[level-membership-for-basic-science-category]
Infections of the Urinary System
After reading this chapter, the student should be able to:
• Identify the parts of the urinary system that are the sites of the most common urinary tract infections (UTI)
• Identify the microorganisms that are the most common causes of UTIs
• Describe typical symptoms of a UTI
• Identify and describe the three most common types of UTIs
• List common risk factors for a UTI
• Identify the patient group with the highest risk for a UTI and give reasons why
• Describe the typical diagnosis process to identify a UTI
• Identify and discuss various methods of treatments for UTIs
• List and discuss prevention factors for UTIs in men, women, children, the elderly, and individuals who are immunocompromised
• Identify some of the major groups of antibiotics specifically used in treating a UTI
Introduction
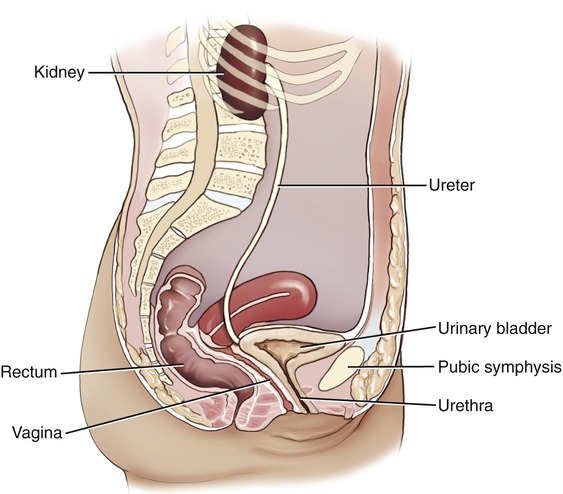
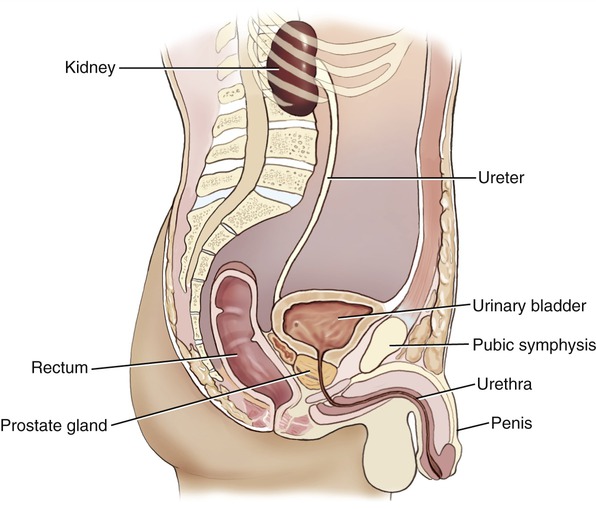
The urinary system consists of the kidneys, ureters, urinary bladder, and urethra (Figure 15.1). The kidneys are the central organ of the system and are responsible for filtering wastes from the blood as well as for removing any excess liquid, thus forming urine. The functional units in the kidneys are the nephrons (Figure 15.2) and in addition to their filtering capacity they also keep a stable balance of minerals, salts, and other substances to maintain the homeostasis (the maintenance of a relatively stable environment of the body) of the blood. Furthermore, the kidneys produce erythropoietin, the hormone that aids in the formation of red blood cells. The ureters are narrow tubes that carry the urine from the kidneys to the urinary bladder, which stores the urine for later expulsion from the body. The urine stored in the urinary bladder is emptied through the urethra, whose length varies between male and female. The male urethra is longer than the female and the opening is located on the penis. Normally urine is sterile, free of any microorganisms; however, an infection can occur when infectious organisms, usually bacteria from the gastrointestinal tract, gain access to the opening of the urethra and multiply. The urinary tract is one of the most common sites of bacterial infection, particularly in females.
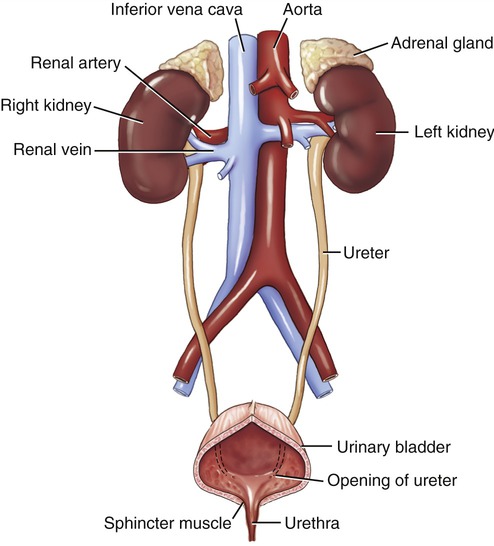
The urinary system consists of the kidneys, ureters, the urinary bladder, and the urethra.
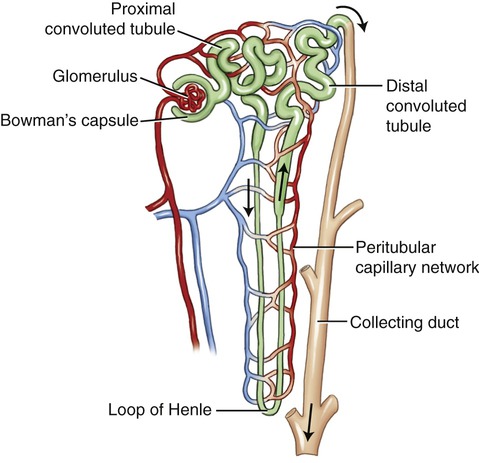
Each nephron has a glomerulus, a Bowman’s capsule, and a tubular portion that consists of the proximal convoluted tubule, the loop of Henle, the distal convoluted tubule, and a collecting duct.
Urinary Tract Infections (UTIs)
• Burning/painful sensation when urinating (dysuria)
• Frequency of urination, passing only small amounts each time
• Presence of blood or pus in the urine, or a cloudy, strong-smelling urine
• Uncomfortable pressure above the pubic bone in women
• A fullness of the rectum in men
Urethritis
Urethritis is a localized infection usually limited to the urethra. It can be caused by E. coli but also by Chlamydia or Mycoplasma, because the urethra is also associated with organs of the reproductive system. A common source of this infection for older or hospitalized patients is a catheter. If not treated early, the infection can travel up the catheter and spread the infection to the urinary bladder. Trichomonas vaginalis, a protozoan, has also been associated with urethritis as well as vaginitis (see Chapter 16, Infections of the Reproductive System). Enterococci and Candida albicans are other organisms that occasionally can cause urethritis.
Diagnosis of UTIs
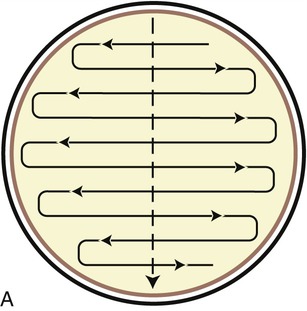
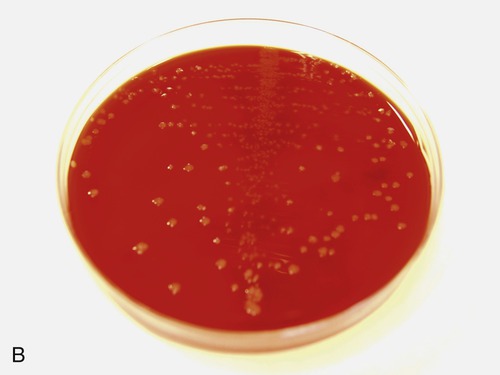
Typically the detection/diagnosis process occurs in two stages. The first stage involves gathering a sample of urine for evaluation and the second stage involves testing the antibiotic sensitivity of any microorganisms that may be present. The collection of urine involves a procedure called a “clean catch,” wherein the patient thoroughly washes the genital area and then collects a midstream sample in a sterile container. The sample can then be both cultured for microbial growth as well as examined microscopically to determine the presence of microbes, pus, or blood. Typically the urine sample is streaked on a blood agar plate, using a special pattern to provide a semiquantitative analysis of the sample (Figure 15.3). If microbial growth occurs on the growth medium, the organisms can be tested with various antibiotics to identify the most effective one against a specific pathogen. This step is called a sensitivity test. The general term for the presence of bacteria in the urine is bacteriuria.
