Complications in Vitreoretinal Surgery
Good judgment is to make the best decision based on the known information in hand, and it is a product of experience. However, experience usually comes from the lessons learned from previously made bad judgments. As surgeons we are trained to predict and treat expected events during surgery. Unexpected events; however, are fact of life and generally the question is not if they will happen but when they will happen. They are frequently dangerous and can lead to undesirable outcome.
The knowledge of how to predict, treat, and prevent unexpected events during surgery is extremely valuable and would make vitreoretinal surgery safer, leading to improved visual outcome in patients. The more one is acquainted with unexpected events, the less they are considered unexpected since one has already seen these events happen and knows how they were handled and therefore the factor of surprise is eliminated.
In this chapter, experienced surgeons from around the world share with you their unexpected experiences during retinal surgery and show how they handle some of the most unusual surgical cases. Further, they share their surgical pearls on how to predict, prevent, and treat these unusual surgical cases.
Always Measure Prior to Trochar Insertion
Vitrectomy surgery with trochar systems reduces conjunctival trauma, scleral manipulation, iatrogenic peripheral breaks, postoperative inflammation, and corneal astigmatism.
Precise measuring of the location of the trochar insertion is crucial to assure a pars plana entrance into the eye, especially when utilizing an oblique insertion technique. Further, it is important that the insertion tunnel is parallel to the limbus so that the distance between the entrance point into the eye and limbus is the same as the scleral insertion point and limbus.
An insertion that is too anterior to the limbus (less than 3 mm posterior to the limbus) leads to an inadvertent insertion into the cilliary body which is very vascular and may cause bleeding as shown in the video(case 1). An anterior insertion may also lead to cataract formation or intraocular lens implant dislocation. In these cases the cannula needs to be removed and re-inserted.
An insertion that is too posterior to the limbus, (more than 4 mm posterior to the limbus) may lead to a subretinal trochar insertion inducing retinal breaks and retinal detachment (case 2). In these patients the iatrogenic breaks need to be treated similar to other peripheral breaks: thorough peripheral vitrectomy, endolaser, and tamponade.
It is important to always measure the distance of the trochar insertion form the limbus (range 3-4 mm posterior to the limbus depending on the lens status). One may use either a caliper or the other side of the trochar inserter (which also serves as a caliper) for measuring. If the trochar is not inserted at a correct distance to the limbus it should be removed and re-inserted correctly.
Suprachoroidal Infusion
Suprachoroidal infusion is a serious intra-operative complication during vitrectomy surgery. This complication has become more prevalent with the use of trochar systems.
At the beginning of the surgery, it is important to visualize the tip of the infusion cannula in the vitreous cavity prior to opening the infusion line. A well-constructed scleral wound may also prevent the dislodgement of the infusion cannula during surgery.
If the tip of the infusion cannula is dislodged into the suprachoroidal space during the surgery one should immediately stop the flow the infusion into the eye. Generally, the infusion needs to be re-inserted into the eye through a different trochar. Pulling back the original infusion trochar slightly outwards so that its tip is placed in the suprachoroidal space may help the draining of the suprachoroidal fluid. Many times the residual fluid in the suprachoroidal space can be left alone.
Subretinal Insertion of Endo-illuminator
Patient underwent combined vitrectomy surgery and scleral buckling for a total retinal detachment with PVR. The inferotemporal trochar was inserted and after the visualization of the tip of the infusion cannula, the infusion line was opened. As the endo-illuminator was inserted into the eye through the trochar (tunneled incision), it was noted that it was placed under the retina. The endo-illuminator was removed and the cannula was examined and the tip of the cannula was under the pars plana (video#1).
To resolve this situation one option would be to remove the trochar, suture the sclerotomy, and re-insert the trochar through a new sclerotomy. The simpler option is shown in the video #2:
The trochar was removed and re-inserted through the same sclerotomy without tunneling the incision (inserted almost perpendicular to the sclera). At this point, the tip of the endo-illuminator could be easily visualized. At the conclusion of the surgery the sclerotomy was sutured.
In the presence of pars plana detachment or hypotony the tunneled trochars could be placed under the pars plana. In these cases one may avoid tunneling the incision and insert the trochar perpendicular to the sclera. These sclerotomies would require suturing at the conclusion of surgery.
Dislocated IOL and Capsular Tension Ring
The patient was presented for the removal of a dislocated intraocular lens implant (IOL) after a difficult phaco-emulsification. During the surgery, after the IOL removal it was noted that the patient also had a capsular tension ring. Removal of the ring can be challenging due to their large size and their elasticity. They may also have extensions that can induce traction to the peripheral vitreous. It is important to remove the ring gently to minimize traction and to remove it by rotating it (rather than pulling it) out of the eye. In patients who present with a dislocated intra-ocular lens, after the removal of the lens it is important to inspect the anterior pars plana very carefully for the capsular tension ring. It can be difficult to detect and (if missed) may dislocate into the vitreous cavity over time.
