, six conceptual approaches for treating the academic deficits of students with learning disabilities have garnered attention (Table 12-1). Three of these approaches, however, have netted limited effects for students with learning disabilities. The neuropsychological approach, which incorporates concepts from medical and psychoeducational theories, shares some shortcomings with these older models, including inadequate technical features of the assessment procedures117–119 and poor ecological validity.118 Moreover, although neuropsychological programs have proliferated since the 1990s, with advances in basic neuroscience, their importance for education has failed to materialize because implementation has not been linked to improved outcomes.11 The second approach with limited efficacy data focuses on intraindividual differences in cognitive processes, which calls for better delineation of the cognitive profiles associated with learning disabilities to inform treatment. The weaknesses of this model are its focus on test scores that describe the performance in isolation from classroom performance, its focus on behaviors that are removed from academic skills, and little empirical evidence to support utility.11 The third model, constructivism, stresses teacher empowerment, child-centered instruction, integration of listening, student interests and background, disavowal of subskills instruction, a view that children are naturally predisposed to learning, and reliance on unstructured activities from which learners construct their own meaning.120 This approach is demonstrably ineffective for students with learning disabilities.
TABLE 12-1 Conceptual Approaches to Remediating Learning Disabilities
| Approach | Orientation | Strengths/Limitations for Students with Learning Disabilities |
|---|---|---|
| Neuropsychological |
Each of the three remaining approaches, in contrast, is supported by persuasive research for remedying the academic deficits of students with learning disabilities. Cognitive models target information-processing abilities (e.g., memory or metacognition), as well as abilities more directly linked to academic skills (e.g., phonological awareness). Sometimes termed strategy instruction, these methods teach students to increase awareness of task demands, to use academic skills in a strategically optimal manner, and to apply strategies toward task completion so that content information can be acquired, manipulated, stored, retrieved, and expressed.118 When rooted in academic content, these approaches have proved effective.121–125
A second and related approach is the cognitive-behavioral model. It combines the methods of strategy instruction with behavioral principles. For example, self-regulated strategy development123,126 was designed to help students master higher-level cognitive processes (e.g., reading comprehension, math problem solving, narrative and expository writing) and strategies underlying effective academic performance; develop reflective, self-regulated use of these processes and strategies; and form positive attitudes about themselves and their academic capabilities. This and related approaches enhance reading, math, and writing performance.126,127
The third approach, the task-analytic model, emphasizes the influence of environment while deemphasizing underlying causal mechanisms or thought processes. The task-analytic model requires an operational learning objective, along with a detailed description and sequencing of the steps for achieving the objective.128 The task-analytic model is exemplified by direct instruction,129 which involves review of prerequisite learning; preview of goals; presentation of new concepts and material in small steps, with student practice after each step; provision of clear, explicit, detailed instructions and explanations; ongoing assessment of student understanding through teacher questioning; and systematic feedback and corrections. Task-analytic methods have been criticized because they control the teaching process in ways that minimize professional discretion; however, the methods have been shown to be effective.130,131
The most persuasive evidence for promoting academic learning among students with learning disabilities is currently provided by the task-analytic approach (e.g., direct instruction) and the cognitive or cognitive-behavioral approach (e.g., strategy instruction, like self-regulated strategy development). In a 1999 meta-analysis, for example, Swanson and colleagues131a classified studies into four intervention models: direct instruction, strategy instruction, direct instruction combined with strategy instruction, and “other” interventions. Direct instruction produced larger effect sizes than “other” interventions, as did strategy instruction. But combining direct instruction and strategy instruction yielded larger effect sizes in comparison with either method alone, which yielded moderate to large effects. A comprehensive review of programs within the task-analytic and cognitive/cognitive-behavioral approaches is not possible in this chapter. Instead, we illustrate the combined use of the task-analytic and strategy methods by describing one or two representative programs in each domain. The illustrative examples presented as follows are based on data from intervention research that has the following characteristics: random assignment, adequate description of interventions, adequate identification of the effective components of the intervention, long enough duration of intervention, control over prior interventions, measurement of teacher and contextual variables, and adequate generalization to real classrooms5 (also see National Reading Panel39 and Snow40 for methods for identifying evidence-based interventions in education).
Practices Illustrating Effective Remediation with the Task-Analytic and Cognitive/Cognitive-Behavioral Instructional Models
WORD-LEVEL READING SKILL
The longest continuous research program on reading remediation is directed by Maureen Lovett at The Hospital for Sick Children.132 She and her colleagues have developed and researched complementary programs that illustrate how direct instruction and strategy instruction can be combined synergistically to enhance the word-level skills of students with learning disabilities in reading. The program of phonological analysis and blending/direct instruction relies on the task-analytic method to explicitly and systematically teach children how to break apart words. Word identification strategy training (WIST) is a metacognitive program designed to teach word recognition through the application of strategies that facilitate transfer of word-level skills. Lovett’s research documents superior effects for the aligned use of the two programs.
A second research program, conducted by Torgesen and colleagues at Florida State University, also shows how comprehensive and intense programs, even with somewhat different emphases promote substantial improvement for students with learning disabilities in reading, when the programs integrate task-analytic and cognitive-behavioral/strategy instruction. For example, Torgesen and colleagues115 randomly assigned third, fourth, and fifth graders who scored below the third percentile in word recognition to one of two 8-week programs, each with 2 hours of daily instruction. Both interventions incorporated direct instruction and strategy instruction, including explicit instruction in the alphabetical principle, structured practice of new skills, and the cuing of appropriate strategies in context. Results showed significant improvement of about one standard deviation in word recognition and about two thirds of a standard deviation in comprehension; moreover, word recognition gains were maintained for 2 years. Of importance was that there was no difference in relative efficacy of the two programs (but, disappointingly, there was no improvement in fluency).
READING COMPREHENSION
Williams and associates also developed and assessed the efficacy of interventions that illustrate the combination of direct instruction and strategy instruction.133–135 For example, with the Theme-Identification Program,136 lessons are organized around a single story and include prereading discussion of the theme concept; reading the story aloud; discussing the important story information, with organizing questions as a guide (i.e., the “theme-scheme”); transfer and application of the theme to other story examples and real-life situations; review; and activity. The heart of the program is the “theme-scheme,” which provides a set of questions that organize the important story components to help students follow the plot and derive the theme. The teacher models how to answer these questions, and students gradually assume increasing responsibility for asking the questions and identifying the theme. The students also rehearse and commit to memory these questions so they can apply the theme-scheme guide independently to untaught stories. Toward the end of instruction, transfer instruction is provided explicitly, with two additional questions employed to help students generalize the theme to other relevant situations.
