Kinesiology of Walking
Walking (ambulation) serves an individual’s basic need to move from place to place and is therefore one of the most common activities that people do on a daily basis. Ideally, walking is performed both efficiently, to minimize fatigue, and safely, to prevent falls and associated injuries.188 Years of practice provide a healthy person with the control needed to ambulate while carrying on a conversation, looking in various directions, and even handling obstacles and other destabilizing forces with minimal effort.
Although a healthy person makes walking seem effortless, the challenge of ambulation can be recognized by looking at individuals at both ends of the lifespan (Figure 15-1). Early in life, the young child needs 11 to 15 months to learn how to stand and walk.67,180 Once on their feet, children will refine their gait so that it visually resembles a mature adult walking pattern by 4 to 5 years of age,26,172,178,179,180 with further refinement taking place over possibly several more years.* Late in life, walking often becomes an increasingly greater challenge. Because of decreased strength, decreased balance, or disease, the elderly may require a cane or walker to ambulate safely. Patla144 eloquently expressed the importance of ambulation in our lives: “Nothing epitomizes a level of independence and our perception of a good quality of life more than the ability to travel independently under our own power from one place to another. We celebrate the development of this ability in children and try to nurture and sustain it throughout the lifespan.”
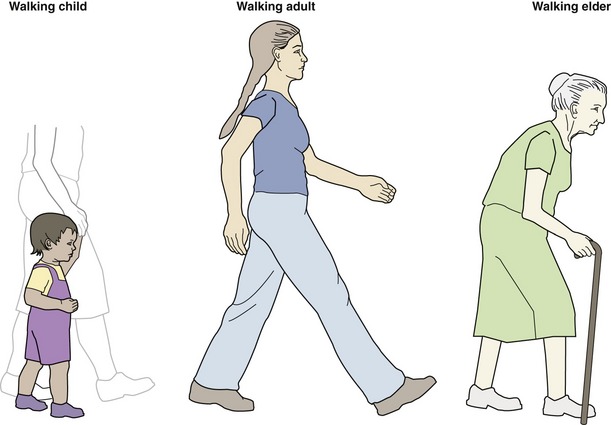
FIGURE 15-1. Walking at various stages in life.
This chapter provides a description of the fundamental kinesiologic characteristics of walking. Unless indicated otherwise, the information provided refers to individuals with a normal and mature gait pattern, walking on level surfaces at a steady average speed. Although this chapter provides enough details to be read independently of the rest of this book, reading Chapters 12 to 14 will facilitate an even greater understanding of walking.
The observation of walking, which is the focus of this chapter, provides information on the outcome of a complex set of “behind the scenes” interactions between sensory and motor functions. For a person to walk, the central nervous system must generate appropriate motor actions from the integration of visual, proprioceptive, and vestibular sensory inputs. Although this chapter covers the intricacy of limb and muscular actions performed during walking, it does not cover the concept of motor control. To gain a greater understanding of the complexity of the motor control of walking, the reader is advised to examine other sources on the topic.*
HISTORICAL PERSPECTIVE OF GAIT ANALYSIS
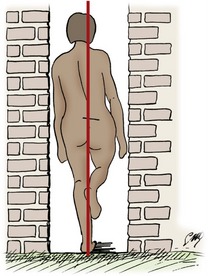
“If a man were to walk on the ground alongside a wall with a reed dipped in ink attached to his head the line traced by the reed would not be straight but zig-zag, because it goes lower when he bends and higher when he stands upright and raises himself.”6 This early written record by Aristotle (384-322 bc) of observation of walking and numerous earlier paintings and sculptures of individuals engaged in the process of walking are testament that both the casual and detailed observation of ambulation has been of interest throughout history.
Despite this earlier interest, it was not until 1836 that the Weber brothers200 published the first notable scientific work on gait, having benefited from the advances in science provided by individuals such as Galileo Galilei (1564-1642), Giovanni Borelli (1608-1679), and Isaac Newton (1642-1727), to name only a few. Willhelm, a physicist and electrician, and Eduard, an anatomist and physiologist, using instruments such as a stopwatch, a tape measure, and a telescope, described and measured elements of walking, such as step length, cadence, foot-to-ground clearance, and vertical excursion of the body. They also defined basic elements of the gait cycle, such as swing phase, stance phase, and double-limb support periods. Many of the terms they introduced remain in use today. The Webers hypothesized that the basic principle of walking is one of least muscular effort—a concept known to be true today, although the exact methods by which the body minimizes energy expenditure are still being studied.137,209,210 An extensive account of the Weber brothers’ work was published in 1894 and translated in 1992.198,199
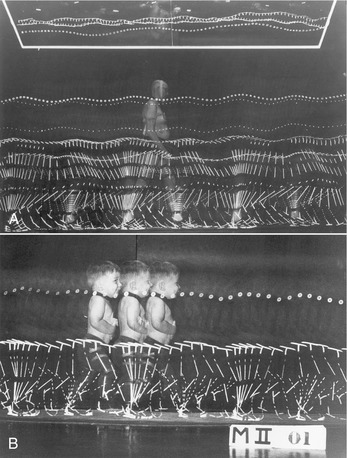
In the nineteenth century, other researchers, such as Marey, Carlet, and Vierordt, made use of ingenious technology to expand our knowledge of gait. Most often cited among Marey and Carlet’s many novel methods of measurement are shoes that had air chambers attached to a recorder to indicate the swing and stance phase of gait (Figure 15-2).112,113,114 Another clever idea, by Vierordt, was the use of ink in small spray nozzles attached to the shoes and limbs.189 The ink sprayed on the floor and wall as the individual walked, providing a permanent record of movement.

Concurrently, advances in the field of cinematography created a powerful medium to study and record the kinematic patterns of humans and animals walking. Muybridge may be the most recognized individual of his time to use cinematography to document sequence of movements. Muybridge is most famous for settling an old controversy regarding a trotting horse. In 1872, using sequence photography, he showed that all four feet of a trotting horse are indeed simultaneously off the ground for very brief periods of time. Muybridge created an impressive collection of photographs on human and animal gait, which was initially published in 1887 and assembled and reproduced in 1979.133,134
Initially, the description of gait was limited to planar analyses; the motion was typically recorded in the sagittal plane and less frequently in the frontal plane. Braune and Fisher15,16 are credited as being the first, from 1895 to 1904, to perform a comprehensive three-dimensional analysis of a walking individual. By using four cameras (two pairs of cameras recording motion for each side of the body) and a number of light tubes attached to various body segments, they documented joint kinematics in three dimensions. They were also the first to use the principles of mechanics to measure dynamic quantities such as segmental acceleration, segmental inertial properties, and intersegmental loads (e.g., joint torques and forces). Their analysis of joint torques, limited to the swing phase of gait, refutes the earlier concept, suggested by Weber and Weber in 1836, that lower extremity motion during the swing phase of gait could be explained solely by a passive pendulum theory.201
Throughout the twentieth century, the understanding of walking was greatly enhanced by many scientific advances. Instrumentation to document kinematics evolved from simple video cameras, with film that required painstaking analysis with a ruler and protractor, to highly sophisticated infrared systems, with real-time coordinate data of limb segments. Notable researchers who contributed to the description of the kinematics of gait using a variety of imaging techniques include Eberhart,49 Murray,125,127 Inman,83 Winter,204 and Perry.147 Noteworthy is the work by Murray, a physical therapist and researcher, who published several papers in the 1960s, 1970s, and 1980s describing the kinematics of many aspects of normal and abnormal gait (Figure 15-3).126–128,130,131,176 Among other accomplishments, data from her research—on the kinematics of walking in individuals with disabilities—influenced the design of artificial joints and lower extremity prosthetic limbs.
Similarly, a more extensive understanding of the kinetics of gait was made possible through the development of devices to measure the forces taking place at the foot-ground interface. Amar,2 Elftman,52 Bresler and Frankel,17 and Cunningham and Brown38 all made significant contributions to this field. With the ability to measure the forces between the foot and the ground came computational methods to calculate the forces and torques taking place at the joints of the lower extremities during the stance phase of ambulation.145,166,206
The development of surface and intramuscular electrodes provided the opportunity to record the electrical activity of muscles during gait.62,181 When this information is integrated with the kinematics of walking, the role that each muscle plays during gait can be better appreciated and more objectively described. Many researchers, including Sutherland,179 Perry,147 Inman,83 and Winter,204 have made notable contributions to the study of electromyography (EMG) during walking.
