[level-membership-for-hematology-oncology-and-palliative-medicine-category]
Chapter 61 Inhibitors in Hemophilia A and B
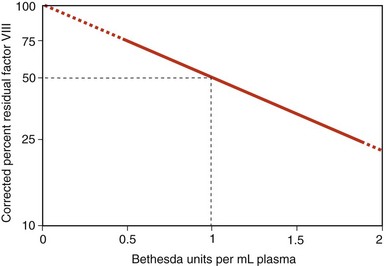
Figure 61-1 BETHESDA ASSAY FOR FACTOR VIII INHIBITOR QUANTITATION.
(From Konkle BA: Clinical approach to the bleeding patient. In Colman RW, Marder VJ, Clowes AW, et al, editors: Hemostasis and thrombosis, Philadelphia, 2006, Lippincott, Williams & Wilkins, p 1147.)
Treatment of Bleeding in a Patient With FVIII Deficiency and an Inhibitor
Low Titer, Low Responder
Mild Bleeding
• Local and conservative measures, such as rest, ice, compression, and elevation
• If the patient is known to respond to DDAVP (i.e., mild hemophilia A), 0.3 µg/kg IV or 300 µg intranasal (150 µg per nostril; 150 µg for patients <50 kg) for minor bleeding or treatment before minor surgery
• Oral antifibrinolytic therapy (ε-aminocaproic acid or tranexamic acid) for mucosal bleeding
• FVIII dosing to raise the level to 50%
• Recombinant FVIIa (90 to 120 µg/kg, followed by 90 µg/kg every 2 to 3 hours)
• Activated prothrombin complex concentrates (50 to 100 units/kg, with maximum daily dose of 200 units/kg)
• Concurrent treatment with antifibrinolytics should be administered with caution
Life- or Limb-Threatening Bleeding
• FVIII dosing to maintain FVIII activity levels at 100%
• Recombinant FVIIa (270 µg/kg for one dose may be considered with caution versus 90 µg/kg every 2 to 3 hours)
• Activated prothrombin complex concentrates (100 units/kg, with maximum daily dose of 200 units/kg)
• Concurrent treatment with antifibrinolytics should be administered with caution
Low Titer, High Responder
Mild Bleeding
• Local and conservative measures, such as rest, ice, compression, and elevation
• If the patient is known to respond to DDAVP (i.e., mild hemophilia A), 0.3 µg/kg IV or 300 µg intranasal (150 µg for patients <50 kg) for minor bleeding or treatment before minor surgery
• Oral antifibrinolytic therapy (ε-aminocaproic acid or tranexamic acid) for mucosal bleeding
• Recombinant factor VIIa (270 µg/kg, bolus may be considered with caution versus 90 µg/kg every 2 to 3 hours)
• Activated prothrombin complex concentrates (100 units/kg, with a maximum daily dose of 200 units/kg, may induce anamnesis)
High Titer, High Responder
Mild Bleeding
• Local and conservative measures, such as rest, ice, compression, and elevation
• Oral antifibrinolytic therapy (ε-aminocaproic acid or tranexamic acid) for mucosal bleeding
• Recombinant FVIIa (270 µg/kg, should be considered with caution versus 90 µg/kg every 2 to 3 hours)
• Activated prothrombin complex concentrates (100 units/kg, with a maximum daily dose of 200 units/kg)
• Concurrent treatment with antifibrinolytics should be administered with caution
Life- or Limb-Threatening Bleeding
• Recombinant FVIIa (270 µg/kg, should be considered with caution versus 90 µg/kg IV every 2 to 3 hours)
• Activated prothrombin complex concentrates (100 units/kg, with a maximum daily dose of 200 units/kg)
• If available, immunoadsorption can be attempted to rapidly lower the inhibitor titer so as to allow use of FVIII
[/level-membership-for-hematology-oncology-and-palliative-medicine-category][not-level-membership-for-hematology-oncology-and-palliative-medicine-category]
Chapter 61 Inhibitors in Hemophilia A and B
Figure 61-1 BETHESDA ASSAY FOR FACTOR VIII INHIBITOR QUANTITATION.
(From Konkle BA: Clinical approach to the bleeding patient. In Colman RW, Marder VJ, Clowes AW, et al, editors: Hemostasis and thrombosis, Philadelphia, 2006, Lippincott, Williams & Wilkins, p 1147.)
Treatment of Bleeding in a Patient With FVIII Deficiency and an Inhibitor
Low Titer, Low Responder
Mild Bleeding
• Local and conservative measures, such as rest, ice, compression, and elevation
• If the patient is known to respond to DDAVP (i.e., mild hemophilia A), 0.3 µg/kg IV or 300 µg intranasal (150 µg per nostril; 150 µg for patients <50 kg) for minor bleeding or treatment before minor surgery
• Oral antifibrinolytic therapy (ε-aminocaproic acid or tranexamic acid) for mucosal bleeding
• FVIII dosing to raise the level to 50%
[/not-level-membership-for-hematology-oncology-and-palliative-medicine-category]