Williams and associates136 applied this program in second and third grade New York City classrooms, representing students with high, average, and low performance in relation to their classmates. Classrooms were assigned randomly to the Theme-Identification Program or to a more traditional comprehension program that emphasized vocabulary and plot. Students were assessed on a variety of acquisition and transfer measures. Results revealed that, as a function of the Theme-Identification Program, students acquired the concept of a theme and learned the theme-scheme questions. Of more importance was that on novel passages, students in the experimental condition were more skilled at identifying themes. Effects pertained to high, average, and low-achieving classmates, as well as to students with learning disabilities, in second and third grade. The methods illustrated how teachers can address a high-level comprehension skill (i.e., identification of a story’s theme) even among students with serious word-reading difficulties. Across the research of Williams and associates and other researchers working on remedying the comprehension difficulties of students with learning disabilities, results highlight how programs that incorporate direct “skills” instruction in combination with strategy instruction can be effective at promoting reading comprehension skill.
MATHEMATICS FACT RETRIEVAL AND PROCEDURAL SKILL
The majority of remediation research for students with learning disabilities in math focuses on fact retrieval and procedural math (i.e., multiple-digit computation). For example, Fuchs and colleagues137,138 cumulatively designed and tested a set of instructional components for enhancing students’ math competence. Three studies conducted at second through sixth grades addressed procedural math. Two additional studies assessed fact retrieval along with procedural math (i.e., multiple-digit computation and estimation) in kindergarten139 and first grade.140 Effects were assessed separately for students with learning disabilities and students not identified with learning disabilities who had low, average, and high initial achievement status. Across all four types of learners throughout the primary and intermediate grades, statistically significant effects resulted from a combination of (1) explicit, procedurally clear, conceptually based explanations; (2) pictorial representations of the math; (3) verbal rehearsal with gradual fading; and (4) timed practice on mixed problem sets, which systematically provided cumulative review of previously mastered problem types. Again, explicit instruction, combining the task-analytic and cognitive/strategy approaches, shows impressive gains for students with learning disabilities.
MATHEMATICAL PROBLEM SOLVING
Less attention, however, has been focused on complex math problem solving, in which problems incorporate irrelevant information and more varied syntactic structures and in which many problems require two or more computations for solution. This lack of attention to math problem solving, especially at the primary grades, is unfortunate for three reasons. First, for students with learning disabilities, a critical outcome of schooling is real-world math problem solving. Second, research even with typical students reveals the challenges associated with effecting math problem solving. Teachers cannot assume that interventions for promoting success with simple word problems will translate into improved math problem solving. Finally, despite severe challenges with foundational math skills,141 waiting for mastery of those foundational skills before working on math problem solving may create deficits in such work that are impossible to address later in school.
Fuchs and colleagues therefore focused on math problem solving in third grade with “Hot Math,” a program that combines task-analytic instruction to teach students solutions to word problems and strategy instruction to help students transfer these skills to more contextually rich and novel word problems. In a series of studies, Fuchs and colleagues142–144 used this framework to explicitly teach math problem solving. For example, they randomly assigned classrooms to four study conditions143: (1) teacher-designed instruction; (2) task-analytic solution instruction (20 sessions); (3) strategic instruction to transfer (20 sessions: half as much task-analytic solution instruction); and (4) task-analytic solution instruction with strategic instruction to transfer (30 sessions). Instruction was delivered over 16 weeks with strong fidelity, with teacher-directed and peer-mediated instructional arrangements, and effects were assessed on avariety of math problem solving measures. Results showed that task-analytic solution instruction was sufficient to improve performance on problems very similar to those used in intervention; that strategic instruction to transfer was necessary to enhance performance on less similar problems; and that for students with learning disabilities and other low-performing students, the full course of both components was most effective. For students with and without disability, the effect sizes were large. Thus, as is the case for reading and writing, effective interventions in the area of mathematics incorporate not only task-analytic skills instruction but also explicit instruction on strategies that facilitate transfer and maintenance of those skills.
Conclusions
LONG-TERM OUTCOMES
The Connecticut Longitudinal Study,3,145 which monitored children from kindergarten through grade 12, demonstrated that children with reading disabilities could be identified by 6 years of age and that they remained poorer readers than their peers with no learning disabilities at every other assessment point. Of importance is that reading scores did improve over time, but the difference between the individuals with and without reading disorders was maintained throughout development, so that fully 70% of the children identified with reading disorders by third grade were still identified as having reading disorders in high school. It is worth noting that these children were identified as learning disabled, and so they had received special education services. Although the Connecticut Longitudinal Study findings underline the fact that reading difficulties can be lifelong disorders, some individuals with reading disabilities are high achieving. In university samples of young adults with childhood diagnoses of reading disability, reading comprehension is better than word recognition, but the core deficit in phonological processing remains.146 Although many of these young adults are successful in school and in their occupations, they may continue to struggle more than their peers with reading-related tasks and may require supports into their college years (see Gerber et al147 for a study of the employment experiences of young American and Canadian adults with learning disabilities).
In the Connecticut Longitudinal Study, youths with reading disability did not differ from their typically developing peers with regard to other outcomes such as substance abuse or legal problems.145 In contrast, the Ottawa Language Study148 revealed an increased risk of substance abuse in adolescents with learning disorders and an elevated risk for poor behavioral outcomes in association with social and economic disadvantage, lower intelligence, and poorer academic and occupational achievements. These differences in nonreading outcomes across studies may be related to the high rate of language impairment in the Ottawa Language Study, which itself carries high risk for behavior disorder.149
THE ROLE OF THE DEVELOPMENTAL-BEHAVIORAL PEDIATRICIAN IN THE CLINICAL MANAGEMENT OF LEARNING DISABILITY
Assessment
 Has any one in the family (immediate and extended) ever had difficulty in school? In what subject or subjects? What are the educational attainments of family members?
Has any one in the family (immediate and extended) ever had difficulty in school? In what subject or subjects? What are the educational attainments of family members? If the child is of school age, did the child have any speech and language difficulties earlier in development? Was treatment provided? Are any assessment and treatment data available? (If the child is a preschooler or just entering the school system, the same questions apply. Children with speech and language impairment are at elevated risk for reading difficulties.7)
If the child is of school age, did the child have any speech and language difficulties earlier in development? Was treatment provided? Are any assessment and treatment data available? (If the child is a preschooler or just entering the school system, the same questions apply. Children with speech and language impairment are at elevated risk for reading difficulties.7)
 If the child is of school age, what are the child’s grades in language arts (which includes reading, language and reading comprehension, and oral and written expression) and mathematics (which may include arithmetic or number sense and numeration and other aspects of math such as geometry, measurement, problem solving, patterning and algebra, and data management) this year and in previous years? What are the teacher’s comments?
If the child is of school age, what are the child’s grades in language arts (which includes reading, language and reading comprehension, and oral and written expression) and mathematics (which may include arithmetic or number sense and numeration and other aspects of math such as geometry, measurement, problem solving, patterning and algebra, and data management) this year and in previous years? What are the teacher’s comments?
There are no medical diagnostic tests, including those that involve brain imaging, that can be used to diagnose learning disabilities or that have current practical clinical utility for assessing treatment benefits or making prognoses. For a child with a suspected learning disability, the most important tests are those that measure achievement in core academic domains. The developmental-behavioral pediatrician who is trained in psychometric measurement or the psychologist or assessment-literate teacher can assess these areas. For example, some developmental-behavioral pediatricians may employ academic screening measures, such as the Wide Range Achievement Test, 3rd Edition,150 that are relatively brief and easy to administer. This type of academic screening measure can be used for children from kindergarten on up to assess reading (letter and word recognition), spelling (writing letters and spelling words in response to dictation), and math (counting, reading numbers, simple verbal problems, and written computations).
