INTRODUCTION
What is respiration?
The ‘bottom line’ of an account of the complicated process of respiration begins with a flow of
The need for respiration
One definition of the success of a species of organism, in evolutionary terms, is how well it can maintain constant the composition of the fluid surrounding its individual cells (its internal environment) despite changes in its external environment (surroundings getting dryer, colder, warmer etc.). This process is called homeostasis and requires energy. Most of the energy generated by our tissues is the result of oxidation of food substrates, and this is the reason we need a flow of OXYGEN IN. Neophytes in physiology often emphasize the role of the respiratory system in providing this oxygen, and certainly an uninterrupted supply is important, particularly for the nervous system, but of more immediate importance is the removal of CO2. The word oxygen means ‘acid producer’ (Greek, oxy; acid; gen, to produce), and the major product of our oxidative metabolism is the acid gas CO2. The accumulation of CO2 would result in acidification of the body fluids. The importance of removing this CO2 can be demonstrated by rebreathing from a plastic bag for a few minutes. The unpleasant sensation that forces you to stop this rather dangerous experiment is due to over stimulation of the reflex that controls breathing to get rid of this gas. You will see later (Chapter 8) that CO2 produces its acidic effect by reacting with water to form carbonic acid.
Diffusion in respiration and the circulation
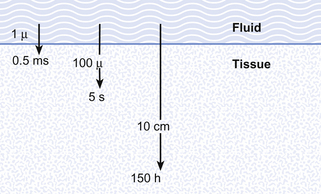
Although in human beings the same passive mechanism of diffusion alone supplies and removes these gases from our bodies (there is no active chemical transport), the phenomenon of diffusion is maximized by complicated respiratory and circulatory systems which accomplish what the pond water does for the amoebae in providing a supply of and a sink for these gases. The lungs promote diffusion by having an enormous surface area, which is very thin, through which diffusion can take place easily. A surface of over 90 m2 is enclosed in a lung volume of less than 10 L. This functional 90 m2 is often reduced in disease, by thickening of the membrane, excess fluid in the lungs, or by a reduction in the supply of air or blood. The circulation of the blood forms the transport link between the diffusion site of the lungs and the diffusion site of the capillaries within the tissues. The distances involved in this link are enormous in molecular terms, and diffusion would be totally useless to transport gas over the metre or so between the lungs and distal tissues of our bodies. This transport is accomplished in seconds by the circulation (Fig. 1.1).
Timing in the circulation and respiration
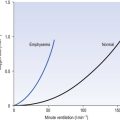
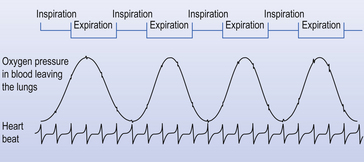
The processes of breathing and the beating of the heart are both cyclic events. One involves the inhalation of air and then its exhalation; the other involves filling of the heart with blood and then its ejection into the circulation. The time courses of these two cycles are very different: at rest you may take 12 breaths in the minute the heart beats 60 times, ejecting 5 L of blood through the lungs (see Fig. 1.2).
Basic science of respiration
All these changes, just like all the events in respiration, are properly described in terms of the basic sciences physics and chemistry. These are generally not the favourite subjects of students of the basic medical sciences. We have therefore included at the end of the book a short section (Appendix) on the most relevant parts of physics and chemistry that a student should understand in order to understand respiration. That section is not obligatory to students confident with these subjects. The Appendix, which is intended to aid not torment, will repay scrutiny by students who have any doubts about their grasp of basic science. That this basic science is integral to understanding normal respiration and diseased states is illustrated when we take an overview of human respiration and point out where the phenomena we describe apply (Fig. 1.3).
