[level-membership-for-orthopaedics-category]
CHAPTER 40 Kinematics of the Lunotriquetral Joint
Lunotriquetral injury is less frequently seen with distal radius fracture than one of the triangular fibrocartilage complex (TFCC) or scapholunate ligament injuries. One of the problems with lunotriquetral disorders is that most patients have normal imaging studies and fall under the broad and often vexing category of patients with ulnar-sided wrist pain. However, these disorders can have devastating effects on carpal mechanics and, unless properly treated, disruptions of the lunotriquetral supporting ligaments may result in substantial instability of the carpus. Knowledge of these effects and potential consequences will aid the treating physician in offering the patient the best possible outcome.
Functional Anatomy
Joint Anatomy
The relevant midcarpal articulation is between the distal articular surfaces of the lunate and triquetrum and the proximal surfaces of the capitate and hamate. A sagittal ridge can divide the lunate articular surface into a radial and ulnar fossa, and in these cases the proximal surface of the hamate articulates with the lunate. The incidence of this type II lunate varies considerably and is reported in 27% to 63% of adults.1,2 Otherwise, the distal surface of the lunate is concave in both coronal and sagittal planes.
The hamate-triquetral articulation has a helicoid or screw-shaped configuration. The plane of the joint is not parallel to the articular surface of the distal hamate with the fourth and fifth metacarpals but is situated at a substantial angle (reported as high as 90 degrees3).
Ligament Anatomy
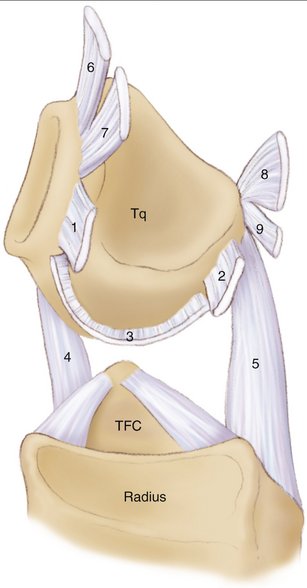
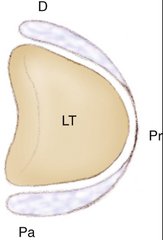
The lunotriquetral joint is stabilized by an intricate arrangement of ligaments (Fig. 40-1). The intrinsic (both origin and insertion are within the carpus) lunotriquetral ligament is “C” shaped and is actually composed of three discrete regions: true ligaments dorsally and palmarly with collinear fascicles of collagen and a proximal region composed of fibrocartilage (Fig. 40-2). This proximal region has a wedge-shaped cross-sectional geometry and is reminiscent of a meniscus. In normal subjects there should be no communication between the midcarpal and radiocarpal joints but the proximal region of the lunotriquetral joint can be perforated by age. Because the proximal membrane contributes very little to the overall lunotriquetral stability, a defect at this level is not a sign of instability but can be a normal physiological, albeit age-related, finding, caused by wear. Mikic4 found up to 55% of lunotriquetral perforations past the third decade.
Radioulnocarpal Ligaments
Most extrinsic ligaments across the radioulnocarpal joint are obliquely oriented relative to the longitudinal axis of the forearm. Based on this, they may be subdivided into two groups: ligaments that prevent excessive passive supination of the proximal row relative to the forearm (anti-supination ligaments) and ligaments that control passive pronation (anti-pronation ligaments).5,6
Three ligaments act synergistically to prevent the proximal row to passively supinate beyond normal. The first is the palmar ulnotriquetral ligament that originates at the fovea near the base of the ulnar styloid. In approximately 90% of normal adults, the ulnotriquetral ligament is split distally to form an orifice that connects the radiocarpal and pisotriquetral joints.7 Second is the ulnolunate ligament that arises from the palmar edge of the triangular fibrocartilage (TFC) and runs obliquely toward its distal insertion into the anterior aspect of the lunate. Palmar to the ulnolunate and ulnotriquetral ligaments is the ulnocapitate ligament, which reinforces both these ligaments before passing anterior to the lunotriquetral joint, where it interdigitates with the fibers of the palmar region of the lunotriquetral interosseous ligament. It arises from the ulna at the fovea where the dorsal and palmar radioulnar ligaments also attach. Third, the dorsal radiotriquetral ligament is a wide, fan-shaped ligament that connects the dorsal edge of the distal radius to the dorsal rim of the triquetrum.8–12
Midcarpal Ligaments
The ulnar limb of the arcuate ligament, also known as the palmar triquetrum/hamate/capitate ligamentous complex, strongly connects the triquetrum to the distal carpal row.10,13–16 It consists of a group of fan-shaped fascicles formed by dense collagen fibers that links the distal anterior edge of the triquetrum to the palmar aspects of the hamate and capitate. This ligament can be regarded as an anti-supination ligament. The only dorsal midpalmar crossing ligament is the dorsal intercarpal ligament. It arises from the dorsal ridge of the triquetrum, courses transversely along the distal edge of the lunate, and fans out to insert on the dorsal rim of the scaphoid, the trapezium, and the trapezoid bones.8,10,17 This ligament can be characterized as an anti-pronation ligament.
