Fry, LC, et al. Utility of double-balloon enteroscopy for the evaluation of malabsorption. Dig Dis. 2008; 26(2):134–139.
Katoch, P, et al. Lymphangiectasia of small intestine presenting as intussusception. Indian J Pathol Microbiol. 2008; 51(3):411–412.
Safatle-Ribeiro, AV, et al. Secondary lymphangiectasia of the small bowel: utility of double balloon enteroscopy for diagnosis and management. Dig Dis. 2008; 26(4):383–386.
Vignes, S, et al. Primary intestinal lymphangiectasia (Waldmann’s disease). Orphanet J Rare Dis. 2008; 3:5.
Yakami, Y, et al. [Efficacy of double balloon enteroscopy for patients with intestinal lymphangiectasia, case report of primary intestinal lymphangiectasia.]. Nippon Shokakibyo Gakkai Zasshi. 2008; 105(11):1612–1618.
Pratz, KW, et al. Intestinal lymphangiectasia with protein-losing enteropathy in Waldenstrom macroglobulinemia. Medicine (Baltimore). 2007; 86(4):210–214.
Mazzie, JP, et al. Congenital intestinal lymphangiectasia: CT demonstration in a young child. Clin Imaging. 2003; 27(5):330–332.
Yang, DM, et al. Localized intestinal lymphangiectasia: CT findings. AJR Am J Roentgenol. 2003; 180(1):213–214.
Stevens, RL, et al. The CT halo sign: a new finding in intestinal lymphangiectasia. J Comput Assist Tomogr. 1997; 21(6):1005–1007.
Puri, AS, et al. Intestinal lymphangiectasia: evaluation by CT and scintigraphy. Gastrointest Radiol. 1992; 17(2):119–121.



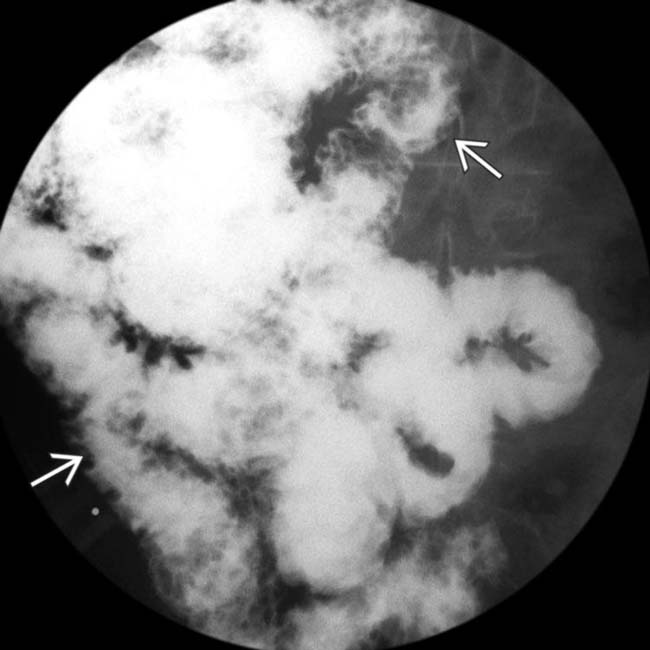
 throughout the entire SB, proved to be due to lymphangiectasia.
throughout the entire SB, proved to be due to lymphangiectasia.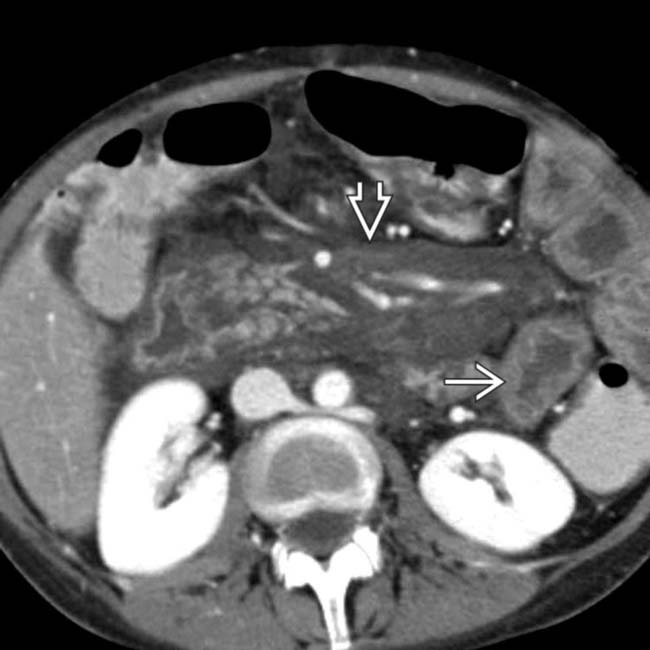
 . More striking is the marked edema within the mesentery
. More striking is the marked edema within the mesentery  .