However, such screening tools need to be followed by academic measures that more comprehensively assess the range of skills in core academic domains that are important for school functioning. These include measures of reading decoding, reading fluency, and reading comprehension; mathematics computations and math word problems; and written expression, such as handwriting, spelling, and composition. The Woodcock-Johnson III Tests of Achievement151 and the Wechsler Individual Achievement Test–Second Edition152 are reliable and well-validated measures of these academic skills that also account for variations in ethnicity and socioeconomic status.4
Assessments that include intelligence tests and measures of cognitive domains such as memory and general problem solving do not contribute much to the choice of appropriate interventions. For example, although working memory deficits are common in children with various learning disabilities,153 knowing about the type and level of the working memory deficit in children suspected of a learning disability does not inform the choice of intervention strategies. As discussed earlier, the choice of the intervention program needs to be based on an assessment that measures the specific academic deficit or deficits. This is powerful knowledge for practitioners to have about the relation between cognitive and academic assessment and intervention, and it carries two important practical and ethical consequences: Children need not undergo time-consuming psychometric testing for determining learning intervention needs, and funding can be directed toward intervention rather than assessment. In keeping with the earlier section on identification of learning disabilities, academic achievement tests such as these may be all that is needed to identify academic underachievement before a program of intervention is begun. Response to intervention (assuming that intervention is of sufficient intensity and duration) can be measured at appropriate intervals, with the same tests and also monitored by the teacher with brief and fairly frequent measures of progress (e.g. curriculum based measurement tools; see www.studentprogress.org).
Prevention
The pediatrician is often the first person who is consulted when a child has suspected developmental difficulties, and the pediatrician is also the professional who sees the child continuously across time. This places the pediatrician in a unique position with regard to early intervention for very young children who may be at risk for later learning disabilities. This intervention might involve referrals such as that for speech and language therapy for delayed language in toddlers and preschoolers. The developmental-behavioral pediatrician has an important role to play with regard to liaison with other health professionals and can provide support and education for parents in terms of prevention strategies. For example, information about learning disabilities in neurodevelopmental disorders such as spina bifida (see the following section) that is communicated to parents of such preschool children may result in careful monitoring of learning and early interventions that could prevent or reduce learning disabilities in these high-risk groups.
Understanding the Relation between Learning Disabilities and Comorbid Disorders
An important role of the medical practitioner is in the assessment and treatment of comorbid developmental disorders. For example, ADHD co-occurs with reading disability at a rate higher than that expected for the general population.30 This means that children presenting with any learning disability need to be thoroughly evaluated for ADHD and children with ADHD, for learning disability. Academic intervention and clinical drug trials for children with ADHD show that the learning disability and the ADHD necessitate treatments that are specific to each disorder154; that is, behavioral and medication treatments for the ADHD do not affect the learning disability, and academic treatments for the learning disability do not affect the behavioral symptoms of the ADHD. Whether combined treatments such as medication plus evidence-based reading interventions serve to potentiate treatment effects for children with comorbid ADHD and reading disability is a question of current research interest.155
Other disorders can co-occur with learning disabilities, including conduct disorder154 and speech and language disorders. These other disorders need to be addressed in their own right. For example, a comorbid language disorder would need to be assessed by a speech and language pathologist, and combined reading and language disorders may necessitate a somewhat different approach to treatment than either disorder alone.156
Several investigators have reported that children and adults with learning disability have a range of social-emotional difficulties, including poor social skills157 and substance abuse disorders,148 as well as depression, anxiety, and low self-esteem.158 One study revealed a reduction in depression in later grades for children who received academic interventions in first grade.159 A meta-analysis of depression and learning disability8 revealed that children with learning disabilities reported higher depression scores than did their nondisabled peers, but the reporting of clinical or severe depression was not elevated in students with learning disabilities. The authors cautioned that in clinical practice, diagnoses of depression are not made on the basis of depression inventories alone and that diagnoses need to be made by a qualified mental health professional and treated according to best practices for childhood depression.
It is also important to be aware of common neurodevelopmental disorders that are associated with higher than expected rates of learning disabilities. For example, very low birth weight is associated with learning disabilities even when such children have relatively spared cognitive and intellectual skills, and math may be particularly affected.160 Spina bifida,104 hydrocephalus from other etiologies,161 Turner syndrome,162 and the fragile X syndrome162 are all associated with relatively high rates of math disability, even when, in some of these neurodevelopmental disorders, word reading develops adequately. Traumatic head injury is associated with difficulties in acquiring word reading skills and math calculation skills, particularly for children who are injured during the preschool or very early school years.163,164 This relation of learning difficulties with an early age at injury is true for both severe and mild to moderate injuries.164 Standard academic achievement tests tend to underestimate the difficulties that children with traumatic brain injury have with academic skills in the classroom, which may reflect the influence of deficits in other cognitive systems such as memory, attention, and executive functions that support learning.165 Children with cancer, such as acute lymphoblastic leukemia, are also more affected by central nervous system treatment at younger ages of diagnosis. Difficulties have been found in math and in reading, and the manifestation of these learning disabilities in the classroom may be exacerbated by accompanying deficits in information processing speed, memory, attention, and visual-motor skills.166 Children with sickle cell disease are at high risk of learning disabilities, as well as other cognitive difficulties in domains such as attention, and this is true not only of those with overt strokes but also of children with clinically silent strokes.167 Furthermore, pain associated with the disease, medications to treat the pain, socioeconomic disadvantage, and behavioral issues may complicate how children with sickle cell disease function in the classroom, over and above the presence of learning disabilities and other cognitive deficits.
Intervention and Advocacy
An important role for the developmental-behavioral pediatrician is to convey information about evidence- based interventions for learning disabilities and, conversely, to be prepared to use professional knowledge to convey to parents which interventions are unlikely to work despite personal testimonials, advertisements, and media reports. This latter category of ineffective methods includes prosthetic devices and medications (e.g., colored lenses or colored overlays, medications for motion sickness/inner ear disease) or programs that do not directly address the academic disability (e.g., sensory integration training; learning styles or sensory modality). (See Chapter 8E.)
In view of the importance of the school in the progress of children with learning disabilities, it is necessary for the pediatric practitioner to (1) be familiar with local school resources and guidelines/criteria for accessing special education resources and (2) be able to refer parents to resources that will familiarize them with the processes that surround identification and access to special education or to prereferral programs designed to help students who are having learning difficulties.45 In other words, the developmental-behavioral pediatrician plays an advocacy role for children with learning disabilities and their families. One important thing to keep in mind is that identification as a student in need of special education is a legal process. This means that the developmental-behavioral pediatrician should know the legislation governing identification, as well as processes such as parent appeal. As mentioned earlier, alternatives to the traditional discrepancy formula for identifying learning disabilities have become acceptable under the Individuals with Disabilities Education Act. Because parents are often the best advocates for their children, the pediatrician may be key in educating some parents about their advocacy roles and the rules governing the process of identification.168 Information about legislation affecting children with learning disability and advocacy tools for health professionals, parents, teachers, and individuals with learning disability can be found on the Web sites of some of the learning disability organizations (e.g., Learning Disabilities Association of America, Learning Disabilities Association of Canada, National Center for Learning Disabilities).