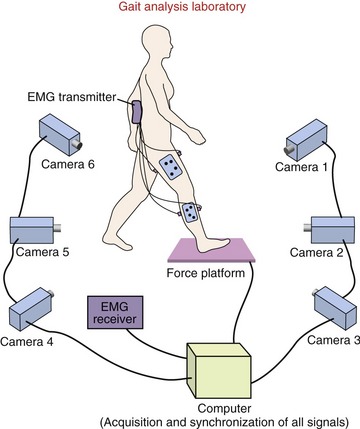
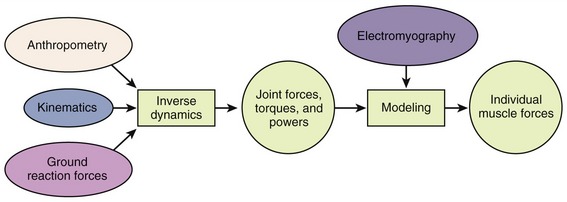
Today, gait analysis is routinely performed in specialized biomechanics laboratories (Figure 15-4). Three-dimensional kinematic data are obtained by using two or more synchronized high-speed cameras. Ground reaction forces are measured using force platforms embedded in the floor. Muscle activity patterns are recorded by multichannel, often telemetered, electromyographic systems. Ultimately, lower extremity joint forces, torques, and powers are calculated with a combination of kinematic data, ground reaction forces, and anthropometric characteristics of the individual (Figure 15-5). These data are then used to describe and study normal and abnormal gait.
Patients with a variety of pathologies can potentially benefit from instrumented gait analyses. Currently the primary beneficiaries of this technology, however, are children with cerebral palsy. In this population, instrumented gait analysis is often used before surgery to help determine the proper intervention. It is employed again after surgery to objectively evaluate the outcome.64 More comprehensive descriptions of the history, tools, and methods used for gait analysis can be found in other sources.7,93,181–183,188,202
Sophisticated technology, such as that described earlier, provides detailed information that can enhance the ability to describe and understand walking. Because such technology is rarely available in the typical clinical setting, clinicians must routinely rely on direct visual observation to evaluate the walking characteristics of their patients.140 Such observational analysis requires a thorough knowledge and understanding of normal gait. Learning about walking, as presented here, is a more dynamic and rewarding experience if the study of this chapter is combined with the observations of gait patterns of relatives, friends, neighbors, and patients in the clinical setting.
SPATIAL AND TEMPORAL DESCRIPTORS
This section describes measurements of distance and time as related to walking.
Gait Cycle
Walking is the result of a cyclic series of movements. As such, it can be conveniently characterized by a detailed description of its most fundamental unit: a gait cycle (Figure 15-6). The gait cycle is initiated as soon as the foot contacts the ground. Because foot contact is normally made with the heel, the 0% point or beginning of the gait cycle is often referred to as heel contact or heel strike. The 100% point or completion of the gait cycle occurs as soon as the same foot once again makes contact with the ground. Initial contact is often used as a substitute term for heel contact when an individual makes first contact with the ground with a part of the foot other than the heel, but for the purpose of this chapter, focusing on normal walking, the term heel contact will be used.
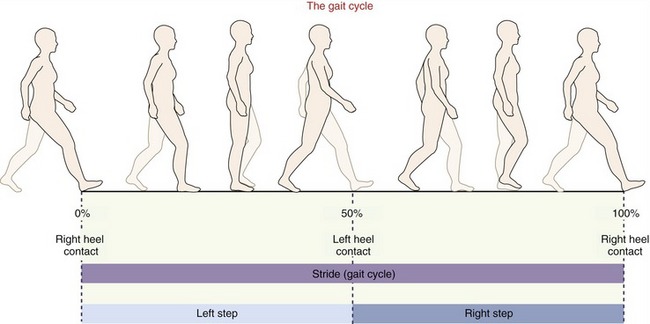
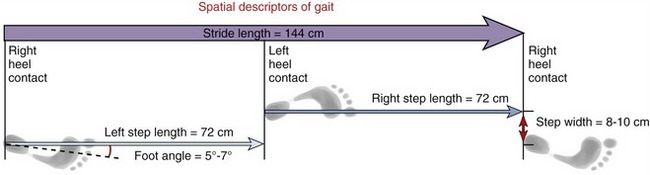
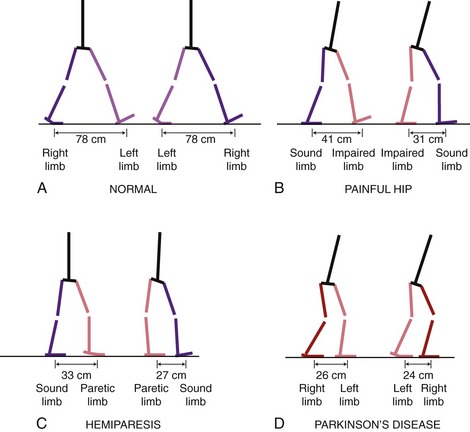
The most basic spatial descriptors of gait include the length of a stride and the length of a step (Figure 15-7). Stride length is the distance between two successive heel contacts of the same foot. Step length, in contrast, is the distance between successive heel contacts of the two different feet. Comparing right with left step lengths can help to evaluate the symmetry of gait between the lower extremities (Figure 15-8). Step width is the lateral distance between the heel centers of two consecutive foot contacts and is on average around 8 to 10 cm (see Figure 15-7).73,111,117,118 Foot angle, the amount of “toe-out,” is the angle between the line of progression of the body and the long axis of the foot. About 5 to 7 degrees is considered average.118 Although the stated norms are for adults, a noteworthy publication80 of data collected from 360 children 7 to 12 years of age documents a normal step width and foot angle of 8 to 10 cm and 2.5 to 6 degrees, respectively—values relatively similar to those in healthy young adults.
Walking speed combines both spatial and temporal measurements by providing information on the distance covered in a given amount of time. The units of measure are typically meters per second (m/sec) or miles per hour (mph). Speed can be calculated by measuring the time it takes to cover a given distance, or the distance covered in a given amount of time, or by multiplying the step rate by the step length. Walking speed varies considerably among individuals based on factors such as age and physical characteristics (e.g., height and weight).36,93 Of all spatial and temporal measurements of gait, speed may be the best and most functional measure of an individual’s walking ability.
For healthy adults, a gait cycle (i.e., two consecutive steps) takes slightly more than 1 second and covers approximately 1.44 m (4.5 feet), resulting in a walking speed of 1.37 m/sec. Data in Table 15-1 indicate that, at a freely chosen walking speed, women exhibit a slower walking speed, shorter step length, and faster cadence than men. These differences are likely in part reflective of anthropometric disparities between genders. Even when anthropometrically matched with men, though, women still demonstrate a higher cadence and shorter step length than men when walking at the same speed.56,129
TABLE 15-1.
Normative Data for Walking Speed, Step Rate, and Step Length
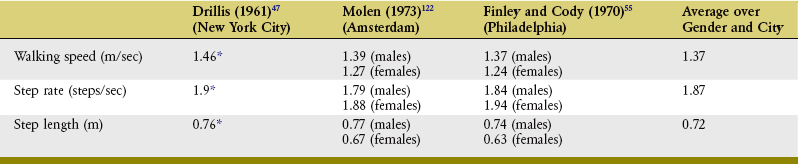
*Males and females are averaged together for these data.
Data obtained from more than 2300 pedestrians unaware of being observed as they walked.
The classic data in Table 15-1 were derived from more than 2300 pedestrians walking outdoors in a large city and who were unaware that their gait characteristics were being measured. Table 15-2 provides data from a select number of studies,* including a smaller number of subjects who walked indoors on an instrumented walkway used to precisely and reliably measure spatial and temporal characteristics of gait. Unlike the pedestrians in the studies in Table 15-1, these subjects were aware that their walking characteristics were being measured, which may account in part for the small differences noted between the data in the two tables.
TABLE 15-2.
Selected Data for Temporal and Spatial Gait Parameters Derived from Individuals Walking in a Laboratory Setting on an Instrumented Walkway*
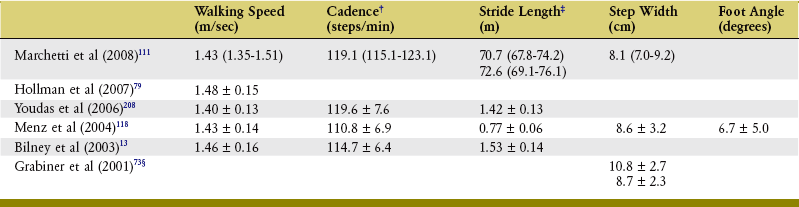
†Divide cadence by 60 to obtain step rate in steps per second.
*Data are means ± standard deviations, with the exception of Marchetti and colleagues, for whom data are means and 95% confidence intervals. All data are for healthy adults, and all groups include both males and females.
‡The data by Marchetti and colleagues are for left and right step length, and the data by Menz and colleagues are for step length.
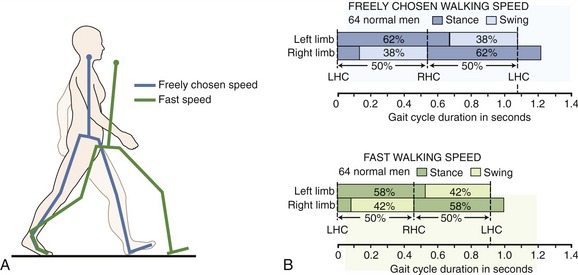
The data in Tables 15-1 and 15-2 were collected from individuals walking at their freely chosen speed, which may not always be fast enough to reach a destination in the desired amount of time. When an increase in walking speed is needed, two strategies are available: increasing the stride, or step length, and increasing the cadence (Figure 15-9). Typically an individual combines both strategies until the longest reasonable step length is reached. From that point on, a further increase in walking speed is solely related to an increase in cadence. It must be reemphasized, therefore, that all values (spatial, temporal, kinematic, and kinetic variables) obtained from the measurements of walking vary based on walking speed. For proper reference and interpretation, reports of gait characteristics should always include the walking speed at which the data were collected.