Iatrogenic Breaks during the Induction of Posterior Vitreous Detachment
Formation of peripheral breaks during the induction of posterior vitreous detachment (PVD) in a patient with macular hole is demonstrated. If these patients generally have a very adhesive vitreous, the induction of PVD may induce peripheral breaks. The use of wide angle viewing system would allow the monitoring of peripheral retina during the induction of PVD.
At the beginning, the surgeon is paying attention to the optic nerve and the grasping of the Weiss ring. Once the Weiss ring is grasped and the PVD is in process of expanding, attention must be given to the peripheral retina to identify the location of the anterior vitreous base. This is the location where the vitreous can no longer be separated and breaks will form if suction/traction is applied.
In these patients it is extremely important to screen the periphery at the conclusion of the surgery. In the presence of peripheral breaks, a thorough peripheral vitrectomy should be performed around the breaks to relive any residual traction, followed by retinopexy, and possibly a tamponade agent.
Iatrogenic Macular Hole during VMT Surgery
This video illustrates the dangers of excessive traction on the fovea while detaching the posterior hyaloid in a case of vitreomacular traction syndrome, or VMT.
VMT is characterised by the presence of a partial vitreous detachment with strong adhesions to the macula, especially the fovea.
This patient had a long history of reduced vision. While using active aspiration over the disc to detach the hyaloid the surgeon is focused on looking for signs of vitreous separation from the disc rather than the traction vectors at the fovea as the fovea tissue is stretched before finally separating. In fact the central lucent area was assumed to be a cyst as no hole was present pre-operatively.
To summarize, observe the fovea closely while detaching the hyaloid in conditions with foveal thinning and strong vitreoretinal adhesions such as vitreomacular traction syndrome. In the presence of significant vitreo-macular adhesion and/or cystic macular changes one may trim the vitreous around the macular area rather than peeling it, leading to the un-roofing of macula.
Iatrogenic Breaks during the Delamination of Diabetic Traction Retinal Detachment
The newly designed 25G+ vitrectomy probes (Alcon Laboratories) have their opening closer to the tip when compared to 23 or 20 gauge probes. This proximity to the surface of the retina allows it to be used similar to scissors during the delamination of diabetic fibrous tissue. However, small iatrogenic retinal breaks may be formed during the delamination. The utilization of a bimanual technique would minimize this complication. In the bimanual technique the use of chandelier light would free up the surgeon’s hand to hold the forceps instead of the endo-illuminator. Keeping the level of the delaminating tissue stable with the forceps would allow the probe to cut the focal adhesion points more accurately. If these adhesion points are broad and difficult to be accessed with the vitreous cutter, then scissors should be used to make a dissection plane for subsequent tissue removal. The iatrogenic breaks need to be marked and treated with endolaser followed by a gas tamponade. It is important to alleviate all the traction around the breaks to prevent retinal re-detachment.
Point Pressure Hemostasis during Diabetic Vitrectomy
Intra-operative bleeding is common during diabetic dissection. Generally one can apply increased intra-ocular pressure or endodiathermy/endolaser to achieve hemostasis. However, none of these techniques are preferable since the retina is generally already ischemic with poor circulation. Lack of good hemostasis; however, can lead to significant bleeding during surgery and the removal of the pre-retinal blood can become challenging due to its “stickiness” to the surface of retina.
In this video an elegant technique is demonstrated in which gentle pressure is applied to the bleeding points with the tip of the cutter while simultaneously the blood is removed with the suction (if necessary). The intra-ocular pressure is not increased during this maneuver.
Iatrogenic Retinal Break during ERM Peeling
Retinal laceration is a serious and preventable complication of epiretinal membrane peeling. This video demonstrates a chorioretinal laceration during ERM peeling.
Having engaged the membrane it is important to elevate the membrane slightly while pulling. In the video, the membrane is peeled tangentially as shown by the proximity of the forceps tip to the shadow. This may be due to the inappropriate extrapolation from capsulorhexis where it is important not to lift the rhexis edge. Because of the concavity of the posterior pole the forceps move closer to the retina as the flap extends.
It is important to regularly re-grasp the membrane rather than peeling with a single grasp. Otherwise it is difficult to pay sufficient simultaneous attention to the forceps tips and the point at which the membrane is delaminating. In fact the surgeon is probably more focused on the delamination point rather than the location of the tip of the forceps.
To summarize: while peeling epiretinal membranes, lift the membrane rather than pulling tangentially as you would in a capsulorhexis and keep sight of the tip of the forceps at all times. It is important to remember that the posterior pole is concave (especially in high myopia) while peeling away from the center of the macula. Always assure that the forceps remain within the surgical field during the peeling.