The developmental-behavioral pediatrician may also play a more direct role in the identification process by writing a letter for the Identification Placement Review Committee meeting or the IEP meeting.168 The letter might include a summary of assessment and/or intervention data and pertinent developmental history information. It is also important for the medical practitioner to provide information about comorbid conditions or medical conditions such as those reviewed previously that could affect the child’s learning and that might also be used to establish eligibility for special education resources through a disabilities category other than learning disability.11 Information on the Identification Placement Review Committee and IEP can be found on several of the Web sites of the learning disability organizations listed earlier.
Finally, the developmental-behavioral pediatrician has an important role to play in terms of transition care as youths prepare to transfer from the child health system to the adult health system. As the health care professional who is often part of the child’s health care team from the child’s birth to adolescence, the developmental-behavioral pediatrician is well suited to transferring care to an appropriate primary care physician. The pediatrician may begin transition planning when the child is about 14 years of age, at a time when the education system is also charged with planning for transitions for further education and/or employment of youths with learning disabilities.169 For youths with learning disabilities, the pediatrician may promote self-advocacy and awareness of legislation governing the rights and entitlements of persons with disabilities.
CONCLUSION
As knowledge about the cognitive and neurobiological correlates of typical and atypical development of academic skills and effective interventions has grown, conceptualizations of learning disabilities have also changed. The application of science into practice and public policy is not always straightforward, and the field of learning disabilities is no exception to this general rule. However, a pediatric practitioner’s scientific knowledge about learning disabilities is crucial for the provision of evidence-based clinical management of children with learning disabilities.
1 U.S. Department of Education, Office of Special Education Program, Data Analysis System, 2004 IDEA Part B Child Count. Twenty-sixth Annual Report to Congress on the Implementation of the Individuals with Disabilities Education Act. Washington, DC: U. S. Government Printing Office, 2004.
2 Spreen O, Risser A, Edgell D. Developmental Neuropsychology. New York: Oxford University Press, 1995.
3 Shaywitz SE, Fletcher JM, Shaywitz BA. A conceptual model and definition of dyslexia: Findings emerging from the Connecticut Longitudinal Study. In: Beitchman JH, Cohen NJ, Konstantareas MM, et al, editors. Language, Learning, and Behavior Disorders. New York: Cambridge University Press; 1996:199-223.
4 Fletcher JM, Francis DJ, Morris R, et al. Evidence-based assessment of learning disabilities in children and adolescents. J Clin Child Adolesc Psychol. 2005;34:506-522.
5 Lyon GR, Fletcher JM, Fuchs LS, et al. Learning disabilities. In Mash E, Barkley R, editors: Treatment of Childhood Disorders, 2nd ed., New York: Guilford, 2006.
6 Plomin R, Kovas Y. Generalist genes and learning disabilities. Psychol Bull. 2005;131:592-617.
7 Bishop DVM, Snowling MJ. Developmental dyslexia and specific language impairment: Same or different? Psychol Bull. 2004;130:858-886.
8 Maag JW, Reid R. Depression among students with learning disabilities: Assessing the risk. J Learn Disabil. 2006;39:3-10.
9 Willcutt EG, Pennington BF, Olsen RK, et al. Neuropsychological analysis of comorbidity between reading disability and attention deficit hyperactivity disorder: In search of the common deficit. Dev Neuropsychol. 2005;27:35-78.
10 Lyon GR, Fletcher JM, Shaywitz SE, et al. Rethinking learning disabilities. In: Finn CEJr, Rotherham RAJ, Hokanson CRJr, editors. Rethinking Special Education for a New Century. Washington, DC: Thomas B. Fordham Foundation and Progressive Policy Institute; 2001:259-287.
11 Lyon GR, Fletcher JM, Barnes MA. Learning disabilities. In: Mash EJ, Barkley R, editors. Child Psychopathol-ogy. 2nd ed. New York: Guilford; 2003:520-588.
12 Hinshelwood J. Congenital Word Blindness. London: HK Lewis, 1917.
13 Lovett MW, Barron RW. Neuropsychological perspectives on reading development and developmental reading disorders. In: Segalowitz SJ, Rapin I, Boller F, Grafman J, editors. Handbook of Neuropsychology, vol 8: Child Neuropsychology, Part II. Amsterdam: Elsevier; 2003:671-716.
14 Chambers JG, Parrish T, Harr JJ: What are we spending on special education services in the United States, 1999–2000? Advance Report #1, Office of Special Education Program. Washington, DC: American Institutes for Research, March 2002. Available at: http://www.csef-air.org/publications/seep/nationa/AdvRpt1.pdf.
15 U.S. Office of Education. Assistance to states for education for handicapped children: Procedures for evaluating specific learning disabilities. Fed Regist. 1977;42:G1082-G1085.
16 U.S. Department of Education. Assistance to the states for the education of children with disabilities: Criteria for determining the existence of a specific learning disability, Part 300.541. Fed Regist. 1999;64:12405-12454.
17 Special Education: A Guide for Educators, Ministry of Education, Ontario, 2001. Available at: http://www.edu.gov.on.ca/eng/general/elemsec/speced/handbook.pdf.
18 American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed, International Version. Washington, DC: American Psychiatric Association, 1994.
19 World Health Organization. The ICD-10 Classification of Mental and Behavioral Disorders: Clinical Descriptions and Diagnostic Guidelines. Geneva: World Health Organization, 1992.
20 Rapoport JL, Ismond DR. DSM-IV Training Guide for Diagnosis of Childhood Disorders. Philadelphia: Brunner/Mazel, 1996.
21 Fletcher JM, Lyon GR, Barnes MA, et al. Classification of learning disabilities: An evidence-based evaluation. In: Bradley R, Danielson L, Hallahan D, editors. Identification of Learning Disabilities: Research in Practice. Mahwah, NJ: Erlbaum; 2002:185-250.
22 Stuebing KK, Fletcher JM, LeDoux JM, et al. Validity of discrepancy classifications of reading difficulties: A meta-analysis. Am Educ Res J. 2002;39:469-518.
23 Stanovich KE, Siegel LS. Phenotypic performance profiles of children with reading disabilities: A regression-based test of the phonological-core variable difference model. J Educ Psychol. 1994;86:24-53.
24 Francis DJ, Shaywitz SE, Stuebing KK, et al. Developmental lag versus deficit models of reading disability: A longitudinal, individual growth curves analysis. J Educ Psychol. 1996;88:3-17.