Risk Factors for UTIs
• Diabetics: Patients with diabetes often have a higher risk for UTIs because of changes in the immune system that make them more vulnerable to infection.
• Patients with catheters: Patients with catheters in place for extended periods of time have an increased risk of infection of the urethra and ultimately the urinary bladder. About 20% of patients catheterized for more than 30 days will develop UTIs. The catheter itself can act as a location for the development of a biofilm (see Chapter 3, Cell Structure and Function), resulting in a greater diversity of species than may normally be found in the urinary bladder.
• Infants/children with abnormalities of the urinary tract: In boys the infections usually occur before the first birthday, and in girls the infections are common around the age of 3 years, overlapping with the period of toilet training. Infections in girls at a young age are especially dangerous because chronic infections over a long time period can lead to serious kidney damage. Some abnormalities that may lead to UTIs in children include vesicoureteral reflux (VUR), urinary obstruction, and dysfunctional voiding. VUR involves the reverse flow of urine from the bladder up the ureters and back to the kidneys. This condition can be corrected by surgical repositioning of the connection between the ureters and the urinary bladder in order to prevent the reverse flow. Urinary obstructions can include narrow ureters, kidney stones, or improper connection of the ureters to the kidneys or urinary bladder. Obstructions are typically solved by corrective surgical procedures or dissolving of the stones. Dysfunctional voiding is often a behavioral problem wherein children may intentionally delay voiding the bladder. This problem involves a simple process of behavior modification.
• Women: The largest group of patients who suffer with UTIs are adult women. Anatomically, women have a higher risk of infection because of the short length of the urethra and the close proximity of the opening to the anus (Figure 15.4), thus presenting a higher risk of fecal bacteria entering the urethra. Statistics also indicate that the incidence of infection increases with age and sexual activity. Rates of infection are particularly high in postmenopausal women because of incomplete urinary bladder emptying, and the loss of estrogen, which results in changes in the vaginal flora. Furthermore, the loss of normal flora such as lactobacilli decreases the level of competition with organisms such as E. coli. In addition, the tissues of the urethra become thinner and more fragile due to a decrease in estrogen, providing a good environment for opportunistic organisms. Sexual activity can irritate the urethra, allowing bacteria to more easily penetrate and move to the urinary bladder. The regular use of a diaphragm as a contraceptive measure can also lead to increased risk of infection particularly in premenopausal women.
• Men: The occurrence of UTIs in men under the age of 50 years is relatively low. The infections that do occur in this group are largely due to sexual activity that causes irritation of the urethra and subsequent penetration of the bacteria into the urinary bladder (Figure 15.5). There is evidence that uncircumcised men are at higher risk of developing a UTI. Most cases that occur in older men are associated with an obstruction or a medical procedure involving the placement of a catheter. In most cases an obstruction may be the result of kidney stones, blood clots, tumors, scar tissue, or a structural defect such as kinking of the ureters or a compression of the ureters by fibrous connective tissue. Surgical procedures can correct most of these defects. In the case of kidney stones, sound shock waves are commonly used if the stones do not pass through the system naturally; surgery is generally not the first course of treatment. Those older men who have an infection of the prostate gland are also at higher risk for a UTI.
Prevention and Treatment of UTIs
Prevention of UTIs
• Diabetics: Preventive measures generally involve actions that improve the health of a diabetic, such as careful control of glucose levels and blood pressure. Those measures will ensure a healthy immune system that in turn will help to prevent UTIs.
• Patients with catheters: The best measures to prevent a UTI are frequent cleaning of the catheter and associated areas, and its removal, done as soon as it is no longer necessary. Although there is some debate about when a transurethral catheter should be changed, the practice in most health facilities is to do a monthly change. On diagnosis of a UTI, catheters need to be changed immediately. Because of the potential for UTIs and other complications, federal regulations mandate that indwelling catheters should be used only when there is valid medical justification.