Subretinal Brilliant Blue
J. Fernando Arevalo MD, FACS, Abdulaziz Adel Rushood MD
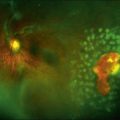
Approximately 0.3 ml of brilliant blue dye was used to stain the ILM during macular hole surgery. A significant resistance was noted at the beginning of the dye injection. To overcome this resistance additional pressure was applied. Sudden jet stream of brilliant blue was formed and it was noted that the dye has gained access to the subretinal space through the macular hole. The dye was immediately removed from the vitreous cavity, and the ILM was peeled in a circular fashion in the usual manner. The eye was filled with 16% perfluoropropane gas. Post-operative fundus examination and OCT indicated a closed macular hole with areas of choroidal hypereflectivity due to RPE and choriocapillaris atrophy. The brilliant blue dye was present in the subretinal space more than 3 months after surgery.
During the injection of any type of fluid, it is critical to inject slowly and away from the macula. If dye gains access to the subretinal space, remove it as much as possible and complete the surgery in the usual fashion.
Peripheral Retinal Detachment during Macular Hole Surgery
This 70-year-old woman underwent macular hole surgery and after separation of the posterior hyaloid, a peripheral retinal detachment was noted inferotemporally in the area of the infusion cannula. The management of the hole proceeded as usual with staining of brilliant blue to assist in ILM peeling. At the end of the procedure, a partial fluid-air exchange was made to prevent displacement of subretinal fluid into the macula. Under air, the infusion line was moved to another opening and the fundus was examined by indirect ophthalmoscopy. A retinal break was found at the ora serrata adjacent to the site of the cannula. It was treated with cryopexy, and an expanding concentration of gas was used. The patient was rotated into the prone position after surgery. In reviewing the video of this surgery it was noted that the angle of insertion of the trocar-cannula was aimed too posteriorly as it entered the eye.
Subretinal Hemorrhage
Subretinal hemorrhage may occur during vitrectomy surgery. The source of blood may be iatrogenic or from already existing breaks. When this occurs it is important to increase the intraocular pressure immediately to stop the bleeding (using the foot pedal). If the blood threatens the macula, perfluorocarbon liquid may be injected to protect the macula and push the subretinal hemorrhage away from the macula. In cases of large subretinal hemorrhage, the subretinal blood may be removed with a soft tip cannula through the original break or through a drainage retinotomy site.
Macular Fold
Andre J. Witkin MD and Jason Hsu MD
A 57-year-old patient presented with a macula-on rhegmatogenous retinal detachment (RRD), with a posterior linear tear at 1 o’clock. C3F8 gas (0.3cc) was injected into the vitreous with the goal of performing a staged pneumatic retinopexy; however, the next day the patient had a bullous macula-splitting RRD, with the gas bubble having moved into the subretinal space. A 23-gauge pars plana vitrectomy (PPV) surgery was performed that day, with creation of an anterior retinotomy to drain the subretinal gas and drainage of subretinal fluid through the original posterior retinal tear.
Two weeks after PPV, visual acuity was 20/400 due to a horizontal retinal fold that had formed through the macula, and a repeat 23-gauge PPV was performed that week. During surgery, a 41-gauge needle was used to inject balanced salt solution into the subretinal space around the retinal fold. A complete air/fluid exchange was then performed, and the sub-retinal fluid slowly coalesced in the posterior region of the retinal fold. After 5 minutes under air, the retina had completely unfolded. 20% SF6 was exchanged with air, and the patient was instructed to lie in the prone position for 5 days. Three weeks after surgery, the retinal fold had disappeared, and visual acuity had improved to 20/200. Three months after surgery, best-corrected visual acuity had improved to 20/30 and the retina remained flat. The following pearls maybe helpful in treating macular folds:
1. Inject balanced salt solution (BSS) via a translocation needle (e.g., 41-gauge cannula), preferably in an area near the macula but away from the fold.
2. For improved control, consider using the viscous fluid injection system when injecting BSS into the subretinal space. Titrate the injection pressure to provide a steady drip of BSS when the foot pedal is fully engaged. This may be titrated under the microscope prior to entering the eye. A steady dripping of BSS rather than a stream is desired. Depending on the vitrectomy machine the injection pressure may vary (For Constellation, (Alcon Laboratories) this pressure is around 12-16 mm Hg).
3. Inject slowly to avoid the formation of macular hole.
4. Expect that the BSS will not coalesce and unfurl the fold until fluid-air exchange is completed. Consider waiting several minutes under air and/or gently shaking the eye to encourage unfurling of the fold.
5. While in this case SF6 gas was used, it is very possible that air tamponade may have been sufficient as the subretinal BSS tends to be resorbed within a few days, depending on the volume.