There is no dorsal or ulnar ligament between the triquetrum and hamate. Because the midcarpal joint is not a true hinge articulation, there are no vertically oriented ligaments. Their absence is functionally substituted by the extensor carpi ulnaris tendon, which is a thick sheath that may act as a dynamic joint stabilizer.18
Mechanics
Material and Constraint Properties
Results of material property testing of the lunotriquetral ligament showed that the palmar region of the ligament is not only thicker but indeed stronger than the dorsal portion of the ligament (average yield strengths: 301 N and 121 N, respectively).19 The palmar region was found to constrain primarily translation, whereas the dorsal region provides the majority of rotational constraint. The fibrocartilaginous proximal region failed at 64 N and was the least important constraint in all directions. The morphology and material and constraint properties of the lunotriquetral ligament are the exact opposite as found in the scapholunate ligament.20 In a way, the lunate could be thought of as a “torque-suspended” bone between the scaphoid and the triquetrum, much in the manner of a spring. This “torque suspension” concept, for which there is now sufficient evidence, is of importance for the discussion and understanding of dorsiflexed intercalated segment instability (DISI) and volar-flexed intercalated segment instability (VISI).
Recently, immunohistochemical analysis of wrist ligament innervation showed that sensory important ligaments were primarily related to the triquetrum while mechanically important ligaments were primarily located in the radial, force-bearing column of the wrist. The triquetrum and its ligamentous attachments are regarded as key elements in the generation of the proprioceptive information necessary for adequate neuromuscular wrist stabilization.21
Kinematics
All the above mechanisms make it necessary for the proximal carpal bones to take very specific positions, with small pronation/supination motions and mainly ulnar deviation as conjunct motion to flexion/extension of the wrist. In 60 degrees and 30 degrees of wrist extension, the lunate extended 29.7 degrees and 15.4 degrees and the triquetrum 39.3 degrees and 20.1 degrees, respectively. With 60 degrees and 30 degrees of flexion, the lunate flexed 23.0 degrees and 11.5 degrees and the triquetrum 30.6 degrees and 15.5 degrees, respectively, with simultaneous ulnar deviation of both lunate and triquetrum. In extension/flexion motion of the wrist there is some progressive pronation of the triquetrum. Thus, the total arc of lunotriquetral intercarpal motion in the sagittal plane was 16.8 degrees, with the wrist moving from 60 degrees of extension to 60 degrees of flexion. With radial and ulnar deviation of the wrist, the magnitude of the conjunct motion of both the lunate and triquetrum is greater than the primary motion: that is, flexion/extension motion of these carpals is greater than the prime radioulnar deviation motion.22
These results are all in broad agreement with previous in vitro studies23–25 concerning normal carpal kinematics as well as with more recent in vivo studies.26,27
Most recently it has been demonstrated that the kinematics of a type I lunate are different from those of a type II lunate during radioulnar deviation of the wrist: wrists with a type I lunate show statistically greater scaphoid translation with radial deviation, whereas wrists with a type II lunate show statistically greater scaphoid flexion with radial deviation.28,29
It is obvious that the intercalated lunate is in need of constraints on both sides to counteract the just-mentioned torques. Although the connections between triquetrum and lunate are strong, they are not so taut as not to allow mutual mobility. In fact, during maximal radioulnar deviation there is an average 2.5-mm proximal shift of the triquetrum relative to the lunate, ranging from 0 to 5.2 mm.30 Thus, from a kinematic viewpoint, the lunotriquetral joint is not a functional block without intrinsic mobility.