25 Vellutino FR, Scanlon DM, Lyon GR. Differentiating between difficult-to-remediate and readily remediated poor readers: More evidence against the IQ-achievement discrepancy definition for reading disability. J Learn Disabil. 2000;33:223-238.
26 Elliot SN, Fuchs LS. The utility of curriculum-based measurement and performance assessment as alternatives to traditional intelligence and achievement tests. School Psychol Rev. 1997;26:224-233.
27 Wadsworth SJ, Olson RK, Pennington BF, et al. Differential genetic etiology of reading disability as a function of IQ. J Learn Disabil. 2000;33:192-199.
28 Francis DJ, Fletcher JM, Stuebing KK, et al. Psychometric approaches to the identification of learning disabilities. Test scores are not sufficient. J Learn Disabil. 2005;38:545-552.
29 Shaywitz SE, Escobar MD, Shaywitz BA, et al. Evidence that dyslexia may represent the lower tail of a normal distribution of reading ability. N Engl J Med. 1992;326:145-150.
30 Fletcher JM, Shaywitz SE, Shaywitz BA. Comorbidity of learning and attention disorders: Separate but equal. Pediatr Clin North Am. 1999;46:885-897.
31 Shankweiler D, Lundquist E, Katz L, et al. Comprehension and decoding: Patterns of association in children with reading difficulties. Sci Stud Read. 1999;3:69-94.
32 Fuchs LS, Fuchs D, Stuebing K, Fletcher JM, et al: Calculation and problem-solving skill: Are they shared or distinct aspects of mathematical problem solving? Manuscript submitted for publication.
33 Geary DC. Mathematical disabilities: Cognitive, neuropsychological, and genetic components. Psychol Bull. 1993;114:345-362.
34 Hart B, Risley TR. Meaningful Differences in the Everyday Experience of Young American Children. Baltimore: Paul H. Brookes, 1999.
35 Whitehurst GJ, Massetti GM. How well does Head Start prepare children to learn to read? In: Zigler E, Styfco SJ, editors. The Head Start Debates. Baltimore: Paul H. Brooks; 2004:251-262.
36 Case R, Griffin Kelly WM. Socioeconomic gradients in mathematical ability and their responsiveness to intervention during early childhood. In: Keating DP, Hertzman C, editors. Developmental Health and the Wealth of Nations. New York: Guilford; 1999:21-40.
37 Whitehurst GJ, Lonigan C. Child development and emergent literacy. Child Dev. 1998;69:848-872.
38 Starkey P, Klein A, Wakeley A. Enhancing young children’s mathematical knowledge through a pre-kindergarten mathematics intervention. Early Child Res Q. 2004;19:99-120.
39 National Reading Panel. Teaching Children to Read: An Evidence-Based Assessment of the Scientific Research Literature on Reading and Its Implications for Reading Instruction. Washington, DC: National Institute of Child Health and Human Development, 2000.
40 Snow CE. Reading for Understanding: Toward an R & D Program in Reading Comprehension. Santa Monica, CA: RAND Corporation, 2002.
41 Berninger VW, Abbott RD. Redefining learning disabilities: Moving beyond aptitude achievement discrepancies to failure to respond to validated treatment protocols. In: Lyon GR, editor. Frames of Reference for the Assessment of Learning Disabilities: New Views on Measurement Issues. Baltimore: Paul H. Brookes; 1994:163-183.
42 Fuchs LS, Fuchs D. Treatment validity: A unifying concept for reconceptualizing the identification of learning disabilities. Learn Disabil Res Prac. 1998;13:204-219.
43 Vellutino FR, Scanlon DM. Phonological coding, phonological awareness, and reading ability: Evidence from a longitudinal and experimental study. Merrill Palmer Q. 1987;33:321-363.
44 Heller KA, Holtzman WH, Messick S, editors. Placing Children in Special Education: A Strategy for Equity. Washington, DC: National Academies Press, 1982.
45 Fletcher JM, Lyon GR. Learning disabilities. In Maria B, editor: Current Management in Child Neurology, 3rd ed., Hamilton, Ontario: BC Decker, 2005.
46 Liberman IY, Shankweiler D, Liberman AM. The alphabetic principle and learning to read. In: Shankweiler D, Liberman IY, editors. Phonology and Reading Disability: Solving the Reading Puzzle. Ann Arbor, MI: University of Michigan Press; 1989:1-33.
47 Adams MJ. Beginning to Read: Thinking and Learning about Print. Cambridge, MA: MIT Press, 1990.
48 Wagner RK, Torgesen JK, Rashotte CA, et al. Changing relations between phonological processing abilities and word-level reading as children develop from beginning to skilled readers: A five year longitudinal study. Dev Psychol. 1997;33:468-479.
49 Torgesen JK, Wagner RK, Rashotte CA, et al. Contributions of phonological awareness and rapid automatic naming ability to the growth of word-reading skills in second- to fifth-grade children. Sci Stud Read. 1997;1:161-185.
50 Scarborough HS. Early identification of children at risk for reading disabilities. In: Shapiro BK, Accardo PJ, Capute AJ, editors. Specific Reading Disability: A View of the Spectrum. Timonium, MD: York Press; 1998:75-119.
51 Stanovich KE. Explaining the differences between the dyslexic and the garden-variety poor reader: The phonological-core variable-difference model. J Learn Disabil. 1988;21:590-604.
52 Morris RD, Stuebing KK, Fletcher JM, et al. Subtypes of reading disability: Variability around a phonological core. J Educ Psychol. 1998;90:1-27.
53 Torgesen JK, Wagner RK, Rashotte CA, et al. Preventing reading failure in young children with phonological processing disabilities: Group and individual responses to instruction. J Educ Psychol. 1999;91:579-593.
54 Vellutino FR, Scanlon DM, Sipay ER, et al. Cognitive profiles of difficult-to-remediate and readily remediated poor readers: Early intervention as a vehicle for distinguishing between cognitive and experiential deficits as basic causes of specific reading disability. J Educ Psychol. 1996;88:601-638.
55 Manis FR, Seidenberg MS, Doi L. See Dick RAN: Rapid naming and the longitudinal prediction of reading subskills in first and second graders. Sci Stud Read. 1999;3:129-157.
56 Bowers PG, Sunseth K, Golden J. The route between rapid naming and reading progress. Sci Stud Read. 1999;3:31-53.
57 Vukovic RK, Siegel LS. The double deficit hypothesis: A comprehensive review of the evidence. J Learn Disabil. 2006;39:25-47.
58 Lovett MW. A developmental approach to reading disability: Accuracy and speed criteria of normal and deficit reading children. Child Dev. 1987;58:234-260.
59 Lovett MW, Steinbach KA, Frijters JC. Remediating the core deficits of developmental reading disability: A double deficit perspective. J Learn Disabil. 2000;33:334-358.
60 Wolf M, Bowers PG. The double-deficit hypothesis for the developmental dyslexias. J Educ Psychol. 1999;91:415-438.
61 Cestnick L, Coltheart M. The relationship between language-processing and visual-processing deficits in developmental dyslexia. Cognition. 1999;71:231-255.