6. Post-operative prone positioning should theoretically lower the chances of recurrent fold formation.
Subretinal Perfluorocarbon
A 35-year-old man was referred 1 week after vitrectomy surgery for macula off retinal detachment. A large subfoveal perfluorocarbon (PFO) bubble was present with a poor visual acuity.
Considering the toxicity of subretinal PFO, the decision was made to remove the subretinal bubble. The surgical strategy consisted of inducing an iatrogenic posterior retinal detachment by injecting BSS into the subretinal space and then displacing the subretinal PFO bubble peripherally by injecting PFO over the posterior pole. The peripherally displaced subretinal PFO bubble was then aspirated together with the subretinal BSS through a 40 gauge subretinal needle. This was followed by air/fluid exchange.
To prevent subretinal PFO in retinal detachment surgery, one should avoid allowing PFO level passing the most posterior break. Also, avoid filling the eye with PFO up to the level of the tears when working in the periphery. In case of posterior breaks, these should be completely covered by the PFO. It is important to shorten the duration of PFO presence in the eye and always monitor the meniscus of the PFO bubble with a wide angle viewing system. One should also avoid the accumulation of free moving small bubbles (fish eggs) of PFO around the meniscus of the main bubble. These small bubbles can gain access to the subretinal space through open breaks in the retina. Further, large breaks and traction associated with breaks can lead to the subretinal access of PFO.
Subretinal Perfluorocarbon Injection during En Bloc Perfluorodissection
This video demonstrates perfluorocarbon dissection in a patient with diabetic traction retinal detachment. Core vitrectomy was performed and an opening was made in the mid peripheral hyaloid. Perfluorocarbon was injected very slowly between the posterior hyaloid and the retina to generate space and dissect the fibrotic tissue tissues (“En Bloc Perfluorodissection”). However, perfluorocarbon gained access to the subretinal space and an iatrogenic retinal detachment was formed. At this point more perfluorocarbon was injected in the posterior pole and the subretinal perfluorocarbon was drained with a soft tip cannula through a peripherally made drainage retinotomy site.
To avoid this complication one may inject perfluorocarbon very slowly without causing undue pressure. In the presence of severe traction detachment, additional instruments may be used i.e. picks, forceps, and scissors to relieve traction prior to perfluorocarbon injection.
To drain the subretinal perfluorocarbon one may make a peripheral drainage retinotomy site. Then inject perfluorocarbon gently over the optic nerve to push the subretinal perfluorocarbon peripherally and flatten the posterior pole while simultaneously aspirating the subretinal perfluorocarbon with a soft tip cannula through the peripheral retinotomy.
Intraocular Foreign Body Dislodged on the Macula
The patient presented with traumatic cataract and intraocular foreign body (IOFB). Cataract surgery was performed followed by vitrectomy. During the vitrectomy the IOFB was dislodged on the macula. Perfluoron was injected and the intraocular foreign body was grasped with a magnet and extracted with forceps. The posterior hyaloid was detached and peripheral shaving of the vitreous base was performed.
48 hours postoperatively the OCT indicated a small scar without affecting the center of the macula. 4 weeks later a macular pucker has developed. Vitrectomy was performed and the ILM was peeled using brilliant blue.
Suprachoroidal Hemorrhage
Suprachoroidal hemorrhage is a severe and devastating complication of vitreoretinal surgery. Trans-scleral drainage of liquefied blood is performed while maintaining relatively high intra-ocular pressure with a 25G cannula inserted in the anterior chamber. After partial drainage and better visualization, trochars were inserted into the pars plana. Additional suprachoroidal hemorrhage was drained through the trochars. Pars plana vitrectomy was performed. Intravitreal perfluorocarbon injection pushed the choroidal hemorrhage peripherally allowing further drainage through the anterior sclerotomies. Silicone oil tamponade was used at the conclusion of the surgery.
Hemorrhagic Choroidal Detachment after “One Stitch” Vitrectomy Surgery
A 35-year-old diabetic patient presented with a history of uneventful “one stitch” vitrectomy surgery for macular traction associated with diabetic macular edema. 24 hours after surgery patient has developed a massive exudative/hemorrhagic choroidal detachment with a retinal tear at the superotemporal sclerotomy site. Patient was treated with laser since the break was supported by the choroidals buckling effect. Few days later the patient developed a retinal detachment with persistent large hemorrhagic choroidals nasally and temporally.
It was decided to proceed with a repeat surgery 7 days after the original vitrectomy. Infusion cannula was inserted into the anterior chamber to avoid supra-choroidal infusion. External choroidal drainage was performed while using internal perfluoron tamponade. Peripheral retina was treated with endolaser and the eye was filled with silicone oil. