23.11 Intraosseous infusions
Equipment


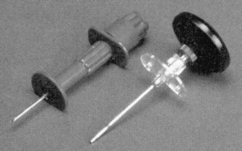
 Commercially available IO needles have more durable parts intended for penetration of bone. There are several styles (Fig. 23.11.1). A central stylet is universal. There are short, 2.5-cm, needles for neonates and infants and longer, 3.0 and 3.5-cm, needles for older children. Some needles have stylets with multifaceted cutting edges intended for a rotary insertion, others have bevels, and others can be screwed in place. The shaft may have side ports.
Commercially available IO needles have more durable parts intended for penetration of bone. There are several styles (Fig. 23.11.1). A central stylet is universal. There are short, 2.5-cm, needles for neonates and infants and longer, 3.0 and 3.5-cm, needles for older children. Some needles have stylets with multifaceted cutting edges intended for a rotary insertion, others have bevels, and others can be screwed in place. The shaft may have side ports.


Preparation
Identification of the entry site
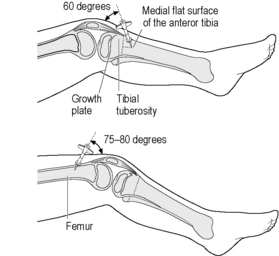
The best site in children is the anteromedial aspect of the proximal tibia lateral to the tibial tuberosity. Alternative sites are the distal end of the femur 2–3 cm above the patella in the midline, and the medial malleolus at the ankle (Fig. 23.11.2). The sternum is not recommended in children. In adults, the medial malleolus may be the best site, although studies are lacking.
Procedure







Tips
The EZ-IO
Mechanical devices such as the EZ-IO have simplified the insertion of an IO needle as they are not dependent on the manual process. The EZ-IO (Vidacare, San Antonio, TX, USA) is a reusable battery-powered device that operates like a small drill. The driver itself is a sealed unit that is good for about 700 insertions. The EZ-IO uses a bevelled drill tip that rotates into the IO space at a preset depth (Fig. 23.11.3).

Brunette D.D., Fischer R. Intravascular access in paediatric cardiac arrest. Ann Emerg Med. 1988;6:577.
Fiser D.H. Intraosseous infusion. N Engl J Med. 1990;322:1579.
Johnson L., Kissoon N., Fiallos M., et al. Use of intraosseous blood to assess blood chemistries and haemoglobin during cardiopulmonary resuscitation with drug infusions. Crit Care Med. 1999;27:1147-1152.
Phillips B., Zideman D., Garcia-Castrillo L., et al. European Resuscitation Council guidelines 2000 for advanced paediatric life support. Resuscitation. 2001;48:231-324.
Vidal R., Kissoon N., Gaylor M. Compartment syndrome following intraosseous infusion. Paediatrics. 1993;91:1201-1202.
Wenzel V., Lindner K.H., Augenstein S., et al. Intraosseous vasopressin improves coronary perfusion pressure rapidly during cardiopulmonary resuscitation in pigs. Crit Care Med. 1999;27:1565-1569.
Tobias J.D., Ross A.K. Intraosseous infusions: a review for the anesthesiologist with a focus on pediatric use. Anesth Analg. 2010;110(2):391-401.