62 Stein JF. The neurobiology of reading difficulties. In: Wolf M, editor. Dyslexia, Fluency, and the Brain. Baltimore: York Press, 2001.
63 Tallal P, Miller SL, Jenkins WM, et al. The role of temporal processing in developmental language-based learning disorders: Research and clinical implications. In: Blachman BA, editor. Foundations of Reading Acquisition and Dyslexia: Implications for Early Intervention. Mahwah NJ: Erlbaum; 1997:49-66.
64 Shaywitz BA, Fletcher JM, Shaywitz SE. Defining and classifying learning disabilities and attention-deficit/hyperactivity disorder. J Child Neurol. 1995;10:50-57.
65 Willcutt EG, Pennington BF. Comorbidity of reading disability and attention-deficit/hyperactivity disorder: Differences by gender and subtype. J Learn Disabil. 2000;33:179-191.
66 Dykman RA, Ackerman PT. Attention deficit disorder and specific reading disability: Separate but often overlapping disorders. J Learn Disabil. 1991;24:96-103.
67 Semrud-Clikeman M, Biederman J, Sprich-Buckminster S, et al. Comorbidity between ADDH and learning disability: A review and report in a clinically referred sample. J Am Acad Child Adolesc Psychiatry. 1992;31:439-448.
68 Willcutt EG, Pennington BF, Boada R, et al. A comparison of the cognitive deficits in reading disability and attention-deficit/hyperactivity disorder. J Abnorm Psychol. 2001;110:157-172.
69 Filipek PA. Neuroimaging in the developmental disorders: The state of the science. J Child Psychol Psychiatry. 1999;40:113-128.
70 Shaywitz SE, Pugh KR, Jenner AR, et al. The neurobiology of reading and reading disability (dyslexia). Kamil ML, Mosenthal PB, Pearson PD, et al, editors. Handbook of Reading Research. Mahwah, NJ: Erlbaum; 2000;3:229-249.
71 Simos PG, Breier JI, Fletcher JM, et al. Brain activation profiles in dyslexic children during nonword reading: A magnetic source imaging study. Neurosci Rep. 2000;290:61-65.
72 Pugh KR, Mencl WE, Shaywitz BA, et al. The angular gyrus in developmental dyslexia: Task-specific differences in functional connectivity within posterior cortex. Psychol Sci. 2000;11:51-56.
73 Simos PG, Fletcher JM, Bergman E, et al. Dyslexia-specific brain activation profiles becomes normal following successful remedial training. Neurology. 2000;58:1-10.
74 Aylward EH, Richards TL, Berninger VW, et al. Instructional treatment associated with changes in brain activation in children with dyslexia. Neurology. 2003;22:212-219.
75 Simos PG, Fletcher JM, Sarkari S, et al. Early development of neurophysiological processes involved in normal reading and reading disability: A magnetic source imaging study. Neuropsychology. 2005;19:787-798.
76 Pennington BB. Dyslexia as a neurodevelopmental disorder. In: Tager-Flusberg H, editor. Neurodevelopmental Disorders. Cambridge, MA: MIT Press; 1999:307-330.
77 Grigorenko EL. Developmental dyslexia: An update on genes, brains, and environments. J Child Psychol Psychiatry. 2001;42:91-125.
78 Alarcon M, DeFries JC. Reading performance and general cognitive ability in twins with reading difficulties and control pairs. Pers Individ Dif. 1997;22:793-803.
79 Gayan J, Olson RK. Genetic and environmental influences on orthographic and phonological skills in children with reading disabilities. Dev Neuropsychol. 2001;20:483-507.
80 Grigorenko EL, Wood FB, Golovyan L, et al. Continuing the search for dyslexia genes on 6p. Am J Med Genet B Neuropsychiatr Genet. 2003;118B:89-98.
81 Gayan J, Willcutt EG, Fisher SE, et al. Bivariate linkage scan for reading disability and attention-deficit/hyperactivity disorder localizes pleiotropic loci. J Child Psychol Psychiatry. 2005;46:1045-1056.
82 Oakhill J, Cain K, Bryant PE. The dissociation of word reading and text comprehension: Evidence from component skills. Lang Cogn Proc. 2003;18:443-468.
83 Barnes MA. The decoding-comprehension dissociation in the reading of children with hydrocephalus: A reply to Yamada. Brain Lang. 2002;80:260-263.
84 Leach JM, Scarborough HS, Rescorla L. Late-emerging reading disabilities. J Educ Psychol. 2003;95:211-224.
85 Cornoldi C, DeBeni R, Pazzaglia F. Profiles of reading comprehension difficulties: An analysis of single cases. In: Cornoldi C, Oakhill J, editors. Reading Comprehension Difficulties: Processes and Intervention. Mahwah, NJ: Erlbaum; 1996:113-136.
86 Nation K, Clarke P, Marshall M, et al. Hidden language impairments in children: Parallels between poor reading comprehension and speech and language impairment? J Speech Lang Hear Res. 2004;47:199-211.
87 Cain K, Oakhill JV, Bryant P. Phonological skills and comprehension failures: A test of the phonological processing deficits hypothesis. Read Write. 2000;13:31-56.
88 Barnes MA, Dennis M. Reading comprehension deficits arise from diverse sources: Evidence from readers with and without developmental brain pathology. In: Cornoldi C, Oakhill J, editors. Reading Comprehension Difficulties. Hillsdale, NJ: Erlbaum; 1996:251-278.
89 Nation K, Clarke P, Snowling MJ. General cognitive ability in children with poor reading comprehension. Br J Educ Psychol. 2002;72:549-560.
90 Fletcher JM, Lyon GR, Fuchs LS, et al. Learning Disabilities: From Identification to Intervention. New York: Guilford, 2006.
91 Shalev RS, Auerbach J, Manor O, et al. Developmenta l dyscalculia: Prevalence and prognosis. Eur Child Adolesc Psychiatry. 2000;9:58-64.
92 Fleishner JE. Diagnosis and assessment of mathematics learning disabilities. In: Lyon GR, editor. Frames of Reference for the Assessment of Learning Disabilities: New Views on Measurement Issues. Baltimore: Paul H. Brookes; 1994:441-458.
93 Rivera-Batiz FL. Quantitative literacy and the likelihood of employment among young adults in the United States. J Hum Resour. 1992;27:313-328.
94 Jordan NC, Hanich LB, Kaplan D. A longitudinal study of mathematical competencies in children with specific math difficulties versus children with comorbid mathematics and reading difficulties. Child Dev. 2003;74:834-850.
95 Butterworth B. What Counts: How Every Brain is Hardwired for Math. New York: Simon & Schuster, 1999.
96 Butterworth B. Developmental dyscalculia. In: Campbell JID, editor. Handbook of Mathematical Cognition. New York: Psychology Press; 2005:455-467.
97 Starkey P, Spelke ES, Gelman R. Numerical abstraction by human infants. Cognition. 1990;36:97-127.
98 Wynn K. Addition and subtraction by human infants. Nature. 1992;358:749-750.
99 Ginsberg HP, Klein A, Starkey P. The development of children’s mathematical thinking: Connecting research with practice. In: Siegel IE, Renninger KA, Damon W, editors. Handbook of Child Psychology, vol 4: Child Psychology in Practice. 5th ed. New York: Wiley; 1998:401-476.