SPECIAL FOCUS 15-1  Simple Clinical Measurements of Walking
Simple Clinical Measurements of Walking
Sophisticated instrumentation, such as walkways and foot switches, exists to make spatial and temporal measurements of foot placement during gait.* For most clinical applications, this information can, however, be measured with readily available tools and a little imagination. Average walking speed can be measured using a stopwatch and a known distance. Step length and step width can be measured by the use of ink marks made by shoes or feet on a roll of paper covering the floor. This technique works especially well to document abnormal gait patterns, including asymmetry in step length.
Clinically, simple measurements of walking speed and distance can be helpful in monitoring functional progress or documenting functional limitations. Results obtained from a patient can be compared with normal values provided in Tables 15-1 and 15-2 or with minimum standards required to perform a specific task, such as crossing a street within the time allowed by the stoplights.† The following are two proposed minimum standards, based on community-living activities: the ability to walk 300 m (1000 feet) in less than 11.5 minutes (walking speed of 0.45 m/sec or 1 mph); the ability to walk at a speed of 1.3 m/sec (3 mph) for 13 to 27 m (42 to 85 feet) to cross a street safely.
Stance and Swing Phases
To help describe events taking place during the gait cycle, it is customary to subdivide the gait cycle from 0% to 100%. As stated earlier, heel or foot contact with the ground is considered the start of the gait cycle (0%) and the next ground contact made by the same foot is considered the end of the gait cycle (100%). Throughout this chapter, gait is described using the right lower extremity as a reference. A full gait cycle for the right lower extremity can be divided into two major phases: stance and swing (Figure 15-10). Stance phase (from right heel contact to right toe off) occurs as the right foot is on the ground, supporting the body’s weight. Swing phase (from right toe off to the next right heel contact) occurs as the right foot is in the air, being advanced forward for the next contact with the ground. At normal walking speed, the stance phase occupies approximately 60% of the gait cycle, and the swing phase occupies the remaining 40%.
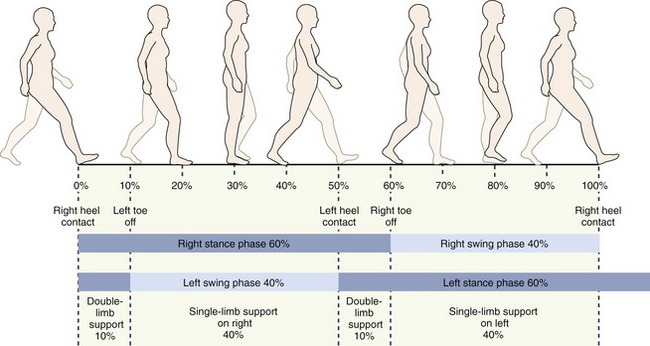
FIGURE 15-10. Subdivision of the gait cycle illustrating the phases of stance and swing and periods of single- and double-limb support.
Within a gait cycle, the body experiences two periods of double-limb support (when both feet are in contact with the ground simultaneously) and two periods of single-limb support (when only one foot is on the ground) (see Figure 15-10). We observe the first period of double-limb support at 0% to 10% of the gait cycle. During that time period, the body’s weight is being transferred from the left to the right lower extremity. The right lower extremity is then in single-limb support until 50% of the gait cycle has been reached. During that time, the left lower extremity is in its swing phase, being advanced forward. The second period of double-limb support takes place at 50% to 60% of the gait cycle and serves the purpose of transferring the weight of the body from the right to the left lower extremity. Finally, at 60% to 100% of the gait cycle the body is again in single-limb support, this time on the left lower extremity. This period of left single-limb support corresponds to the swing phase of the right lower extremity.
As gait speed increases, the percentage of the gait cycle spent in periods of double-limb support becomes shorter (see Figure 15-9). Race walkers aim to walk as fast as possible while always keeping one foot in contact with the ground. For these athletes, greater speeds are achieved by increasing cadence and stride length and by minimizing periods of double-limb support to the point at which stance and swing phase times are about equal. Whereas maximum walking speed in adults 20 to 50 years of age is approximately 2.4 to 2.5 m/sec (5.5 to 5.7 mph),14 walking speed during race walking can be in excess of 3.3 m/sec (7.5 mph).129,169
During running, the periods of double-limb support disappear altogether to be replaced by periods when both feet are off the ground simultaneously. The transition from walking to running normally takes place at a step rate of approximately 180 steps/min or at a speed of approximately 2.1 to 2.2 m/sec (4.8 to 5.0 mph).43,163 Above that speed it is more energy efficient to run than to walk.
Conversely, at a slow walking speed, the periods of double-limb support occupy an increasingly greater percentage of the gait cycle. A slower gait provides greater stability because both feet are on the ground simultaneously for a greater percentage of the cycle. In fact, the reduced speed, shorter step length, and slower cadence commonly seen in the elderly with fear of falling or strength deficits serve to improve gait stability and prevent falls.96
SUBDIVISION OF STANCE AND SWING PHASES
Five specific events are typically described during stance phase: heel contact, foot flat, mid stance, heel off (or heel rise), and toe off (Figure 15-11 and Table 15-3). Heel contact is defined as the instant the heel comes in contact with the ground, at 0% of the gait cycle. Foot flat corresponds to the instant the entire plantar surface of the foot comes in contact with the ground. This event occurs at approximately 8% of the gait cycle. Mid stance is most often defined as the point at which the body’s weight passes directly over the supporting lower extremity. It is also defined as the time when the foot of the lower extremity in the swing phase passes the lower extremity in the stance phase (i.e., the feet are side by side). A third definition of mid stance is the time when the greater trochanter of the femur is vertically above the midpoint of the supporting foot in the sagittal plane. In reality, these three definitions all correspond to about 30% of the gait cycle or 50% of the stance phase. Heel off, the timing of which varies appreciably among individuals, occurs at somewhere between 30% and 40% of the gait cycle. It corresponds to the instant the heel comes off the ground. Toe off, which occurs at 60% of the gait cycle, is defined as the instant the toes come off the ground.
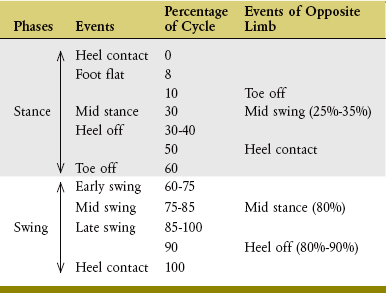
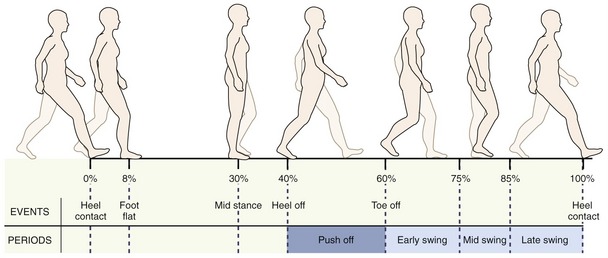
FIGURE 15-11. Traditional subdivisions of the gait cycle.
Although there is a significant amount of variation in the description of the swing phase of gait, this phase is traditionally subdivided into three sections: early, mid, and late swing (see Figure 15-11). Early swing is the period from the time of toe off to mid swing (60% to 75% of the gait cycle). Mid swing corresponds to the time from slightly before to slightly after the mid stance event of the opposite lower extremity, when the foot of the swing limb passes next to the foot of the stance limb (75% to 85% of the gait cycle). Late swing is the period from the end of mid swing to foot contact with the ground (85% to 100% of the gait cycle).
An alternate and relatively more recent terminology, proposed by Perry,147 consists of eight events that divide the gait cycle into seven periods (Figure 15-12). The events are initial contact, opposite toe off, heel rise, opposite initial contact, toe off, feet adjacent, tibia vertical, and initial contact for the next stride. The four time periods during stance are loading response, mid stance, terminal stance, and pre swing. Swing phase has three time periods: initial swing, mid swing, and terminal swing. With a few exceptions, this terminology is in general agreement with the earlier description of gait.