• Infants/children with abnormalities of the urinary tract: The most effective measure is early identification of the problem followed by corrective surgery or procedures done as soon as possible.
• Women: The following measures have been suggested to help prevent infections in women:
• Don’t resist the urge to urinate.
• Wipe from front to back to prevent bacteria around the anus from being spread to the area of the urethra.
• Take showers instead of tub baths.
• Cleanse the genital area before sexual intercourse.
• Avoid using feminine hygiene products, which may irritate the urethra.
Treatment of UTIs
HEALTHCARE APPLICATION
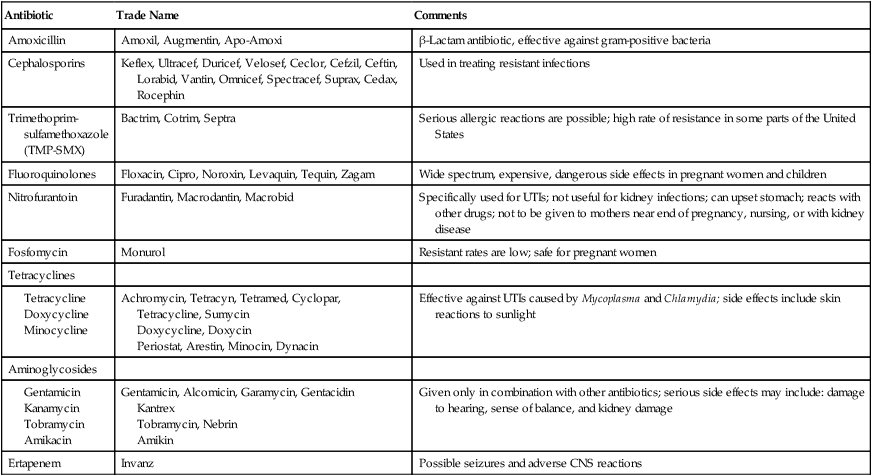
UTI Antibiotics
| Antibiotic | Trade Name | Comments |
| Amoxicillin | Amoxil, Augmentin, Apo-Amoxi | β-Lactam antibiotic, effective against gram-positive bacteria |
| Cephalosporins | Keflex, Ultracef, Duricef, Velosef, Ceclor, Cefzil, Ceftin, Lorabid, Vantin, Omnicef, Spectracef, Suprax, Cedax, Rocephin | Used in treating resistant infections |
| Trimethoprim-sulfamethoxazole (TMP-SMX) | Bactrim, Cotrim, Septra | Serious allergic reactions are possible; high rate of resistance in some parts of the United States |
| Fluoroquinolones | Floxacin, Cipro, Noroxin, Levaquin, Tequin, Zagam | Wide spectrum, expensive, dangerous side effects in pregnant women and children |
| Nitrofurantoin | Furadantin, Macrodantin, Macrobid | Specifically used for UTIs; not useful for kidney infections; can upset stomach; reacts with other drugs; not to be given to mothers near end of pregnancy, nursing, or with kidney disease |
| Fosfomycin | Monurol | Resistant rates are low; safe for pregnant women |
| Tetracyclines | ||
Doxycycline, Doxycin
Periostat, Arestin, Minocin, Dynacin
Kantrex
Tobramycin, Nebrin
Amikin
Bacterial Infections
Most UTIs are caused by bacteria and the primary microorganism responsible for most UTIs is E. coli; however, Chlamydia, a gram-negative, coccoid obligate parasite, and Mycoplasma, a gram-negative, pleomorphic facultative anaerobe, may also cause infections. Some other organisms that have been associated with UTIs are Klebsiella, Proteus, Enterobacter, Citrobacter, Serratia, Pseudomonas, Enterococcus, and coagulase-negative Staphylococcus. The actual designation as a bacterial UTI is based on the presence of greater than 100,000 colony-forming units (CFU)/1 ml of urine. A summary of the most common bacterial infection of the urinary system is shown in Table 15.1.