100 Gelman R, Butterworth B. Number and language: How are they related? Trends Cogn Sci. 2005;9:6-10.
101 Rourke BP. Arithmetic disabilities, specific and otherwise: A neuropsychological perspective. J Learn Disabil. 1993;26:214-226.
102 Geary DC, Hoard MK. Learning disabilities in arithmetic and mathematics: Theoretical and empirical perspectives. In: Campbell JID, editor. Handbook of Mathematical Cognition. New York: Psychology Press; 2005:253-267.
103 Ashcraft MH, Yamashita TS, Aram DM. Mathematics performance in left and right brain-lesioned children and adolescents. Brain Cogn. 1992;19:208-252.
104 Barnes MA, Wilkinson M, Khemani E, et al. Arithmetic processing in children with spina bifida: Calculation accuracy, strategy use, and fact retrieval fluency. J Learn Disabil. 2006;39:174-187.
105 Jordan NC, Hanich LB, Kaplan D. Arithmetic fact mastery in young children: A longitudinal investigation. J Exp Child Psychol. 2003;85:103-119.
106 Gersten RM, Jordan NC, Flojo JR. Early identification and interventions for students with mathematical difficulties. J Learn Disabil. 2005;38:293-304.
107 Geary DC, Hamson CO, Hoard MK. Numerical and arithmetical cognition: A longitudinal study of process and concept deficits in children with learning disability. J Exp Child Psychol. 2000;77:236-263.
108 Fuchs LS, Fuchs D. Mathematical problem-solving profiles of students with mathematics disabilities with and without comorbid reading disabilities. J Learn Disabil. 2002;35:563-573.
109 Hanich L, Jordan N, Kaplan D, et al. Performance across different areas of mathematical cognition in children with learning difficulties. J Educ Psychol. 2001;93:615-626.
110 Gross-Tsur V, Manor O, Shalev RS. Developmental dyscalculia: Prevalence and demographic features. Dev Med Child Neurol. 1996;38:25-33.
111 Shalev RS, Manor O, Kerem B, et al. Developmental dyscalculia is a familial learning disability. J Learn Disabil. 2001;34:59-65.
112 Kovas Y, Harlaar N, Petrill SA, et al. “Generalist genes” and mathematics in 7-year-old twins. Intelligence. 2005;33:473-489.
113 Dehaene S, Spelke E, Pinel P, et al. Sources of mathematical thinking: Behavioral and brain-imaging evidence. Science. 1999;284:970-974.
114 Dehaene S, Piazza M, Pinel P, et al. Three parietal circuits for number processing. In: Campbell JID, editor. Handbook of Mathematical Cognition. New York: Psychology Press; 2005:433-453.
115 Torgesen JK, Alexander AW, Wagner RK, et al. Intensive remedial instruction for children with severe reading disabilities: Immediate and long-term outcomes from two instructional approaches. J Learn Disabil. 2001;34:33-58.
116 Torgesen JK. Lessons learned from research on interventions for students who have difficulty learning to read. In: McCardle P, Chhabra V, editors. The Voice of Evidence in Reading Research. Baltimore: Paul H. Brookes; 2004:355-382.
117 Brown AL, Campione J. Psychological theory and the study of learning disabilities. Am Psychol. 1986;41:14-21.
118 Lyon GR, Moats LC. Critical issues in the instruction of the leaning disabled. J Consult Clin Psychol. 1988;56:830-835.
119 Torgesen JK. Empirical and theoretical support for direct diagnosis of learning disabilities by assessment of intrinsic processing weaknesses. In: Bradley R, Danielson L, Hallahan D, editors. Identification of Learning Disabilities: Research to Practice. Mahwah, NJ: Erlbaum; 2002:565-650.
120 Reid DK, Hresko WP. A Cognitive Approach to Learning Disabilities. New York: McGraw-Hill, 1981.
121 Englert CS, Hiebert EH, Stewart SR. Spelling unfamiliar words by an analogy strategy. J Spec Educ. 1986;19:291-306.
122 Fuchs LS, Fuchs D, Hamlett CL, et al. Explicitly teaching for transfer: Effects on the mathematical problem solving performance of students with disabilities. Learn Disabil Res Prac. 2002;17:90-106.
123 Graham S, Harris K. Addressing problems in attention, memory, and executive function. In: Lyon GR, Krasnegor NA, editors. Attention, Memory, and Executive Function. Baltimore: Paul H. Brookes; 1996:349-366.
124 Palinscar AS, Brown DA. Enhancing instructional time through attention to metacognition. J Learn Disabil. 1987;20:66-75.
125 Vaughn S, Klingner JK. Teaching reading comprehension to students with learning disabilities: Instructional/intervention frameworks. In: Stone CA, Silliman ER, Apel K, Ehren BJ, et al, editors. Handbook of Language and Literacy Development and Disorders. New York: Guilford, 2004.
126 Graham S, Harris KR. Students with learning disabilities and the process of writing: A meta-analysis of SRSD studies. In: Swanson HL, Harris KR, Graham S, editors. Handbook of Learning Disabilities. New York: Guilford; 2003:323-344.
127 Case LP, Harris KR, Graham S. Improving the mathematical problem-solving skills of students with learning disabilities: Self-regulated strategy development. J Spec Educ. 1992;26:1-19.
128 Hallahan DP, Kauffman J, Lloyd J. Introduction to Learning Disabilities. Needham Heights, MA: Allyn & Bacon, 1996.
129 Rosenshine B, Stevens R. Teaching functions. In: Wittrock MC, editor. Handbook of Research on Teaching. 3rd ed. New York: Macmillan; 1986:376-391.
130 Adams G, Carnine D. Direct instruction. In: Swanson HL, Harris KR, Graham S, editors. Handbook of Learning Disabilities. New York: Guilford; 2003:403-416.
131 Gersten RM, White WA, Falco R, et al. Teaching basic discriminations to handicapped and non-handicapped individuals through a dynamic presentation of instructional stimuli. Anal Interven Dev Disabil. 1982;2:305-317.
131a Swanson HL. Interventions for students with Learning Disabilities. New York: Guilford, 1999.
132 Lovett MW, Lacerenza L, Borden SL, et al. Components of effective remediation for developmental reading disabilities: Combining phonological and strategy-based instruction to improve outcomes. J Educ Psychol. 2000;92:263-283.
133 Wilder AA, Williams JP. Students with severe learning disabilities can learn higher-order comprehension skills. J Educ Psychol. 2001;93:268-278.
134 Williams JP. Teaching text structure to improve reading comprehension. In: Swanson HL, Harris KR, Graham S, editors. Handbook of Learning Disabilities. New York: Guilford; 2003:293-305.
135 Williams JP, Brown LG, Silverman AK, et al. An instructional program for adolescents with learning disabilities in the comprehension of narrative themes. Learn Disabil Q. 1994;17:205-221.