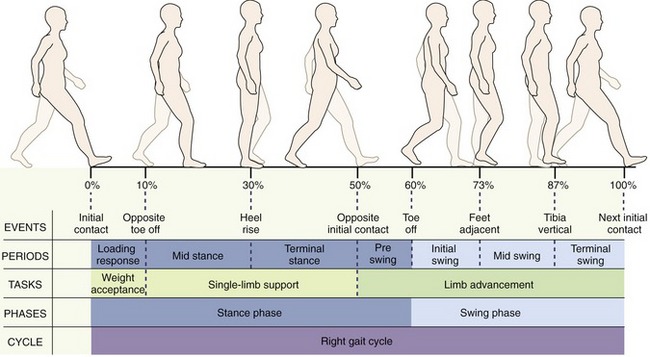
FIGURE 15-12. Terminology to describe the events of the gait cycle. Initial contact corresponds to the beginning of stance when the foot first contacts the ground at 0% of gait cycle. Opposite toe off occurs when the contralateral foot leaves the ground at 10% of gait cycle. Heel rise corresponds to the heel lifting from the ground and occurs at approximately 30% of gait cycle. Opposite initial contact corresponds to the foot contact of the opposite limb, typically at 50% of gait cycle. Toe off occurs when the foot leaves the ground at 60% of gait cycle. Feet adjacent takes place when the foot of the swing limb is next to the foot of the stance limb at 73% of gait cycle. Tibia vertical corresponds to the tibia of the swing limb being oriented in the vertical direction at 87% of gait cycle. The final event is, again, initial contact, which in fact is the start of the next gait cycle.
These eight events divide the gait cycle into seven periods. Loading response, between initial contact and opposite toe off, corresponds to the time when the weight is accepted by the lower extremity initiating contact with the ground. Mid stance is from opposite toe off to heel rise (10% to 30% of gait cycle). Terminal stance begins when the heel rises and ends when the contralateral lower extremity touches the ground, from 30% to 50% of gait cycle. Pre-swing takes place from foot contact of the contralateral limb to toe off of the ipsilateral foot, which is the time corresponding to the second double-limb support of the gait cycle (50% to 60% of gait cycle). Initial swing is from toe off to feet adjacent, when the foot of the swing limb is next to the foot of the stance limb (60% to 73% of gait cycle). Mid swing is from feet adjacent to when the tibia of the swing limb is vertical (73% to 87% of gait cycle). Terminal swing is from a vertical position of the tibia to immediately before heel contact (87% to 100% of gait cycle). The first 10% of the gait cycle corresponds to a task of weight acceptance—when body mass is transferred from one lower extremity to the other. Single-limb support, from 10% to 50% of the gait cycle, serves to support the weight of the body as the opposite limb swings forward. The last 10% of stance phase and the entire swing phase serve to advance the limb forward to a new location.
The existence of two different terminologies can be confusing, especially when many use them interchangeably. In this chapter, the terminology proposed by Perry in 1992 is used predominantly.147 To eliminate confusion, the timing of the events during gait is most often described as a percentage of the gait cycle.
 Take Time to Develop Your Observation Skills
Take Time to Develop Your Observation SkillsDISPLACEMENT AND CONTROL OF THE BODY’S CENTER OF MASS
Displacement of the Center of Mass
The body’s CoM is located just anterior to the second sacral vertebra, but the best visualization of the movement of the CoM is by tracking the displacement of the head or torso. Clearly, the most notable displacement of the body during gait is in the forward direction (Figure 15-13). Superimposed on this forward displacement, however, are two sinusoidal patterns of movement that correspond to the movement of the CoM in the vertical and side-to-side directions.
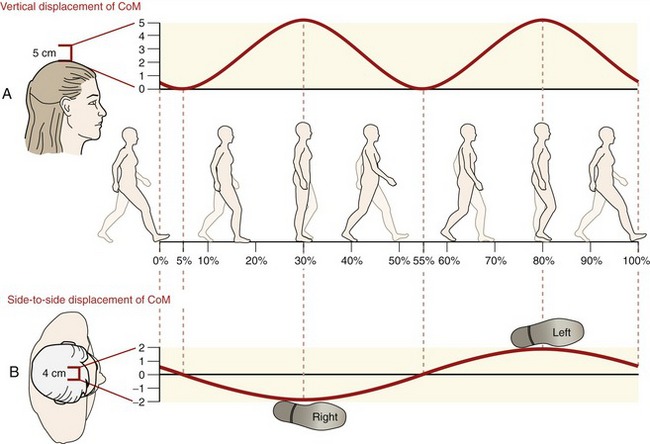
In the vertical direction, the CoM oscillates up and down to describe two full sine waves per gait cycle (see Figure 15-13, A). This movement of the CoM is best understood by looking at the individual from the side. Minimum height of the CoM occurs at the midpoint of both periods of double-limb support (5% and 55% of the gait cycle). Maximum height of the CoM occurs at the midpoint of both periods of single-limb support (30% and 80% of the gait cycle). A total vertical displacement of approximately 5 cm is noted at the average walking speed in the adult male.
During ambulation the CoM is also alternately shifted from the right to the left lower extremity, creating a single side-to-side (right-to-left) sinusoidal pattern per gait cycle (see Figure 15-13, B). Maximum position of the CoM to the right occurs at the midpoint of the stance phase on the right lower extremity (30% of the gait cycle), and maximum position of the CoM to the left occurs at the midpoint of the stance phase on the left lower extremity (80% of the gait cycle). A total side-to-side displacement of approximately 4 cm occurs during normal ambulation.83 The amount of displacement increases when the individual has a wider base of support during gait (i.e., walking with the feet wider apart) and decreases with a narrower base of support (i.e., walking with the feet closer together).
Next consider the total pattern of motion of the CoM during a full gait cycle (see Figure 15-13). Starting shortly after right heel contact, the CoM is moving forward, upward, and toward the right foot. This general direction of movement continues for the first 30% of the gait cycle—the body is essentially “climbing and shifting its mass” over the supporting lower extremity. At right mid stance, the CoM reaches its highest and most lateral position toward the right. Just after right mid stance, the CoM continues forward but starts moving in a downward direction and toward the left side of the body—the body is essentially “falling away” from the supporting lower extremity. This is a critical moment in the gait cycle. With the left limb in its swing phase, the body depends on the left lower extremity to make secure contact with the ground to accept the weight transfer and to prevent a fall. Shortly after left heel contact, during the double-limb support phase, the CoM is located midway between the feet and reaches its lowest position as it continues to move forward and toward the left lower extremity. From right toe off to mid stance on the left lower extremity (80% of the gait cycle), the CoM moves forward, upward, and toward the left lower extremity, which is now providing support. At 80% of the gait cycle, the CoM is again at its highest point, but in its most lateral position to the left. Shortly after left mid stance, the movement of the CoM shifts downward and toward the right side of the body. The gait cycle is completed, and the process repeated, when the right heel contacts the ground.
Noteworthy is the fact that the body’s CoM is never directly located over the body’s base of support during single-limb support (see Figure 15-13, B). This fact illustrates the relative imbalance of the body during gait, especially during single-limb support, when the foot must be positioned just slightly lateral to the vertical projection of the body’s CoM to control its side-to-side movement. Proper location of the foot by hip motion in the frontal plane (i.e., hip abduction and adduction) is crucial considering the limited ability of the muscles of the subtalar joint to control the side-to-side motion of the CoM.203
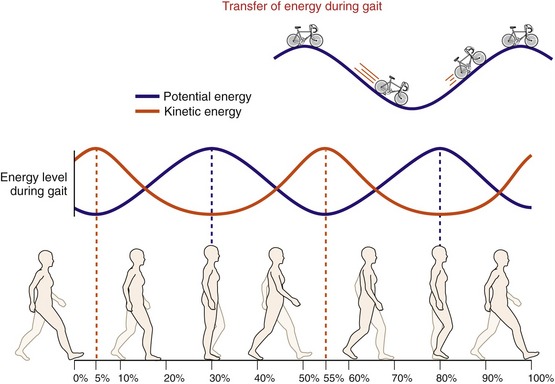
Kinetic and Potential Energy Considerations
Although walking appears to take place at a steady forward speed, the body actually speeds up and slows down slightly with each step. When the supporting lower extremity is in front of the body’s CoM, the body slows down. Conversely, when the supporting lower extremity is behind the body’s CoM, the body speeds up. The body reaches its lowest velocity, therefore, at mid stance, once it has “climbed” on the supporting lower extremity, and its highest velocity during double-limb support, once it has “fallen away” from the supporting lower extremity and before “climbing” on the opposite limb. Because kinetic energy of the body during ambulation is a direct function of its velocity (Equation 15-1), minimum kinetic energy is present at mid stance (30% and 80% of the gait cycle) and maximum kinetic energy is reached at double-limb support (5% and 55% of the gait cycle) (Figure 15-14).

where m is the mass of the body, and v is the velocity of the body’s CoM.
Kinetic energy is complemented by potential energy (see Figure 15-14). Potential energy is a function of the mass of the body, the gravitational field acting on the body, and the height of the body’s CoM (Equation 15-2). During gait, maximum potential energy is achieved when the CoM reaches its highest points (30% and 80% of the gait cycle). Minimum potential energy of the body occurs at double-limb support (5% and 55% of the gait cycle), when the body’s CoM is at its lowest points.

where m is the mass of the body, g is the potential downward acceleration of the body resulting from gravity, and h is the height of the body’s CoM.