TABLE 15.1
Bacterial Diseases of the Urinary System
| Infection/Disease | Pathogen | Symptoms | Treatment |
| Urinary bladder infection (cystitis) | Escherichia coli, Staphylococcus saprophyticus | Difficulty and/or pain in urination | Trimethoprim-sulfamethoxazole |
| Pyelonephritis | Mostly Escherichia coli | Fever, back pain | Cephalosporin |
| Leptospirosis | Leptospira interrogans | Headaches, muscle pain, fever, kidney failure | Doxycycline |

Viral Infections
Viral UTIs are rare, but certain viruses may be found in urine even in the absence of urinary tract infections/disease. These viruses include human polyomaviruses JC and BK, cytomegalovirus (CMV), adenovirus, hantavirus, and a number of other viruses that can infect the kidneys, including mumps and HIV. Viruses are increasingly recognized as the cause of lower UTIs, especially hemorrhagic cystitis after stem cell and organ transplantation. Early diagnosis and treatment of viral UTIs may prevent the significant morbidity of hemorrhagic cystitis. Diagnosis of viral UTIs is based on molecular techniques including the polymerase chain reaction (see Chapter 25, Biotechnology), which allows quantification of the viral load. The current drug of choice against viral UTIs is cidofovir, because it is active against the most common viral pathogens.
Cytomegalovirus
Cytomegalovirus infections are widely recognized as potentially serious causes of complications in the lung, spinal fluid, and brain, and also as the cause of graft failure in renal transplantation. Cytomegalovirus can also cause asymptomatic shedding in the urine of congenitally infected infants (see Congenital Infections in Chapter 23, Human Age and Microorganisms).
Adenovirus
Adenoviruses are a group of viruses that typically cause respiratory illnesses (see Chapter 11, Infections of the Respiratory System), but can also cause infections of the urinary and intestinal tracts. Some serotypes of the adenovirus have been implicated as the cause of hemorrhagic cystitis. In immunocompromised patients severe adenoviral infections are serious complications, especially in patients receiving hematopoietic stem cell transplantations. The most critical and fatal for these transplant patients are adenovirus-induced urinary tract infections and acute necrotizing tubulointestinal nephritis.
Fungal Infections
Fungal infections of the urinary tract affect primarily the bladder and the kidneys, with Candida species being the most common cause. However, all invasive fungi such as Cryptococcus neoformans, Aspergillus species, Mucoraceae species, Histoplasma capsulatum, Blastomyces species, and Coccidioides immitis may infect the kidneys as a result of a systemic or disseminated mycotic infection. Candida infections are usually associated with a urinary catheter, often after bacteriuria and antibiotic therapy. Renal candidiasis spread by the blood commonly originates from the gastrointestinal tract. Other Candida infections can occur in patients with nephrostomy tubes, other permanent indwelling devices, and stents. At high risk for these infections are patients who are immunocompromised because of chemotherapy, AIDS, or immunosuppressants after transplantation. Fungal pathogens are a cause of the increasing numbers of healthcare-associated (nosocomial) infections (see Healthcare-associated [Nosocomial] Infections in Chapter 9, Infection and Disease).
Parasitic Infections
Few parasites cause UTIs in humans; they include the protozoan Trichomonas vaginalis and the helminth Schistosoma haematobium. Trichomonas vaginalis can cause urethritis in both males and females, but in females it often also causes vaginitis (see Chapter 16, Infections of the Reproductive System).
Schistosomiasis is one of the most common parasitic infestations in the world, caused by flukes in the genus Schistosoma (see Helminths in Chapter 8, Eukaryotic Microorganisms). The organism associated with urinary schistosomiasis is Schistosoma haematobium, found in the Middle East, India, Portugal, and Africa; to date it does not exist in the United States. Typically the infection involves the bladder, but ureteral involvement can be found in as many as 30% of the patients. Adult Schistosoma is present in the venous plexuses around the urinary bladder, where they release their eggs. The eggs then cross the wall of the bladder, causing hematuria and fibrosis of the bladder. Subsequently the bladder becomes calcified, which increases the pressure on the ureters and kidneys. The main cause of schistosomiasis is the contamination of water supplies with human waste.