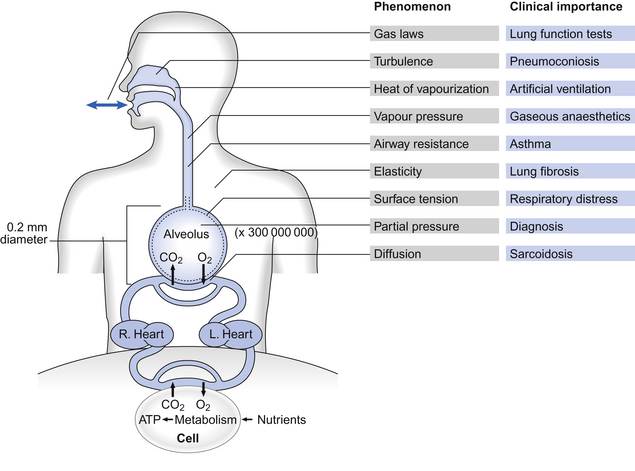
These examples of the importance of the basic sciences in understanding the respiratory system do not mean that a great deal, or a great depth, of knowledge is required. The Appendix contains all that is required to understand the contents of this book. However, there is a vocabulary that is specific to the respiratory system, and it is probably helpful for you to be introduced to it here.
Case 1.1 Introduction: 2
Examination of the respiratory system
A clinical examination of the respiratory system includes examination of the hands, tongue, neck and chest wall, as well as percussion (tapping) and auscultation (listening with a stethoscope) of the chest.
These are the important findings in a clinical examination of the respiratory system:
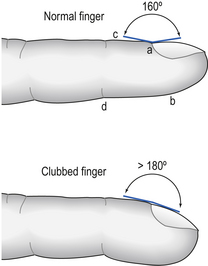
1. Finger clubbing. Inspecting the hands is an important part of examining the respiratory system. As well as looking for peripheral cyanosis (see below) it is important to look for finger clubbing. Clubbing is present when the normal angle at the nailbed is lost, the curvature of the nail is increased and there is increased mobility of the nail on the nailbed (the nail is fluctuant) (Fig. 1.4). It is not known for certain why finger clubbing occurs, but it is present in a number of respiratory diseases, including bronchial carcinoma, bronchiectasis and pulmonary fibrosis. Clubbing is also present in some non-respiratory diseases.
2. Cyanosis. Cyanosis means a blue tinge to skin or mucous membranes and indicates the presence of deoxygenated haemoglobin (p. 106). Cyanosis may be either central or peripheral. Central cyanosis means blueness of the lips and tongue. Because these organs are covered in mucosa rather than skin, cyanosis is more evident there than in the face, for example. Blood does not travel far from the heart to reach the tongue and lips, and so if they are cyanosed it suggests that blood leaving the left ventricle is deoxygenated, either because of lung disease or as a result of certain forms of heart abnormality. Peripheral cyanosis means blueness of the extremities and is usually most evident in the fingernails and toenails. In the absence of central cyanosis it usually suggests inadequate circulation to the periphery.
3. Trachea. The trachea can be felt in the neck above the sternum and it is examined to assess whether it is lying in the midline or deviated to one side. Tracheal deviation can occur in a number of lung diseases, including pneumonia and pneumothorax.
4. Inspection of the chest. Examination of the chest itself starts with inspection. The shape of the chest may be abnormal: for example, in asthmatics the chest is often unusually expanded and rounded – so-called barrel chest. Surgical scars or other abnormalities of the skin on the chest wall may be present. The patient is asked to take a deep breath and the movements of the chest wall are noted. Movements of the chest wall may be limited by abnormalities of the spine or chest wall itself, or by abnormalities of the underlying lung.
5. Percussion. Percussion essentially means tapping the patient’s chest and listening to the sound that is produced. Normally, the chest sounds hollow or resonant if the underlying lung is filled with air, but a dull sound is heard if there is fluid in the intrapleural space (pleural effusion) or if the alveoli of the underlying lung are filled with fluid. If there is a pneumothorax and there is air between the chest wall and the lung, then percussion may be hyperresonant, in other words the chest sounds more hollow than normal.