Mechanisms of Injury
Trauma
Frequently encountered associated regional injuries are a combination of a partial or complete rupture of the lunotriquetral ligaments, a peripheral tear of the TFCC, and a distal avulsion of the ulnotriquetral ligament. The mechanism of injury may be similar to the just discussed mechanism for the isolated lunotriquetral injury except for the presence of radial deviation and pronation as the predominant torque-inducing vectors. It is reported that this combination of injuries is not unusual, and it is easy to miss any one of its components.31 Avulsion fracture of the palmar rim of the triquetrum as documented by Smith and Murray32 should be interpreted as a subtle sign of a more extended lunotriquetral injury and would correlate well with the previously described concept of a “reversed Mayfield perilunate dislocation model” discussed by Viegas and coworkers.33
In other circumstances the progression of injury seems to follow a more direct perilunate destabilization process, as described in the well-known paper by Mayfield.34 This classic pattern of progressive perilunate instability begins with palmar to dorsal disruption of the scapholunate interosseous ligament. In these instances, injury to the lunotriquetral ligaments occurs in stage III, after rupture of the scapholunate ligaments (stage I) and the lunocapitate dislocation (stage II). Lunotriquetral dissociation is an integral part of a progressive perilunate dislocation, but it is difficult to imagine as an isolated finding according to this classic progression pattern. Perhaps isolated lunotriquetral instability represents a residual problem from a previous perilunate injury in which the scapholunate problem heals spontaneously or with intervention.
Acute lunotriquetral ligament injury is less frequently seen with distal radius fracture than one of the TFCC or scapholunate ligament injuries. Still, partial or complete lunotriquetral ligament disruption is reported to be associated with intra-articular fractures in a considerable number of cases, ranging from 7% to 24%.35–37 Because additional disruption of the palmar arcuate ligament and/or the dorsal radiocarpal ligaments is necessary to produce a VISI stance, this pattern is seldom seen acutely in distal radius fractures.
Degeneration
A lunotriquetral instability pattern may also appear as the consequence of an ulnocarpal abutment resulting in degeneration of (mainly) the proximal portion of the lunotriquetral ligament by a wear mechanism. Patients without history of trauma, inflammatory arthritis, or ulnocarpal abutment also may have degenerative lunotriquetral lesions because this region is prone to age-related degeneration.4 In both situations the lunotriquetral joint is not dissociated and no progressive derotational changes will develop.
Injury to the Lunotriquetral Supporting Ligaments: Effects on Carpal Kinematics*
In the laboratory, several attempts to ascertain the consequences of lunotriquetral ligament disruptions have been made.14,15,25,38 The first published investigation of the role of the lunotriquetral ligaments in the carpal kinematics was reported by Reagan and associates,39 who also were the first to analyze a series of such ligament injuries. They showed that in patients with severe lunotriquetral sprains there was often a static VISI deformity and abnormal motion of the carpus. That clinical study also showed that on lateral radiographs the longitudinal axis of the triquetrum, which in normal subjects exhibits an average 16 degrees of flexion relative to the longitudinal axis of the lunate, shows an extension posture of more than 14 degrees in severe lunotriquetral disruption: this is a more than 30-degree change in the lunotriquetral angle compared with normal. Reagan and associates39 also described an increased proximal migration of the triquetrum on ulnar-deviated posteroanterior radiographs.
In 1990, Viegas and coworkers33 showed that even in partial disruptions of the lunotriquetral ligament there is increased motion between the elements of the lunotriquetral joint, a finding later confirmed by Horii and colleagues25 using biplanar radiography. All intercarpal joints have altered kinematics after complete lunotriquetral ligament sectioning. The changes were especially marked at the lunotriquetral joint, with the lunate adopting a palmar-flexed position and the triquetrum rotating into supination. Li and associates40 concluded that the palmar lunotriquetral ligament is the major stabilizer of the lunotriquetral joint during wrist extension and that the rest of the lunotriquetral ligament provides stability during ulnar deviation.