Summary
• The most common sites of infection in the urinary tract are the urethra, ureters, urinary bladder, and kidneys.
• The microorganism most frequently identified as the cause of a UTI is E. coli, with Mycoplasma and Chlamydia also being significant culprits.
• The most common UTIs are urethritis—infection of the urethra, cystitis—infection of the urinary bladder, and pyelonephritis—infection of the kidneys.
• The detection/diagnosis of a UTI occurs in two stages: gathering a sample of urine for testing and the subsequent testing of any organisms that may be present for antibiotic susceptibility.
• The risk factors associated with UTIs vary from individual to individual, but the largest risk groups are women and the elderly (particularly those with catheters or previous urinary tract problems).
• The primary treatment for UTIs is antibiotics. The specific antibiotic used and the prescribed regimen depends on the target microorganism and the general health/condition of the infected individual.
• Incidences of recurring infections are of particular concern for women, among whom as many as one in three will experience a recurrence within 1 year.
• Preventive measures to avoid a UTI in women include the following: take showers instead of baths, don’t resist the urge to urinate, wipe from front to back, clean the genital area before intercourse, urinate after intercourse, drink plenty of water, and avoid feminine hygiene products that may irritate the urethra.
• Preventive measures to avoid a UTI in men include the following: drink plenty of water, clean the genitals before intercourse, don’t resist the urge to urinate, and urinate after intercourse.
• The antibiotics commonly used to treat UTIs include amoxicillin, nitrofurantoin, trimethoprim, a combination of trimethoprim and sulfamethoxazole, gentamicin, ciprofloxacin, cefadroxil, mecillinam, fosfomycin, and the cephalosporins.
Review Questions
1. The main organs/structures of the urinary system are:
a. Large intestine, stomach, esophagus, urinary bladder
b. Small intestine, liver, urinary bladder, urethra
2. The primary bacterium responsible for most UTIs is:
3. Diagnosis of a UTI is a two-stage process that involves:
a. Collecting a blood sample and conducting a physical examination of the bladder
b. Exploratory surgery and radiation therapy
c. Collecting a urine sample and testing for antibiotic susceptibility of the organism
d. Modifying the diet of the patient and conducting a physical examination of the urethra
4. The group most susceptible to recurring UTIs is:
5. Which of the following has not been shown to be a preventive against UTIs in women?
a. Taking a daily dose of 81 mg of aspirin
b. Urinating soon after sexual intercourse
6. The urinary tract infection involving infection of the urinary bladder is called:
7. The urinary tract infection of the kidneys is called:
8. An effective method for treating a UTI is:
9. The following are typical symptoms of a UTI:
a. Vomiting, blood in the urine
b. Painful urination, cloudy urine
10. What anatomical features in women can increase the possibility of a UTI?
a. A shorter urethra, close proximity of the anus to the urethral opening
b. A longer urethra, smaller urinary bladder
c. Longer ureters, larger urinary bladder
d. A longer urethra, close proximity of the anus to the vagina
11. The __________ are the central organs of the urinary system and are responsible for filtering wastes from the blood.
12. __________ is a UTI that occurs in the urinary bladder.
13. The method of collecting urine in which the patient washes the genital area and collects a midstream sample in a sterile container is called the __________ __________ procedure.
14. __________ and __________ are genera of organisms that are usually associated with UTIs related to sexual activity.