6. Auscultation. Auscultation means listening to the lungs with a stethoscope. Normally, it is possible to hear air quietly entering and leaving the lungs without there being any added sounds. Breath sounds like this are called vesicular. Breath sounds may be absent or very quiet if there is a pleural effusion or a pneumothorax. There may also be sounds present in addition to breath sounds. Where gas passes through narrowed airways a sound like a musical note may be produced. These sounds are called wheeze or rhonchi, and are usually heard during expiration and are most likely to be heard in asthma or chronic bronchitis, although if airway narrowing is very severe, no gas flow takes place and there is no wheeze. Crackles or crepitations may also be heard on auscultation. Crackles probably represent the opening of closed airways and are most commonly heard in chronic bronchitis, pulmonary fibrosis and pulmonary oedema.
Case 1.1 Introduction: 3
Looking at a chest X-ray
In the clinical sections of the book, cases are frequently illustrated with chest X-rays demonstrating a range of abnormalities. This section will introduce you to the appearance of a normal chest X-ray so that you can appreciate the abnormal chest X-ray appearances that are associated with some respiratory conditions.
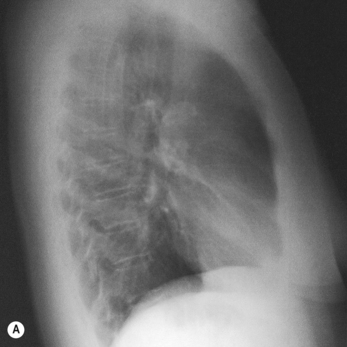
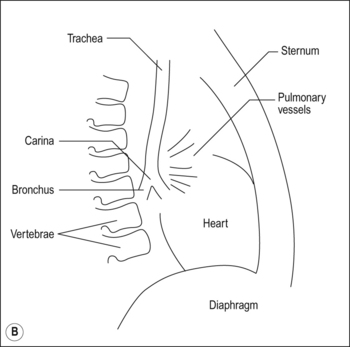
If a patient is too unwell to stand in front of the photographic plate – for example if they are too ill to leave his/her bed – the X-ray may be taken with the photographic plate behind the patient and with the X-rays administered from in front of the patient. This is an anteroposterior chest X-ray; it is also possible to take a lateral chest X-ray from the side (see Fig. 1.6(A)).
On the chest X-ray of a healthy person in Fig. 1.5 the following structures are visible:
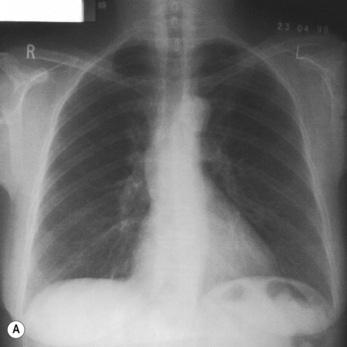
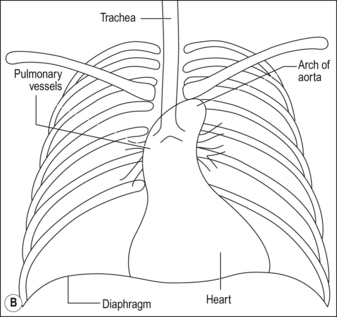
1. Bones. The ribs, sternum and thoracic vertebrae can usually all be seen on a chest X-ray.
2. Heart. The outline of the heart is clearly visible. If the heart is enlarged, for example as a result of heart disease, this will be evident. The border of the heart may not appear sharp and distinct if the lung tissue around it is diseased.
3. Aorta. The outline of the aorta is usually visible as it arises from the heart and arches round in the thorax.
4. Trachea. Because the trachea is filled with air through which X-rays can pass easily, it appears as a dark structure in the midline. It is usually possible to see the carina, where the trachea divides into the two main bronchi.
5. Pulmonary vessels. The pulmonary vessels are visible as they pass from the heart into the lungs.
6. Diaphragm. The outline of the diaphragm is usually clearly visible. The right-hand side of the diaphragm is usually higher than the left. Collapse of the lung or damage to the phrenic nerve may cause the diaphragm to be shifted upwards, whereas emphysema and other diseases that increase lung volume may cause the diaphragm to be shifted downwards. If the outline of the diaphragm is not sharp, particularly where the shadows of the diaphragm and the ribs intersect (the costophrenic angle) this suggests that there is fluid in the intrapleural space adjacent to the diaphragm.