Horii and colleagues25 and Viegas and coworkers33 emphasized the importance of the dorsal radiotriquetral and scaphotriquetral ligaments in the prevention of a global carpal collapse when the lunotriquetral ligaments are disrupted. In most studies, a carpal collapse, typically in the form of a VISI pattern, occurred only when the ligaments were sectioned in association with complete lunotriquetral ligament division. Li and associates40 did not observe a static or dynamic VISI deformity after sectioning only the lunotriquetral ligaments.
More recently, Ritt and colleagues,38 from the Mayo Clinic, reported on a series of cadaver specimen using stereoradiographic techniques to study carpal kinematics after different sequences of lunotriquetral ligament sectioning. According to that investigation, neither the isolated section of the proximal lunotriquetral membrane nor the disruption of both proximal and dorsal regions of the lunotriquetral capsule creates any significant change in carpal alignment (stage II in Table 40-1) or carpal motion. From a kinematic viewpoint, partial tears of the proximal lunotriquetral membrane need not be treated because they have minimal mechanical consequences. In contrast, when the palmar lunotriquetral ligament is sectioned selectively, significant changes in carpal kinematics occur. Although the intrinsic tendency of the scapholunate complex to rotate into flexion is still balanced (no carpal malalignment yet at this stage), increased lunotriquetral instability becomes evident, especially in ulnar deviation. Only after dividing the dorsal radiotriquetral and scaphotriquetral ligaments does carpal malalignment occur in a consistent fashion: lunate and triquetrum supinate, flex, and radially deviate (stage IV in Table 40-1). The strong dorsal radiotriquetral and scaphotriquetral ligaments can act as rotational constraints for the lunotriquetral joint in the absence of the dorsal lunotriquetral ligament.
TABLE 40-1 Carpal Alignment (Degrees) Relative to the Radius (Changes from Intact Stage) at Neutral Wrist Position*
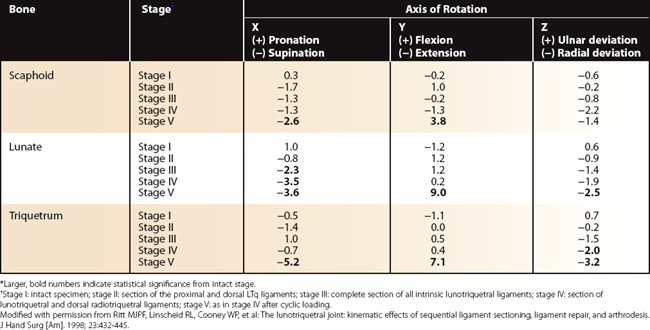
One factor that should be taken into account is the effect of cyclic loading on the generation of abnormal patterns of motion. Horii and colleagues25 applied “some degree of manipulation” after sectioning of the ligaments. It may require secondary attenuation from prolonged cyclic loading to produce the clinical findings. Ritt and colleagues38 simulated gradual attenuation of the remaining ligaments by repetitively loading the joint before analyzing carpal motion. The values of static carpal malalignment changed dramatically: the static malalignment increased in magnitude (stage V in Table 40-1).
1. Dharap AS, Lutfi I, Abu-Hijleh MF. Population variation in the incidence of the medial (hamate) facet of the carpal bone lunate. Anthropol Anz.. 2006;64:59-65.
2. Galley I, Bain GI, McLean JM. Influence of lunate type on scaphoid kinematics. J Hand Surg.. 2007;32:842-847.
3. Mastella DJ, Zelouf DS. Anatomy of the lunotriquetral joint. Atlas Hand Clin.. 2004;9:1-6.
4. Mikic ZD. Arthrography of the wrist joint. J Bone Joint Surg Am.. 1984;66:371-378.
5. Ritt MJPF, Stuart PR, Berglund LJ, et al. Rotational stability of the carpus relative to the forearm. J Hand Surg [Am].. 1995;20:305-311.
