[level-membership-for-radiology-category] Most commonly diagnosed benign small bowel (SB) tumor (easy to recognize on CT)
Most common cause of SB intussusception (symptomatic)
• GI stromal tumor (GIST)
Most common type (if duodenum is included)
Often large, exophytic, with central necrosis, may communicate with lumen
• Leiomyoma
Calcifications and necrosis are common (in this rare tumor)
• Hemangioma
Usually small, ± calcified phleboliths
• Neural tumors
Schwannoma, paraganglioma, neurofibroma
Multiple SB neurofibromas may be seen in neurofibromatosis type 1 (NF1)
TOP DIFFERENTIAL DIAGNOSES
• Intestinal metastases and lymphoma
• Small bowel carcinoma
• Intramural hematoma
• Ectopic pancreas
CLINICAL ISSUES
• Asymptomatic (most common)
• GI bleeding, intestinal obstruction, intussusception
DIAGNOSTIC CHECKLIST
• Small bowel follow-through: Very low yield procedure to identify small bowel tumors
CT enterography is best imaging test
Capsule endoscopy or double balloon endoscopy may miss submucosal masses
(Left) CT shows a fat-density mass diagnostic of a lipoma. The mass appears to be intraluminal, due to the effects of chronic peristaltic tugging on the mass, causing it to elongate into an intraluminal polypoid shape.
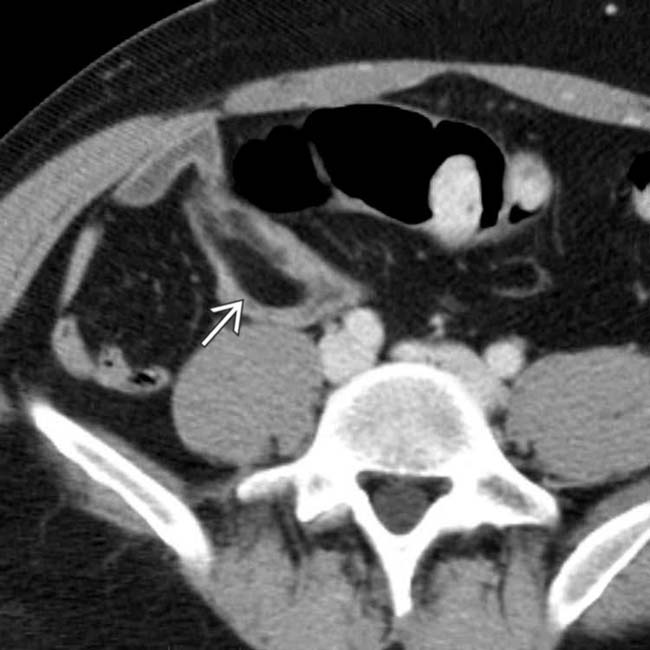
(Right) Axial CECT shows a well-circumscribed mass with heterogeneous enhancement in the pelvis, intimately associated with the adjacent small bowel. This proved to be a leiomyoma of the bowel with necrosis accounting for the heterogeneity.
(Left) A coronal CT section shows a homogeneous, soft tissue density mass within the wall of the duodenum without luminal obstruction. The homogeneous soft tissue density supports the diagnosis of leiomyoma and excludes lipoma, but other masses, such as GI stromal or neural tumors, could have a similar appearance.
(Right) Axial CET shows a cylindrical mass within the lumen of the 3rd portion of duodenum, without signs of bowel obstruction. This was a paraganglioma arising from the duodenal wall.
Upper GI series shows a large duodenal mass with central ulceration in this patient with a gastrointestinal stromal tumor.
Axial CECT shows a large mass in the medial wall of the duodenum with a large central ulceration in this patient with a gastrointestinal stromal tumor.
Axial CECT shows a duodenal teratoma that is comprised of fat, calcification, and soft tissue.
Axial CECT shows a fat-density intramural/luminal mass in this patient with jejunal lipoma.