7. Lungs. As the lungs are filled mainly with air, X-rays pass through them easily and they appear relatively dark on a chest X-ray. However, it is generally possible to make out the shadows of large blood vessels as they pass through the lung tissue. If there is fluid in the alveoli, for example as a result of oedema or infection, the lung fields will appear lighter as fewer X-rays will pass through them. If an area within the lungs appears darker than normal, this suggests that there is more air present than usual. This might be as a result of emphysema or as a result of a pneumothorax.
Respiratory symbols – the language of the respiratory system
Primary units are given in capital letters (see Table 1.1):
Table 1.1
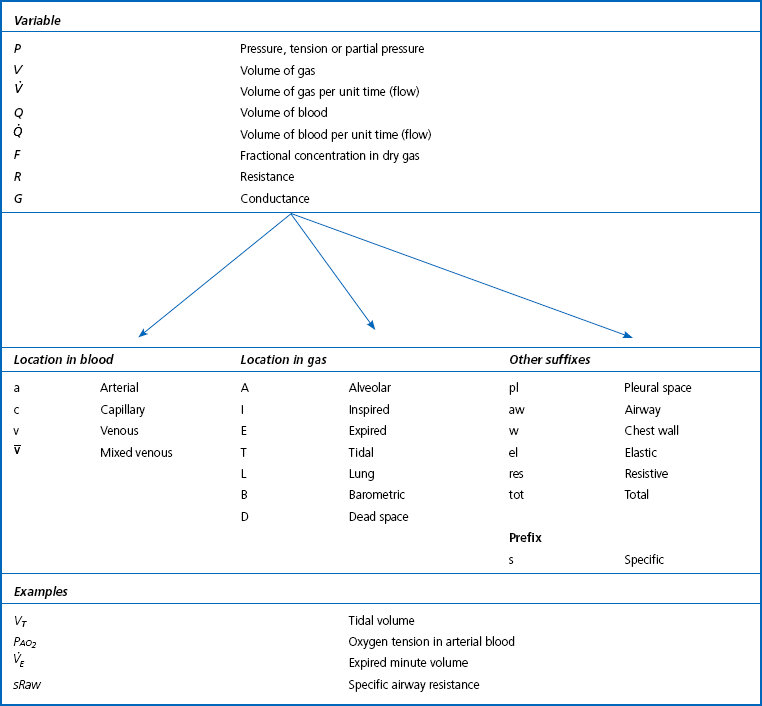

Locations in the gas phase are also given capital letters but smaller than the primary units:

Locations in blood are identified by lower-case letters:

The primary symbol is written first, followed by the qualifying symbol at a lower level.
Drugs
Drugs are chemicals which change the natural functions of the body. Most prescribed drugs have therapeutic properties. Just as Fig. 1.3 demonstrates where specific physical phenomena have particular importance in the respiratory system, Table 1.2 gives examples of conditions where specific types of drugs are used therapeutically in treatment of specific conditions or for specific procedures.
Table 1.2
Drugs and the respiratory system
| Drug name | Type | Condition treated |
| Oxymetazoline | α-agonist | Nasal congestion |
| Atropine | Muscarinic cholinergic antagonist | Excess mucus secretion |
| Prednisolone | Corticosteroid | Allergic rhinitis |
| Chlorpheniramine | Antihistamine | Rhinorrhea |
| Succinylcholine | Neuromuscular blocking | Facilitate tracheal intubation |
| Dextromethorphan | Synthetic narcotic analgesic | Non-productive cough (suppression) |
| Salbutamol (Isoproterenol, USA) | β2 agonist (bronchodilator) | Asthma |
| Cromoglicate | Inflammatory-cell stabilizer | Asthma |
| Beclometasone | Anti-inflammatory corticosteroid | Asthma |
| Azathioprine | Cytotoxic immunosuppressant | Diffuse connective tissue |
| Aminopenicillin etc. | Antibiotic | Pneumonia and other infections |
| Amphotericin B | Antifungal | Fungal infections |