6. Wiesner L, Rumelhart C, Pham E, Comtet JJ. Experimentally induced ulno-carpal instability: a study on 13 cadaver wrists. J Hand Surg [Br].. 1996;21:24-29.
7. Berger RA. Arthroscopic anatomy of the wrist and distal radioulnar joint. Hand Clin.. 1999;15:393-413.
8. Viegas SF, Yamaguchi S, Boyd NL, Patterson RM. The dorsal ligaments of the wrist: anatomy, mechanical properties, and function. J Hand Surg [Am].. 1999;24:456-468.
9. Ambrose L, Posner MA. Lunate-triquetral and midcarpal joint instability. Hand Clin.. 1992;8:653-668.
10. Feipel V, Rooze M. The capsular ligaments of the wrist. Eur J Morphol.. 1997;35:87-94.
11. Garcia-Elias M. Soft-tissue anatomy and relationships about the distal ulna. Hand Clin.. 1998;14:165-176.
12. Hogikyan JV, Louis DS. Embryologic development and variations in the anatomy of the ulnocarpal ligamentous complex. J Hand Surg [Am].. 1992;17:719-723.
13. Lichtman DM, Noble WH III, Alexander CE. Dynamic triquetrolunate instability: Case report. J Hand Surg [Am].. 1984;9:185-188.
14. Lichtman DM, Schneider JR, Swafford AR, Mack GR. Ulnar midcarpal instability—clinical and laboratory analysis. J Hand Surg.. 1981;6:515-523.
15. Trumble TE, Bour CJ, Smith RJ, Glisson RR. Kinematics of the ulnar carpus related to the volar intercalated segment instability pattern. J Hand Surg [Am].. 1990;15:384-392.
16. Weaver L, Tencer AF, Trumble TE. Tensions in the palmar ligaments of the wrist: I. The normal wrist. J Hand Surg [Am].. 1994;19:464-474.
17. Mizuseki T, Ikuta Y. The dorsal carpal ligaments: their anatomy and function. J Hand Surg [Br].. 1989;14:91-98.
18. Zancolli ER. Localized medial triquetral-hamate instability: anatomy and operative reconstruction-augmentation. Hand Clin.. 2001;17:83-96.
19. Ritt MJPF, Bishop AT, Berger RA, et al. Lunotriquetral ligament properties: a comparison of three anatomic subregions. J Hand Surg [Am].. 1998;23:425-431.
20. Berger RA, Imaeda T, Berglund L, An KN. Constraint and material properties of the subregions of the scapholunate interosseous ligament. J Hand Surg [Am].. 1999;24:953-962.
21. Hagert E, Garcia-Elias M, Forsgren S, Ljung BO. Immunohistochemical analysis of the wrist ligament innervation in relation to their structural composition. J Hand Surg [Am].. 2007;32:30-36.
22. Kobayashi M, Berger RA, Nagy L, et al. Normal kinematics of carpal bones: a three-dimensional analysis of carpal bone motion relative to the radius. J Biomech.. 1997;30:787-793.
23. Berger RA, Crowninshield RD, Flatt AE. The three-dimensional rotational behaviors of the carpal bones. Clin Orthop Relat Res.. 1982;167:303-310.
24. De Lange A: A kinematic study of the human wrist joint. Thesis, University of Nijmegen, the Netherlands, 1987.
25. Horii E, Garcia-Elias M, An KN, et al. A kinematic study of lunotriquetral dissociations. J Hand Surg.. 1991;16:355-362.
26. Moojen TM, Snel JG, Ritt MJ, et al. In vivo analysis of carpal kinematics and comparative review of the literature. J Hand Surg.. 2003;28:81-87.
27. Moojen TM, Snel JG, Ritt MJ, et al. Three-dimensional carpal kinematics in vivo. Clin Biomech.. 2002;7:506-514.
28. Nakamura K, Beppu M, Patterson RM, et al. Motion analysis in two dimensions of radial-ulnar deviation of type I versus type II lunates. J Hand Surg.. 2000;25:877-888.
29. Galley I, Bain GI, McLean M. Influence of lunate type on scaphoid kinematics. J Hand Surg.. 2007;32:842-847.
30. Garcia-Elias M, Pitágoras T, Gilabert-Senar A. Relationship between joint laxity and radio-ulno-carpal joint morphology. J Hand Surg [Br].. 2003;28:158-162.
31. Melone CP, Nathan R. Traumatic disruption of the triangular fibrocartilage complex: pathoanatomy. Clin Orthop Relat Res.. 1992;275:65-73.
32. Smith DK, Murray PM. Avulsion fractures of the volar aspect of triquetral bone of the wrist: a subtle sign of carpal ligament injury. AJR Am J Roentgenol. 1996;166:609-614.
33. Viegas SF, Patterson RM, Peterson PD, et al. Ulnar-sided perilunate instability: an anatomic and biomechanic study. J Hand Surg [Am].. 1990;15:268-278.
34. Mayfield JK. Patterns of injury to carpal ligaments: a spectrum. Clin Orthop Relat Res.. 1984;187:36-42.
35. Leibovic SJ, Geissler WB. Treatment of complex intra-articular distal radius fractures. Orthop Clin North Am.. 1994;25:685-706.
36. Kolkin L: Wrist arthroscopy. Paper presented at the AAOS annual meeting, Washington, DC, 1992.
37. Geissler WB, Fernandez DL. Percutaneous and limited open reduction of the articular surface of the distal radius. J Orthop Trauma.. 1991;5:255-264.
38. Ritt MJPF, Linscheid RL, Cooney WP, et al. The lunotriquetral joint: kinematic effects of sequential ligament sectioning, ligament repair, and arthrodesis. J Hand Surg [Am].. 1998;23:432-445.
39. Reagan DS, Linscheid RL, Dobyns JH. Lunotriquetral sprains. J Hand Surg [Am].. 1984;9:502-514.
40. Li G, Rowen B, Tokunaga D, et al. Carpal kinematics of lunotriquetral dissociations. Biomed Sci Instrum.. 1991;27:273-281.
* This section is reprinted from Garcia-Elias M, Ritt MJPF: Lunotriquetral dissociation: pathomechanics. Atlas of Hand Clinics 2004; 9(1):7-15.
[/level-membership-for-orthopaedics-category][not-level-membership-for-orthopaedics-category]
CHAPTER 40 Kinematics of the Lunotriquetral Joint
Lunotriquetral injury is less frequently seen with distal radius fracture than one of the triangular fibrocartilage complex (TFCC) or scapholunate ligament injuries. One of the problems with lunotriquetral disorders is that most patients have normal imaging studies and fall under the broad and often vexing category of patients with ulnar-sided wrist pain. However, these disorders can have devastating effects on carpal mechanics and, unless properly treated, disruptions of the lunotriquetral supporting ligaments may result in substantial instability of the carpus. Knowledge of these effects and potential consequences will aid the treating physician in offering the patient the best possible outcome.
Functional Anatomy
Joint Anatomy
The relevant midcarpal articulation is between the distal articular surfaces of the lunate and triquetrum and the proximal surfaces of the capitate and hamate. A sagittal ridge can divide the lunate articular surface into a radial and ulnar fossa, and in these cases the proximal surface of the hamate articulates with the lunate. The incidence of this type II lunate varies considerably and is reported in 27% to 63% of adults.1,2 Otherwise, the distal surface of the lunate is concave in both coronal and sagittal planes.
The hamate-triquetral articulation has a helicoid or screw-shaped configuration. The plane of the joint is not parallel to the articular surface of the distal hamate with the fourth and fifth metacarpals but is situated at a substantial angle (reported as high as 90 degrees3).
Ligament Anatomy
The lunotriquetral joint is stabilized by an intricate arrangement of ligaments (Fig. 40-1). The intrinsic (both origin and insertion are within the carpus) lunotriquetral ligament is “C” shaped and is actually composed of three discrete regions: true ligaments dorsally and palmarly with collinear fascicles of collagen and a proximal region composed of fibrocartilage (Fig. 40-2). This proximal region has a wedge-shaped cross-sectional geometry and is reminiscent of a meniscus. In normal subjects there should be no communication between the midcarpal and radiocarpal joints but the proximal region of the lunotriquetral joint can be perforated by age. Because the proximal membrane contributes very little to the overall lunotriquetral stability, a defect at this level is not a sign of instability but can be a normal physiological, albeit age-related, finding, caused by wear. Mikic4 found up to 55% of lunotriquetral perforations past the third decade.
Radioulnocarpal Ligaments
Most extrinsic ligaments across the radioulnocarpal joint are obliquely oriented relative to the longitudinal axis of the forearm. Based on this, they may be subdivided into two groups: ligaments that prevent excessive passive supination of the proximal row relative to the forearm (anti-supination ligaments) and ligaments that control passive pronation (anti-pronation ligaments).5,6
Three ligaments act synergistically to prevent the proximal row to passively supinate beyond normal. The first is the palmar ulnotriquetral ligament that originates at the fovea near the base of the ulnar styloid. In approximately 90% of normal adults, the ulnotriquetral ligament is split distally to form an orifice that connects the radiocarpal and pisotriquetral joints.7 Second is the ulnolunate ligament that arises from the palmar edge of the triangular fibrocartilage (TFC) and runs obliquely toward its distal insertion into the anterior aspect of the lunate. Palmar to the ulnolunate and ulnotriquetral ligaments is the ulnocapitate ligament, which reinforces both these ligaments before passing anterior to the lunotriquetral joint, where it interdigitates with the fibers of the palmar region of the lunotriquetral interosseous ligament. It arises from the ulna at the fovea where the dorsal and palmar radioulnar ligaments also attach. Third, the dorsal radiotriquetral ligament is a wide, fan-shaped ligament that connects the dorsal edge of the distal radius to the dorsal rim of the triquetrum.8–12
Midcarpal Ligaments
The ulnar limb of the arcuate ligament, also known as the palmar triquetrum/hamate/capitate ligamentous complex, strongly connects the triquetrum to the distal carpal row.10,13–16 It consists of a group of fan-shaped fascicles formed by dense collagen fibers that links the distal anterior edge of the triquetrum to the palmar aspects of the hamate and capitate. This ligament can be regarded as an anti-supination ligament. The only dorsal midpalmar crossing ligament is the dorsal intercarpal ligament. It arises from the dorsal ridge of the triquetrum, courses transversely along the distal edge of the lunate, and fans out to insert on the dorsal rim of the scaphoid, the trapezium, and the trapezoid bones.8,10,17 This ligament can be characterized as an anti-pronation ligament.
There is no dorsal or ulnar ligament between the triquetrum and hamate. Because the midcarpal joint is not a true hinge articulation, there are no vertically oriented ligaments. Their absence is functionally substituted by the extensor carpi ulnaris tendon, which is a thick sheath that may act as a dynamic joint stabilizer.18
Mechanics
Material and Constraint Properties
Results of material property testing of the lunotriquetral ligament showed that the palmar region of the ligament is not only thicker but indeed stronger than the dorsal portion of the ligament (average yield strengths: 301 N and 121 N, respectively).19 The palmar region was found to constrain primarily translation, whereas the dorsal region provides the majority of rotational constraint. The fibrocartilaginous proximal region failed at 64 N and was the least important constraint in all directions. The morphology and material and constraint properties of the lunotriquetral ligament are the exact opposite as found in the scapholunate ligament.20 In a way, the lunate could be thought of as a “torque-suspended” bone between the scaphoid and the triquetrum, much in the manner of a spring. This “torque suspension” concept, for which there is now sufficient evidence, is of importance for the discussion and understanding of dorsiflexed intercalated segment instability (DISI) and volar-flexed intercalated segment instability (VISI).
Recently, immunohistochemical analysis of wrist ligament innervation showed that sensory important ligaments were primarily related to the triquetrum while mechanically important ligaments were primarily located in the radial, force-bearing column of the wrist. The triquetrum and its ligamentous attachments are regarded as key elements in the generation of the proprioceptive information necessary for adequate neuromuscular wrist stabilization.21