15. Glomerulonephritis is also referred to as __________ disease.
16. Describe some of the functions of a normal healthy body that help prevent the occurrence of UTIs.
17. List two reasons why postmenopausal women are at higher risk for UTIs.
18. Briefly describe the steps in the diagnosis of a UTI.
19. Name the typical antibiotic treatment regimen for UTIs.
20. Outline the path of infection that begins as urethritis and eventually becomes pyelonephritis.
[/level-membership-for-basic-science-category][not-level-membership-for-basic-science-category]
Infections of the Urinary System
After reading this chapter, the student should be able to:
• Identify the parts of the urinary system that are the sites of the most common urinary tract infections (UTI)
• Identify the microorganisms that are the most common causes of UTIs
• Describe typical symptoms of a UTI
• Identify and describe the three most common types of UTIs
• List common risk factors for a UTI
• Identify the patient group with the highest risk for a UTI and give reasons why
• Describe the typical diagnosis process to identify a UTI
• Identify and discuss various methods of treatments for UTIs
• List and discuss prevention factors for UTIs in men, women, children, the elderly, and individuals who are immunocompromised
• Identify some of the major groups of antibiotics specifically used in treating a UTI
Introduction
The urinary system consists of the kidneys, ureters, urinary bladder, and urethra (Figure 15.1). The kidneys are the central organ of the system and are responsible for filtering wastes from the blood as well as for removing any excess liquid, thus forming urine. The functional units in the kidneys are the nephrons (Figure 15.2) and in addition to their filtering capacity they also keep a stable balance of minerals, salts, and other substances to maintain the homeostasis (the maintenance of a relatively stable environment of the body) of the blood. Furthermore, the kidneys produce erythropoietin, the hormone that aids in the formation of red blood cells. The ureters are narrow tubes that carry the urine from the kidneys to the urinary bladder, which stores the urine for later expulsion from the body. The urine stored in the urinary bladder is emptied through the urethra, whose length varies between male and female. The male urethra is longer than the female and the opening is located on the penis. Normally urine is sterile, free of any microorganisms; however, an infection can occur when infectious organisms, usually bacteria from the gastrointestinal tract, gain access to the opening of the urethra and multiply. The urinary tract is one of the most common sites of bacterial infection, particularly in females.
The urinary system consists of the kidneys, ureters, the urinary bladder, and the urethra.
Each nephron has a glomerulus, a Bowman’s capsule, and a tubular portion that consists of the proximal convoluted tubule, the loop of Henle, the distal convoluted tubule, and a collecting duct.
Urinary Tract Infections (UTIs)
• Burning/painful sensation when urinating (dysuria)
• Frequency of urination, passing only small amounts each time
• Presence of blood or pus in the urine, or a cloudy, strong-smelling urine
• Uncomfortable pressure above the pubic bone in women
• A fullness of the rectum in men
Urethritis
Urethritis is a localized infection usually limited to the urethra. It can be caused by E. coli but also by Chlamydia or Mycoplasma, because the urethra is also associated with organs of the reproductive system. A common source of this infection for older or hospitalized patients is a catheter. If not treated early, the infection can travel up the catheter and spread the infection to the urinary bladder. Trichomonas vaginalis, a protozoan, has also been associated with urethritis as well as vaginitis (see Chapter 16, Infections of the Reproductive System). Enterococci and Candida albicans are other organisms that occasionally can cause urethritis.
Diagnosis of UTIs
Typically the detection/diagnosis process occurs in two stages. The first stage involves gathering a sample of urine for evaluation and the second stage involves testing the antibiotic sensitivity of any microorganisms that may be present. The collection of urine involves a procedure called a “clean catch,” wherein the patient thoroughly washes the genital area and then collects a midstream sample in a sterile container. The sample can then be both cultured for microbial growth as well as examined microscopically to determine the presence of microbes, pus, or blood. Typically the urine sample is streaked on a blood agar plate, using a special pattern to provide a semiquantitative analysis of the sample (Figure 15.3). If microbial growth occurs on the growth medium, the organisms can be tested with various antibiotics to identify the most effective one against a specific pathogen. This step is called a sensitivity test. The general term for the presence of bacteria in the urine is bacteriuria.
Risk Factors for UTIs
• Diabetics: Patients with diabetes often have a higher risk for UTIs because of changes in the immune system that make them more vulnerable to infection.
• Patients with catheters: Patients with catheters in place for extended periods of time have an increased risk of infection of the urethra and ultimately the urinary bladder. About 20% of patients catheterized for more than 30 days will develop UTIs. The catheter itself can act as a location for the development of a biofilm (see Chapter 3, Cell Structure and Function), resulting in a greater diversity of species than may normally be found in the urinary bladder.
• Infants/children with abnormalities of the urinary tract:
[/not-level-membership-for-basic-science-category]
