Chapter 41 Indwelling Access Devices
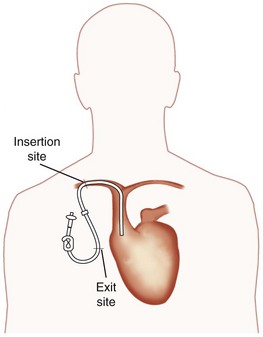
Figure 41-1 Schematic diagram of an indwelling central venous catheter in place. Insertion site refers to the insertion of the proximal end of the catheter into the chest wall. Clamp attached to the catheter is shown next to the Luer-Lok cap at the distal end.
(Modified from Hickman Subcutaneous Port, Use, and Maintenance and How to Care for Your Hickman or Broviac Catheter. Cranston, RI, Davol Inc.)
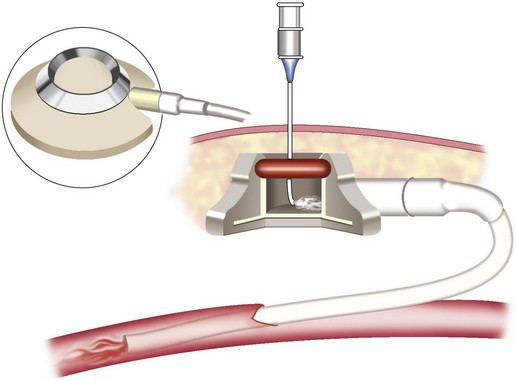
Figure 41-2 Totally implanted Hickman subcutaneous (central venous access) port with a noncoring needle in place.
(Modified from Hickman Subcutaneous Port, Use, and Maintenance and How to Care for Your Hickman or Broviac Catheter. Cranston, RI, Davol Inc.)
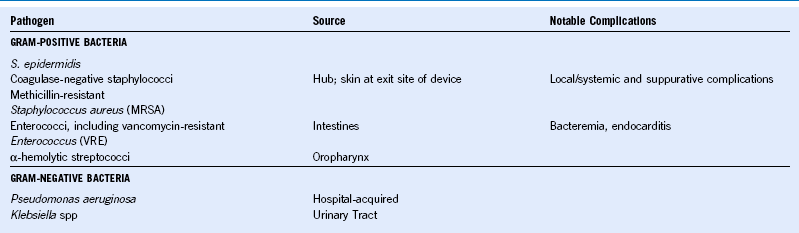
Infectious Indications for Device Removal
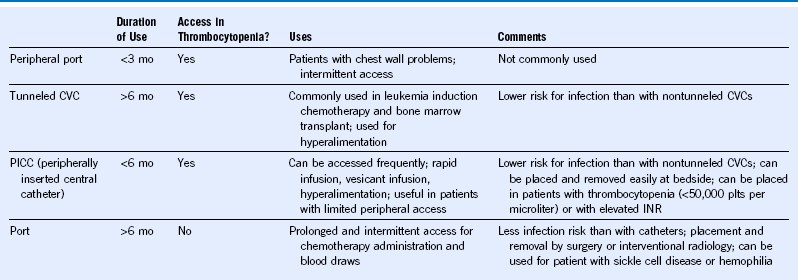
Venous Access Devices
Treatment of Vesicant Drug Extravasation
Treatment protocols for vesicant drug extravasation, including those recommended by the Oncology Nursing Society, are outlined in Table 41-2. When these protocols were used, 89% of vesicant extravasations were reported to resolve without additional therapy. However, 30% of anthracycline extravasations progressed to ulceration.
Table 41-2 Management of Vesicant Drug Extravasation
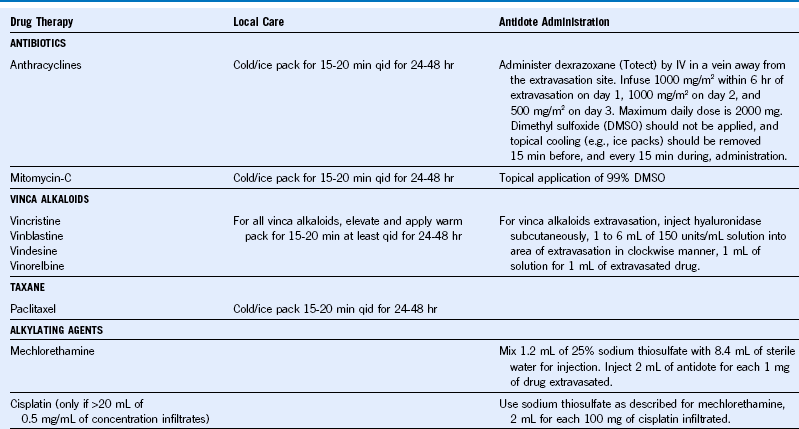
From Schulmeister L: Extravasation management: Clinical update, Semin Oncol Nurs 27:82, 2011.