In a graphic representation of the changes in kinetic and potential energy during gait, a relationship between the curves is readily observed (see Figure 15-14). The times of maximum potential energy correspond to the times of minimum kinetic energy and vice versa. As potential energy is lost from mid stance to double-limb support (the CoM of the body going from its highest to its lowest location), kinetic energy is gained (the CoM of the body going from its minimum to maximum speed). Conversely, as kinetic energy is lost from double-limb support to mid stance, potential energy is gained. Therefore the body, acting to a great extent as an inverted pendulum, appears to use an optimal magnitude of vertical oscillation to most effectively transfer mechanical energy between its potential and kinetic forms. Deviation from this optimal vertical oscillation, by adoption of either a “bouncy” or a “flat” gait, has been demonstrated to increase energy expenditure.1,115,141
In closing, it must be noted that although the cyclic transfer between kinetic and potential energy minimizes the metabolic cost of walking, this process alone is not sufficient to sustain steady-speed ambulation.19 Consequently, unlike the movement of a perfect pendulum, walking is dependent on the energy generated by muscles. Muscles of the lower extremity must generate forces to assist with forward propulsion of the body during stance phase and help with the advancement of the lower limb during the swing phase.201
JOINT KINEMATICS
Sagittal Plane Kinematics
PELVIS
Movement of the pelvis in the sagittal plane is described as short-arc rotations in anterior and posterior directions about a medial-lateral axis through the hip joints (see Chapter 12). (The direction of the pelvic tilt is based on movement of the iliac crests.) The neutral position (0 degrees of pelvic tilt) is defined as the orientation of the pelvis in relaxed stance. Because the pelvis is a relatively rigid structure, both iliac crests are considered as moving together. During gait at normal speed, the amount of anterior and posterior pelvic tilt is small (i.e., a total of approximately 2 to 4 degrees). Although the movement of the pelvis is described as movement of an independent “detached” structure, the kinematics actually take place primarily at the hip joints (through pelvic-on-femoral flexion and extension) and, to a lesser degree, at the lumbosacral joints (through pelvic-on-lumbar flexion and extension).
The pattern of motion of the pelvis over the full gait cycle resembles a sine wave with two full cycles (Figure 15-15, A). At right heel contact, the pelvis is in a near neutral position. From 0% to 10% of the gait cycle, a period of double-limb support, a small amount of posterior pelvic tilt occurs. The pelvis then begins tilting anteriorly during the period of single-limb support, reaching a slight anterior pelvic tilted position just after mid stance (30% of the gait cycle). In the second half of the stance phase, the pelvis tilts posteriorly until just after toe off. During initial and mid swing (60% to 87% of gait), the pelvis again tilts anteriorly before starting to tilt in the posterior direction in terminal swing.
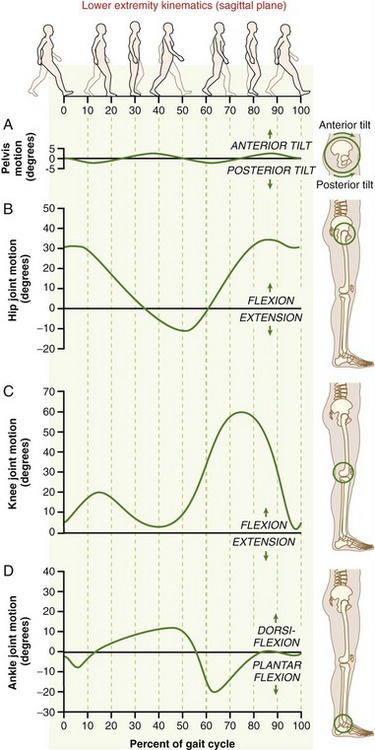
FIGURE 15-15. Sagittal plane angular rotation of the pelvis (A), hip (B), knee (C), and ankle (D) during a gait cycle.
In general, pelvic tilting increases with the speed of ambulation.83 Significant variability in the amount, timing, and direction of tilt, however, has been noted across walking speed and among individuals. The generally noted greater magnitude of pelvic tilt with faster walking speed serves to increase functional limb length, which in turn serves to increase step length.
HIP
At a typical walking speed the hip is flexed approximately 30 degrees at heel contact (see Figure 15-15, B). As the body moves forward over the fixed foot, the hip extends. Maximum hip extension of approximately 10 degrees is achieved before toe off. Flexion of the hip is initiated during pre-swing, and the hip is at about 0 degrees of flexion by toe off (60% of gait). During the swing phase, the hip further flexes to bring the lower extremity forward for the next foot placement. Maximum flexion (slightly more than 30 degrees) is achieved just before heel contact. Note that at heel contact the hip has already started to extend in preparation for weight acceptance. Overall, approximately 30 degrees of flexion and 10 degrees of extension (from the anatomic neutral position) are needed at the hip for normal walking.65,159 As for all of the joints of the lower extremities, the magnitude of hip movement is proportional to walking speed.
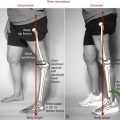
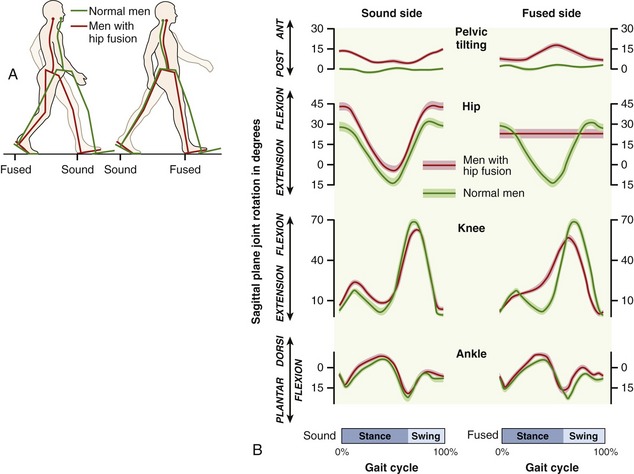
Individuals with limited sagittal plane hip mobility may appear to walk without a gait deviation as the movement of the pelvis and lumbar spine, compensating for reduced hip motion, may be initially unnoticed. Apparent hip extension, detectable with good visual observational skills, can be achieved through an anterior pelvic tilt and associated increase in lumbar lordosis. Conversely, a posterior pelvic tilt accompanied by a flattening of the lumbar spine provides apparent hip flexion. To ambulate, individuals with a fused (i.e., ankylosed) hip use an exaggerated posterior and anterior pelvic tilt as a means to compensate for the absence of sagittal plane hip mobility (Figure 15-16).71,185 Because the pelvis and lumbar spine motions are mechanically linked at the sacroiliac joint, exaggerated pelvic tilting during walking may increase the stress at the lumbar spine. These stresses could eventually irritate the structures within this region, resulting in low back pain.
KNEE
The kinematic pattern of the knee is slightly more complex than that of the hip (see Figure 15-15, C).65,159 At heel contact the knee is flexed approximately 5 degrees, and it continues to flex an additional 10 to 15 degrees during the initial 15% of the gait cycle. This slight knee flexion, controlled by eccentric action of the quadriceps, serves the purpose of shock absorption and weight acceptance as body weight is progressively transferred to this lower extremity. Following initial flexion, the knee approaches near full extension until about heel off (occurring at 30% to 40% of the gait cycle). At this point the knee starts flexing, reaching approximately 35 degrees of flexion by the time of toe off (60% of gait cycle). Maximum knee flexion of approximately 60 degrees is assumed by the beginning of mid swing (73% of gait cycle). Knee flexion during initial swing serves to shorten the length of the lower limb, facilitating toe clearance. In mid and terminal swing, the knee extends to just short of full extension before starting to flex slightly in preparation for heel contact.
ANKLE (TALOCRURAL JOINT)
At the ankle, heel contact occurs with the talocrural joint in a slightly plantar flexed position (between 0 and 5 degrees) (see Figure 15-15, D). Shortly after heel contact (the first 8% of the gait cycle), the foot is positioned flat on the ground by a movement of plantar flexion controlled eccentrically by the ankle dorsiflexors. Then, during stance, up to 10 degrees of ankle dorsiflexion occurs as the tibia moves forward over the foot, which is in firm contact with the ground (from 8% to 45% of the gait cycle). Shortly after heel off (occurring at 30% to 40% of the gait cycle), the ankle begins to plantar flex, reaching a maximum of 15 to 20 degrees of plantar flexion just after toe off. During the swing phase the ankle is again dorsiflexed to a neutral position to allow the toes to clear the ground.65,159
FIRST TARSOMETATARSAL JOINT
The first tarsometatarsal joint, the function of which is described in Chapter 14, has a slight amount of plantar flexion and dorsiflexion that helps adjust the flexibility and stability of the foot’s medial longitudinal arch during gait.8,68
FIRST METATARSOPHALANGEAL JOINT
The metatarsophalangeal (MTP) joint of the hallux (great toe) is crucial to normal gait. At heel contact, the MTP joint is slightly extended. From shortly after heel contact to heel off, the MTP joint is in a relatively neutral position. Between heel off to just before toe off, the MTP joint extends approximately 45 to 55 degrees beyond neutral position. (This is the angle measured between the long axis of the first metatarsal and the proximal phalanx of the hallux.83) During the late part of stance phase and initial swing, the joint flexes and returns to a near neutral position.