[/level-membership-for-radiology-category][not-level-membership-for-radiology-category] Most commonly diagnosed benign small bowel (SB) tumor (easy to recognize on CT)
Most common cause of SB intussusception (symptomatic)
• GI stromal tumor (GIST)
Most common type (if duodenum is included)
Often large, exophytic, with central necrosis, may communicate with lumen
• Leiomyoma
Calcifications and necrosis are common (in this rare tumor)
• Hemangioma
Usually small, ± calcified phleboliths
• Neural tumors
Schwannoma, paraganglioma, neurofibroma
Multiple SB neurofibromas may be seen in neurofibromatosis type 1 (NF1)
TOP DIFFERENTIAL DIAGNOSES
• Intestinal metastases and lymphoma
• Small bowel carcinoma
• Intramural hematoma
Buy Membership for Radiology Category to continue reading. Learn more here









 diagnostic of a lipoma. The mass appears to be intraluminal, due to the effects of chronic peristaltic tugging on the mass, causing it to elongate into an intraluminal polypoid shape.
diagnostic of a lipoma. The mass appears to be intraluminal, due to the effects of chronic peristaltic tugging on the mass, causing it to elongate into an intraluminal polypoid shape.
 with heterogeneous enhancement in the pelvis, intimately associated with the adjacent small bowel. This proved to be a leiomyoma of the bowel with necrosis accounting for the heterogeneity.
with heterogeneous enhancement in the pelvis, intimately associated with the adjacent small bowel. This proved to be a leiomyoma of the bowel with necrosis accounting for the heterogeneity.
 within the wall of the duodenum without luminal obstruction. The homogeneous soft tissue density supports the diagnosis of leiomyoma and excludes lipoma, but other masses, such as GI stromal or neural tumors, could have a similar appearance.
within the wall of the duodenum without luminal obstruction. The homogeneous soft tissue density supports the diagnosis of leiomyoma and excludes lipoma, but other masses, such as GI stromal or neural tumors, could have a similar appearance.
 within the lumen of the 3rd portion of duodenum, without signs of bowel obstruction. This was a paraganglioma arising from the duodenal wall.
within the lumen of the 3rd portion of duodenum, without signs of bowel obstruction. This was a paraganglioma arising from the duodenal wall.
 in this patient with a gastrointestinal stromal tumor.
in this patient with a gastrointestinal stromal tumor.
 in this patient with a gastrointestinal stromal tumor.
in this patient with a gastrointestinal stromal tumor.
 that is comprised of fat, calcification, and soft tissue.
that is comprised of fat, calcification, and soft tissue.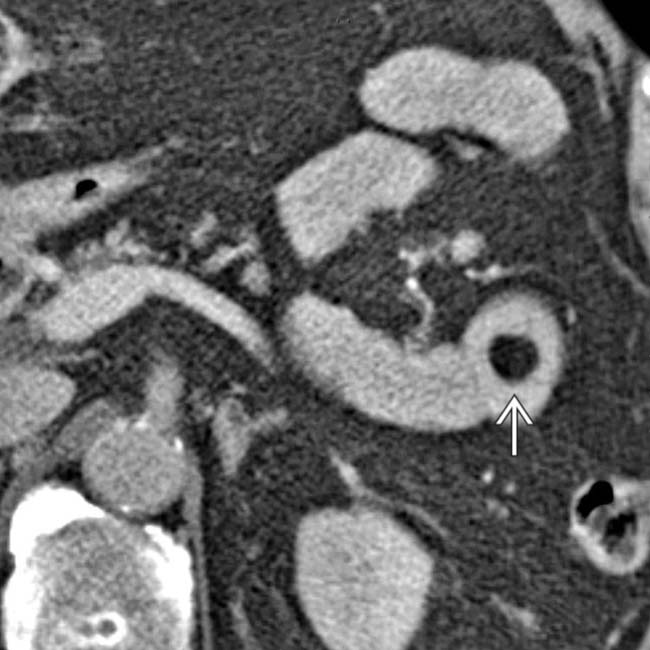
 in this patient with jejunal lipoma.
in this patient with jejunal lipoma.