.
 , mesenteric edema
, mesenteric edema  , as well as ascites
, as well as ascites  and enlarged, low density lymph nodes
and enlarged, low density lymph nodes  .
.
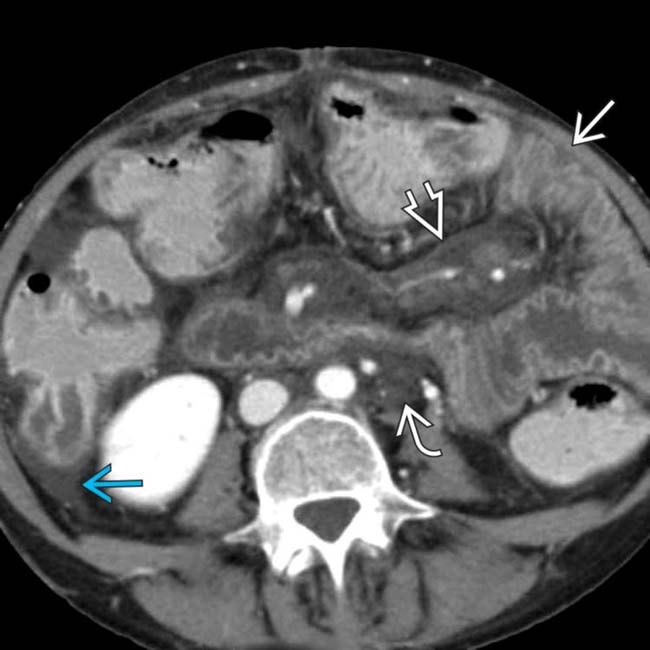
 and colon and additional hypodense nodes or infiltration at the root of the SB mesentery
and colon and additional hypodense nodes or infiltration at the root of the SB mesentery  . Intestinal lymphangiectasia was the final diagnosis.
. Intestinal lymphangiectasia was the final diagnosis.
























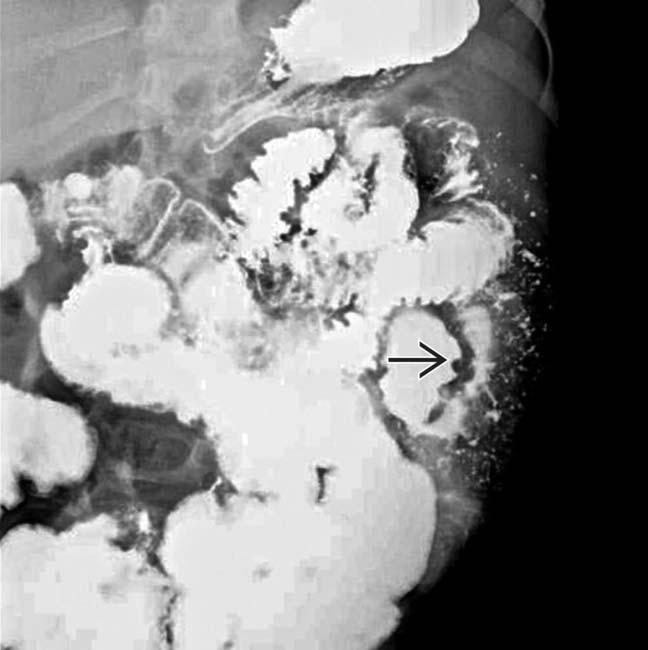
 . This process was diffuse throughout all the small intestine.
. This process was diffuse throughout all the small intestine.
 .
.