SPECIAL FOCUS 15-3  Summary of Sagittal Plane Kinematics
Summary of Sagittal Plane Kinematics
The level of control of the lower extremities during ambulation is remarkable.12,204 During swing, typical toe clearance (the minimum distance between the toes and the floor) is on average between 1.2 and 1.9 cm depending on measurement techniques.10,117,120,123,171 This minimum clearance occurs at mid swing, when the foot has its greatest linear horizontal speed (4.5 m/sec). The transition from the swing to the stance phase is also amazingly well controlled. To provide smooth contact with the ground, vertical heel speed slows just before heel contact to only 0.05 m/sec. This level of control is the basis of the argument against using the term heel “strike” to describe the typically well-controlled heel contact with the ground. Further evidence of the fine control taking place during walking is expressed by the small clearance observed between the edge of steps and the foot during stair descent.167
Frontal Plane Kinematics
PELVIS
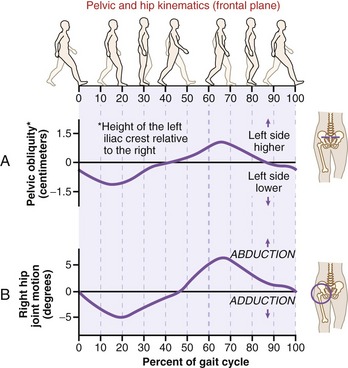
Frontal plane motion of the pelvis during walking is best observed from either in front of or behind the individual, watching the iliac crests rise and fall in relationship to the horizontal plane. The pelvis rotates through a total excursion of about 10 to 15 degrees as a result of pelvic-on-femoral (hip) adduction and abduction on the stance limb. During weight acceptance on the right lower extremity (i.e., the first 15% to 20% of the gait cycle), the left iliac crest drops slightly below the height of the right iliac crest (Figure 15-17, A); this drop of the left iliac crest reflects pelvic-on-femoral adduction of the right stance hip (see Figure 15-17, B).143 This initial downward motion of the left side of the pelvis is the result of gravity acting on the trunk and is controlled to a great extent by eccentric activation of the right hip abductors. From 20% to 60% of the gait cycle, the left iliac crest is elevated by concentric activation of the right hip abductors, assisted by a slight shift of the CoM of the trunk toward the right side. This shift brings the mass of the trunk over the right hip, thereby reducing the external torque demands on the right hip abductors. The elevation of the left iliac crest (on the swing limb) effectively produces abduction of the right stance hip. Throughout the swing phase on the right, a similar pattern occurs of initial controlled lowering of the right iliac crest followed by its progressive elevation.31,161
HIP
The pattern of elevation and depression of the iliac crests reflects the frontal plane motion of the hips (see Figure 15-17, B). During the stance phase this frontal plane motion occurs primarily from pelvic-on-femoral kinematics (see Chapter 12). A much smaller and variable amount of frontal plane motion likely occurs during stance by way of femoral-on-pelvic kinematics. During the swing phase, the motion of the pelvis (about the stance limb) combines with motion of the advancing femur to return the hip to its neutral frontal plane position.31,159
SPECIAL FOCUS 15-4  Possible Causes for Excessive Hip Frontal Plane Motion during Walking
Possible Causes for Excessive Hip Frontal Plane Motion during Walking
The drop of the contralateral iliac crest (i.e., hip adduction) during early to mid stance is normally controlled by an eccentric activation of the hip abductor muscles of the stance limb. Inadequate abduction torque from these muscles often leads to excessive frontal plane motion during stance.138 While standing on one limb, a person with moderate hip abductor weakness demonstrates an excessive drop of the pelvis to the side of the lifted lower extremity (Figure 15-18).21 This action is referred to as a positive Trendelenburg sign. Typically, however, a person with weakened hip abductors, especially if severe, compensates by leaning the trunk to the same side as the weakened muscle during any single-limb support activities, whether standing or walking. During walking, this is called a “compensated” Trendelenburg gait or gluteus medius limp. Leaning of the trunk to the side of weakness minimizes the external torque demands resulting from body weight on the abductor muscles of the stance limb.
KNEE
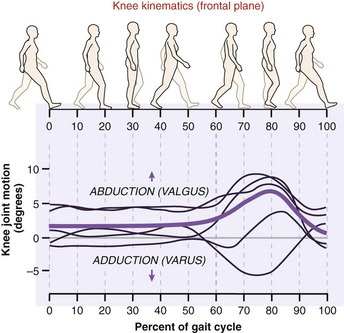
Because of its articular geometry and strong collateral ligaments, the knee is relatively stable in the frontal plane, allowing only a very small amount of angular movement.11,99,159 Benoit and colleagues11 studied the kinematics at the tibiofemoral joints of six healthy subjects by recording the movement of reflective markers attached to the pins inserted in the cortexes of each subject’s femur and tibia. As subjects walked at a self-selected speed, the movements were measured in three-dimensions through the use of four infrared cameras. Overall, the authors found a minimal and inconsistent pattern of abduction-adduction movement (less than 3 degrees) at the knee during the first 80% of stance phase. In the last 20% of stance, just before toe off, approximately 5 degrees of knee adduction took place in most subjects. Benoit and colleagues’ data are generally consistent with those of a previously published study by Lafortune and co-workers who used similar invasive methods on five subjects walking at 1.2 m/sec.99 Lafortune and colleagues reported the knee to be in an average of 1.2 degrees of abduction (valgus) at the time of heel contact (Figure 15-19). This alignment remained unchanged throughout the stance phase.
ANKLE (TALOCRURAL JOINT)
The primary motion of the talocrural joint is dorsiflexion–plantar flexion. Although, as described in Chapter 14, the ankle everts and abducts slightly with dorsiflexion, and inverts and adducts slightly with plantar flexion, these secondary frontal and horizontal plane motions are very small and are not discussed in this chapter.
FOOT AND SUBTALAR JOINT
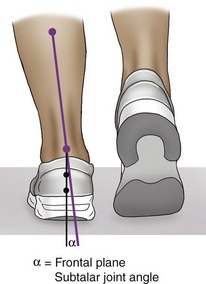
The triplanar motions of pronation and supination occur through interaction of the subtalar and transverse tarsal joints. Pronation combines components of eversion, abduction, and dorsiflexion; supination combines inversion, adduction, and plantar flexion. This chapter considers the frontal plane motions of eversion and inversion at the subtalar joint to represent the more global motions of foot pronation and supination, respectively. Subtalar joint motions are typically measured as the angle made between the posterior aspect of the calcaneus and the posterior aspect of the lower leg (Figure 15-20).
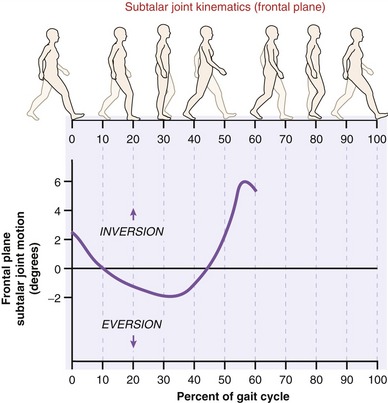
The subtalar joint is inverted approximately 2 to 3 degrees at the time of heel contact (Figure 15-21). Immediately after heel contact, rapid eversion of the calcaneus begins and continues until mid stance (30% to 35% of the gait cycle), where a maximally everted position of approximately 2 degrees is reached. At that time, the subtalar joint reverses its direction of movement and starts toward inversion. Normally, a relatively neutral position of the calcaneus is reached at about 40% to 45% of the gait cycle, at approximately heel off. Between heel off and toe off, calcaneal inversion continues until it reaches a value of approximately 6 degrees of inversion.35 During swing, the calcaneus returns to a slightly inverted position in preparation for the next heel contact. This pattern of motion is generally agreed on in the literature; however, the reported amount of foot pronation during gait varies based on the techniques and preferences for measurement. Reischl and co-workers,150 using a three-dimensional model of the foot, report a mean peak pronation of 10.5 ± 3.4 degrees, occurring at 26.8% ± 8.7% of the gait cycle.
The movement of foot pronation or supination during walking is accompanied by changes in height of the foot’s medial longitudinal arch.8,68 A detailed review of this associated kinesiology is provided in Chapter 14.
 Summary of Frontal Plane Kinematics
Summary of Frontal Plane KinematicsHorizontal Plane Kinematics
Information currently available about lower extremity kinematics in the horizontal plane during walking is provided by only a limited number of studies. To improve the accuracy of these measurements, some investigators fixed rigid metal pins in the pelvis, femur, and tibia of their subjects. Attached to these metal pins were markers that allowed video cameras to track bone movement. In some studies only the movement of the bony structures in space was observed; reports from other studies described the relative motion that took place at the joint itself.82,99
PELVIS
During walking, the pelvis rotates in the horizontal plane around a vertical axis of rotation through the hip joint of the stance limb. The following description of pelvic rotation is based on a top view for a right gait cycle. At right heel contact the right anterior-superior iliac spine (ASIS) is forward compared with the left ASIS. For the initial 15% to 20% of the gait cycle, the pelvis rotates in an internal (counterclockwise) rotation, as viewed from above in Figure 15-22. Throughout the rest of stance on the right lower extremity, an external (clockwise) rotation of the pelvis occurs as the left ASIS progressively moves forward along with the advancing left swing limb. At right toe off, the right ASIS is now behind the left. During swing of the right lower extremity, the right ASIS progressively moves forward. Throughout the gait cycle, the pelvis rotates 3 to 4 degrees in each direction. A greater amount of rotation of the pelvis occurs with increasing walking speed to increase step length.
FEMUR
After heel contact, the femur rotates internally for the first 15% to 20% of the gait cycle (see Figure 15-22). At about 20% of the gait cycle, the femur reverses its direction and rotates externally until shortly after toe off. Internal rotation of the femur takes place throughout most of the swing phase. Overall, the femur rotates approximately 6 to 7 degrees in each direction during gait.25
TIBIA
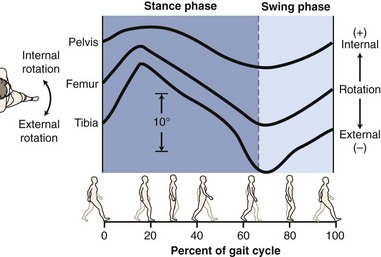
The pattern of movement of the tibia is very similar to the movement described for the femur (see Figure 15-22). The magnitude of the rotation is about 8 to 9 degrees in each direction.
HIP
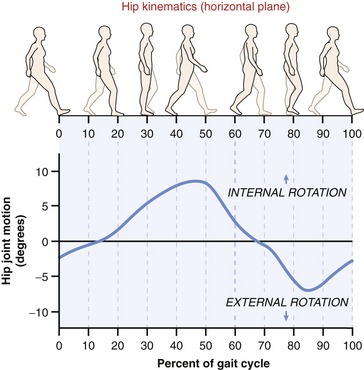
Both the femur and the pelvis rotate simultaneously. At right heel contact, the right hip is in slight external rotation based on the relative posterior position of the contralateral (left) ASIS (Figure 15-23). A net internal rotation movement of the right hip occurs during most of stance on the right lower extremity, as the contralateral (left) ASIS is brought forward. A maximum internally rotated position is achieved by 50% of gait. External rotation of the right hip occurs from 50% of gait until mid swing, as the right lower extremity is advanced forward. From mid swing to right heel contact, a slight amount of right hip internal rotation takes place.31,159,179
KNEE
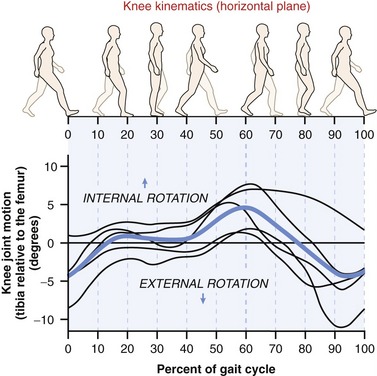
There are two studies of particular interest that used intracortical pins attached to the femur and tibia as a means to precisely document horizontal plane rotation of the knee during ambulation.11,99 Figure 15-24 illustrates data from a study by Lafortune and colleagues for each subject, along with the group average.99 Clearly, and consistent with data from Benoit and co-workers,11 the amount and direction of the horizontal plane rotation of the knee is highly variable. Much of this variability is masked by the process of averaging the data across individuals, as performed in Figure 15-24 and in many descriptive and research reports. In fact, although Figure 15-24 shows an overall trend toward internal rotation during the stance phase, data by Benoit and colleagues11 indicate an average overall pattern of knee external rotation. This variability makes it difficult to interpret many of the studies that have proposed a biomechanical link between knee pain and abnormal horizontal plane kinematics at this joint during walking and running.
ANKLE AND FOOT
SPECIAL FOCUS 15-6  Summary of Horizontal Plane Kinematics
Summary of Horizontal Plane Kinematics
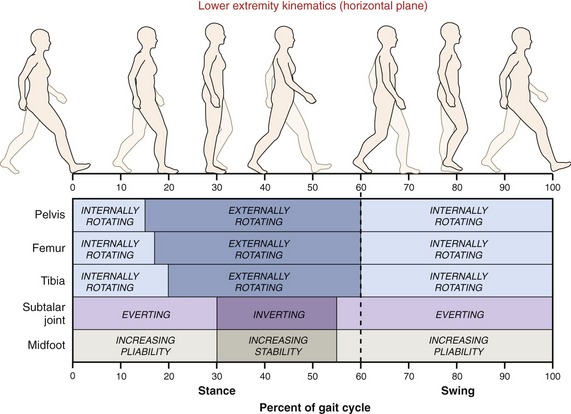
Figure 15-25 summarizes the direction of horizontal plane rotation of the major bones of the lower extremity and subtalar joint during walking, using different sets of data.35,71,110 The pelvis, femur, and tibia rotate internally, well after heel contact (i.e., through about 15% to 20% of the gait cycle). This mass internal rotation is accompanied by subtalar joint eversion. As described in Chapter 14, an everting subtalar joint tends to increase the pliability of the midfoot region, including the transverse tarsal joint. A pliable midfoot serves to cushion the impact of limb loading. After about 15% to 20% of the gait cycle, the pelvis, femur, and tibia all begin to externally rotate until toe off. Simultaneously to this external rotation of the pelvis, femur, and tibia the subtalar joint begins moving toward inversion, which tends to increase the stability of the midfoot region. This stability enables the midfoot to serve as a rigid lever in terminal stance and pre-swing, allowing the plantar flexors to lift the calcaneus without the midfoot collapsing under the body’s weight. Further investigation, such as that performed by Reischl and colleagues,150 is needed to clearly elucidate the exact relationship that exists between the timing and magnitude of pronation of the foot and rotation of the tibia and femur.
Trunk and Upper Extremity Kinematics
The trunk and upper extremities play an important role in maintaining balance and minimizing energy expenditure during gait. In addition, small intricate spinal movements and muscular actions at the trunk serve to dampen the gait-related oscillations and accelerations produced by the movement of the lower extremities.86,119 As a result, accelerations of the head segment are 10% to 40% less than those of the lower portion of the trunk. This dampening effect, keeping the head more stable, serves an important role in optimizing visual and vestibular function during gait.
TRUNK
During ambulation, translation of the CoM follows the general pattern of translation of the head and trunk (see Figure 15-13). In addition, the trunk rotates in the horizontal plane around its vertical axis. The shoulder girdle rotates in the opposite direction as the pelvis. The average total rotational excursion of the shoulder girdle is approximately 7 to 9 degrees.18,132 This pattern of movement of the trunk makes a small contribution to the overall efficiency of gait.18 Restriction of trunk motion increases energy expenditure during walking by as much as 10%.149
Although the preceding paragraph briefly describes the horizontal plane motion of the trunk, Rozumalski and colleagues155 in 2008 published data on segmental motion throughout the lumbar spine during ambulation. The uniqueness of this study is related to the methods of data collection, which included three-dimensional video analysis of markers rigidly fixed to the spinous processes of all lumbar segments using surgically inserted Kirshner wires. The data indicate complex intervertebral lumbar motion of up to 3 to 5 degrees in each direction, in all three planes.155 These kinematics, although modest, are likely necessary to allow the previously described small triplanar pelvic motions to occur while the trunk is kept in a relatively erect posture.
SHOULDER
In the sagittal plane the shoulder exhibits a sinusoidal pattern of movement that is out of phase with hip flexion and extension. As the hip (femur) moves toward extension, the ipsilateral shoulder (humerus) moves toward flexion, and vice versa.174 At heel contact, the shoulder is in its maximally extended position of approximately 25 degrees beyond the neutral position. The shoulder then progressively rotates forward to reach a maximum of 10 degrees of flexion by 50% of the gait cycle. In the second half of the gait cycle, as the ipsilateral hip moves forward toward flexion, the shoulder extends to return to 25 degrees of extension by the next heel contact.
The pattern of movement of the shoulder is consistent across individuals, although the magnitude of movement varies greatly. In general, the amplitude of shoulder movement increases with greater speed. Arm swing is partly active, rather than fully passive, especially for the movement of shoulder extension that requires some activation of the posterior deltoid muscle.197 The major function of arm swing is to balance the rotational forces in the trunk.51 Restriction of arm motion has not been shown to have a significant effect on the energy cost of ambulation.149,207
ELBOW
The elbow is normally in approximately 20 degrees of flexion at heel contact. As the shoulder flexes in the first 50% of the gait cycle, the elbow also flexes to a maximum of approximately 45 degrees. In the second half of the gait cycle, as the shoulder extends, the elbow extends to return to 20 degrees of flexion.132
ENERGY EXPENDITURE
Energy expenditure during gait is measured by the amount of energy used in calories per meter walked per kilogram of body weight. Typically, energy expenditure is measured indirectly by quantifying oxygen consumption.154 When walking, the body strives to minimize energy cost. Conservation of energy is achieved by optimizing the excursion of the CoM, controlling the body momentum, and taking advantage of intersegmental transfers of energy.201
The metabolic efficiency of walking is greatest at a walking speed of approximately 1.33 m/sec (3 mph).154 Not surprisingly, this walking speed roughly corresponds to that freely adopted by individuals ambulating on the street (see Table 15-1). Walking faster or slower than that optimal speed increases the energy cost of ambulation (Figure 15-26).
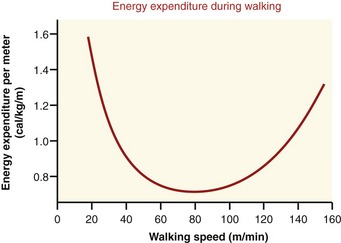
Walking speed is equal to the product of step length and cadence (step rate). Maximum energy efficiency of walking is achieved by the body’s innate ability to adopt an ideal combination of step length and step rate. This combination is demonstrated across all walking speeds. Although the energy cost of ambulation increases with walking speed, the efficiency of walking is greatest at the maintained step length–step rate ratio of 0.0072 m/steps/min for men and 0.0064 m/steps/min for women across all walking speeds.211 At any given walking speed, imposition of a different step length or step rate increases energy expenditure.
With abnormal gait the energy cost of ambulation increases (Table 15-4).39,135 As a consequence, individuals with abnormal gait patterns tend to walk more slowly as a means to keep the rate of energy consumption at a comfortable aerobic level. Further discussion of the energetics of walking in individuals with pathologic gaits can be found in Perry’s textbook147 and reviews of the literature by Gonzalez and Corcoran69 and Waters and Mulroy.196
TABLE 15-4.
Increased Energy Cost of Walking Associated with Specific Conditions
| Conditions | Increased Energy Cost (%)* |
| Immobilization of one ankle149,192 | 3-6 |
| Immobilization of one knee in full extension92,193 | 23-33 |
| Immobilization of one knee at 45 degrees of flexion149 | 37 |
| Immobilization of one hip, arthrodesis192 | 32 |
| Unilateral transtibial amputation, walking with prosthesis60 | 20-38 |
| Unilateral transfemoral amputation, walking with prosthesis60 | 20-60 |
| Postcerebrovascular accident, moderate-to-severe residual deficits34 | 55 |
Energy-Saving Strategies of Walking
During gait, five kinematic strategies serve to reduce the displacement of the CoM which, in turn, has long been believed to decrease energy cost. Vertical displacement of the CoM is reduced by the combined actions of the first four strategies. The fifth strategy serves to reduce the side-to-side displacement of the CoM (Table 15-5). The strategies detailed in this chapter are based on the six determinants of gait originally described by Saunders and colleagues in 1953.158 A detailed account of these determinants is found in the work of Inman and colleagues.82,83
TABLE 15-5.
Kinematic Strategies to Optimize Energy Expenditure during Gait
| Direction of Action | Name of Strategy | Action |
| Vertical | Horizontal plane pelvic rotation | Reduces the downward displacement of the center of mass (CoM) |
| Vertical | Sagittal plane ankle rotation | Reduces the downward displacement of the CoM |
| Vertical | Stance phase knee flexion | Reduces the upward displacement of the CoM |
| Vertical | Frontal plane pelvic rotation | Reduces the upward displacement of the CoM |
| Side to side | Frontal plane hip rotation (step width) | Reduces the side-to-side excursion of the CoM |
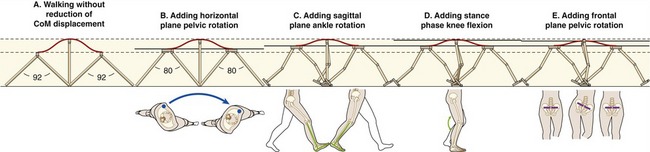
To appreciate the effects of the four kinematic strategies used to optimize the vertical displacement of the CoM, envision gait without such mechanisms. This can be achieved by using two pencils connected at the eraser ends (Figure 15-27, A). During walking, a large vertical oscillation of the eraser end of the pencils (representing the pelvis and therefore the body’s CoM) is readily observed. The eraser end is highest when the pencils are side by side in a vertically oriented position (i.e., mid stance). Conversely, the eraser end is lowest when the pencils are maximally angled (i.e., double-limb support). This gait pattern results in a large displacement of the CoM.
Saunders and colleagues158 in their classic manuscript, suggested that the goal of these strategies is to reduce the displacement of the CoM so as to decrease the energy expenditure related to the muscular effort needed to cyclically lift the body. This view has since been challenged in favor of a model in which the vertical displacement of the body acts more like an inverted pendulum, taking advantage of the transfer between potential and kinetic energy.97 More recent data actually suggest that an optimal amount of vertical oscillation of the CoM exists, one that is neither too “flat” or too “bouncy,” which minimizes energy cost.1,70,97,115,141 These data provide a new perspective on the interpretation of the goal of the original determinants of gait, possibly from “minimizing” to “optimizing” the CoM displacement. Additional work is needed to better understand the relationship among lower extremity kinematics, CoM excursion, and energy cost of ambulation.
VERTICAL DISPLACEMENT OF THE CENTER OF MASS
Reducing the downward displacement of the CoM is achieved by horizontal plane pelvic rotation and sagittal plane ankle rotation. Horizontal plane rotation of the pelvis advances the entire swing limb forward, thereby minimizing the amount of hip flexion and extension needed for a given step length (compare Figure 15-27, A with Figure 15-27, B). As a consequence of the lower extremities remaining closer to a vertical orientation throughout the gait cycle, the lowest points of the CoM trajectory are raised, which reduces the downward displacement of the CoM. Sagittal plane ankle rotation makes use of the configuration of the ankle-foot complex (Figure 15-27, C). At heel contact the alignment of the ankle places the large protruding calcaneus in contact with the ground, functionally elongating the lower extremity. Near the end of stance, as the hip extends and the knee begins to flex, the lower extremity is elongated by plantar flexion of the ankle (i.e., heel rise). This functional elongation of the lower extremity at both ends of stance phase further reduces the downward displacement of the CoM (compare Figure 15-27, B with Figure 15-27, C).41,90,91
Limiting the upward displacement of the CoM is partially achieved by stance phase knee flexion, when the lower extremity is in its most vertical orientation (see Figure 15-27, D). Frontal plane pelvic rotation further assists in reducing upward displacement of the CoM (see Figure 15-27, E). During stance phase, the contralateral iliac crest falls as the ipsilateral iliac crest rises. Throughout a complete gait cycle, therefore, the iliac crests alternately rise and fall like the ends of a seesaw, but the point just anterior to the second sacral vertebra (i.e., the point representing the body’s CoM) remains relatively stationary, as would the pivot point of a seesaw.41,91
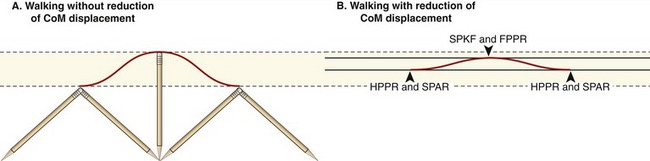
As shown in Figure 15-28, the combination of the four aforementioned strategies reduces the total net vertical displacement of the CoM. The downward displacement of the CoM is reduced by horizontal plane pelvic rotation and sagittal plane ankle rotation. The upward displacement of the CoM is reduced by stance phase knee flexion and frontal plane pelvic rotation. Although still debated, the work by Della Croce and colleagues41 suggests that sagittal plane ankle rotation has the largest influence on CoM vertical displacement, followed by pelvic obliquity, stance phase knee flexion, and frontal plane pelvic rotation.
SIDE-TO-SIDE DISPLACEMENT OF THE CENTER OF MASS
While a person walks, his or her CoM shifts side-to-side and remains within the dynamic base of support provided by the feet (see Figure 15-13). The amplitude of this lateral displacement, partially reflected by step width, is largely a function of frontal plane hip motion (i.e., hip abduction and adduction). The normally adopted 8- to 10-cm step width during ambulation reduces side-to-side displacement of the body, primarily as a strategy to reduce energy expenditure.46,135 Because, however, this step width also decreases the potential size of the dynamic base of support, it likely represents a mechanical compromise between energy conservation and stability of the body as a whole. Theoretically a step width greater than 8 to 10 cm provides greater stability at a cost of increased energy expenditure. Persons with balance disorders, for example, often choose to walk with a wider base of support as a means to improve their stability. Although this strategy increases the energy cost of walking, the tradeoff is likely worthwhile, considering the often negative consequences of falling.
But, as discussed earlier with regard to vertical displacement of the CoM, the normally adopted step width of 8 to 10 cm seems to reflect the inherent ability of the body to naturally use kinematic strategies that are optimal to minimize energy expenditure. It has been demonstrated that ambulation with either a lesser or a larger step width increases energy cost of ambulation in young healthy individuals.46