136 Williams JP. Using the Theme Scheme to improve story comprehension. In: Block CC, Pressley M, editors. Comprehension Instruction: Research-Based Best Practices. New York: Guilford; 2002:126-139.
137 Fuchs LS, Fuchs D, Hamlett CL, et al. Class wide curriculum-based measurement: Helping general educators meet the challenge of student diversity. Except Child. 1994;60:518-537.
138 Fuchs LS, Fuchs D, Phillips CL, et al. General educators’ specialized adaptation for students with learning disabilities. Except Child. 1995;61:440.
139 Fuchs LS, Fuchs D, Karns K. Enhancing kinder-gartners’ mathematical development: Effects of peer-assisted learning strategies. Elem Sch J. 2001;101:494-510.
140 Fuchs LS, Fuchs D, Yazdian L, et al. Enhancing first-grade children’s mathematical development with peer-assisted learning strategies. Sch Psychol Rev. 2002;31:569-584.
141 Jordan NC, Hanich LB. Mathematical thinking in second-grade children with different forms of LD. J Learn Disabil. 2000;33:567-578.
142 Fuchs LS, Fuchs D, Prentice K, et al. Enhancing third-grade students’ mathematical problem solving with self-regulated learning strategies. J Educ Psychol. 2003;95:306-315.
143 Fuchs LS, Fuchs D, Prentice K, et al. Explicitly teaching for transfer: Effects on third-grade students’ mathematical problem solving. J Educ Psychol. 2003;95:293-304.
144 Fuchs LS, Fuchs D, Prentice K, et al. Enhancing mathematical problem solving among third-grade students with schema-based instruction. J Educ Psychol. 2004;96:635-647.
145 Shaywitz SE, Fletcher JM, Holahan JM, et al. Persistence of dyslexia: The Connecticut Longitudinal Study at adolescence. Pediatrics. 1999;104:1351-1359.
146 Bruck M. Outcomes of adults with childhood histories of dyslexia. In: Hume C, Joshi RM, editors. Reading and Spelling: Development and Disorders. Mahwah, NJ: Erlbaum; 1998:179-200.
147 Gerber PJ, Price LA, Mulligan R, et al. Beyond transition: A comparison of the employment experiences of American and Canadian Adults with LD. J Learn Disabil. 2004;37:283-291.
148 Beitchman JH, Wilson B, Douglas L, et al. Substance use disorders in young adults with and without LD: Predictive and concurrent relationships. J Learn Disabil. 2001;34:317-332.
149 Tomblin JB, Zhang X, Buckwalter P, et al. The association of reading disability, behavioral disorders, and language impairment among second-grade children. J Child Psychol Psychiatry. 2000;41:473-482.
150 Wilkinson GS. The Wide Range Achievement Test, 3rd ed. New York: Academic Press, 1993.
151 Woodcock RW, McGrew KS, Mather N. Woodcock-Johnson III Tests of Achievement. Itasca, IL: Riverside, 2001.
152 Wechsler D. Wechsler Individual Achievement Test-II. Examiner’s Manual. 2nd ed. San Antonio, TX: Psychological Corporation; 2001.
153 Gathercole SE, Pickering SJ. Working memory deficits in children with low achievements in the national curriculum at 7 years of age. Br J Educ Psychol. 2000;70:177-194.
154 Rabiner DL, Malone PS, the Conduct Problems Prevention Research Group. The i mpact of tutoring on early reading achievement for children with and without attention problem. J Abnorm Child Psychol. 2004;32:273-284.
155 Tannock R, Lovett M, Martinussen R, et al: Intervention for ADHD with comorbid reading disorders: Combined modality approach (Abstract, p. 46). Scientific Proceedings of the 2005 Joint Annual Meeting of the American Academy of Child & Adolescent Psychiatry and the Canadian Academy of Child & Adolescent Psychiatry, Toronto, October 18–23, 2005.
156 Bishop DVM. Uncommon Understanding: Development and Disorders of Language Comprehension in Children. Hove, East Sussex, UK: Psychology Press, 1997.
157 Kavale KA, Forness SR. Social skills deficits and learning disabilities: A meta-analysis. J Learn Disabil. 1996;29:226-237.
158 Johnson DJ, Blalock J, editors. Adults with Learning Disabilities. Orlando, FL: Grune & Stratton, 1987.
159 Kellam SG, Rebok GW, Mayer LS, et al. Depressive symptoms over first grade and their response to a developmental epidemiologically based preventive trial aimed at improving achievement. Dev Psycho-pathol. 1994;6:463-481.
160 Litt J, Taylor HG, Klein N, et al. Learning disabilities in children with very low birthweight: Prevalence, neuropsychological correlates, and educational interventions. J Learn Disabil. 2005;38:130-141.
161 Barnes MA, Pengelly S, Dennis M, et al. Mathematics skills in good readers with hydrocephalus. J Int Neuropsychol Soc. 2002;8:72-82.
162 Mazzocco MMM, McCloskey M. Math performance in girls with Turner or fragile X syndrome. In: Campbell JID, editor. Handbook of Mathematical Cognition. New York: Psychology Press; 2005:269-297.
163 Barnes MA, Dennis M, Wilkinson M. Reading after closed head injury in childhood: Effects on decoding, fluency, and comprehension. Dev Neuropsychol. 1999;15:1-24.
164 Ewing-Cobbs L, Barnes MA, Fletcher JM, et al. Modeling of longitudinal academic achievement scores after pediatric traumatic brain injury. Dev Neuropsychol. 2004;25:107-134.
165 Barnes MA, Ewing-Cobbs L, Fletcher JM: Mathematical disabilities in congenital and acquired neurodevelopmental disorders. In Berch D, Mazzocco M, eds: New York: Brookes Publishing, in press.
166 Armstrong DF, Briery BG. Childhood cancer and the school. In: Brown RT, editor. Handbook of Pediatric Psychology in School Settings. Mahwah, NJ: Erlbaum; 2004:263-281.
167 Bonner MJ, Hardy KK, Elzell E, et al. Hematological disorders: Sickle cell disease and hemophilia. In: Brown RT, editor. Handbook of Pediatric Psychology in School Settings. Mahwah, NJ: Erlbaum; 2004:241-261.
168 The pediatrician’s role in development and implementation of an Individual Education Plan (IEP) and/or an Individual Family Service Plan (IFSP). American Academy of Pediatrics. Committee on Children with Disabilities. Pediatrics. 1999;104:124-127.
169 American Academy of Pediatrics Committee on Children with Disabilities. The role of the pediatrician in transitioning children and adolescents with developmental disabilities and chronic illnesses from school to work or college. American Academy of Pediatrics. Committee on Children with Disabilities. Pediatrics. 2000;106:854-856.
* Supported by grants from the National Institute of Child Health and Human Development, P01 HD46261, Cognitive, Instructional, and Neuroimaging Factors in Math, and from the Canadian Language and Literacy Research Network, Comprehension in Englishand French-speaking Children: Core Processes & Predictors.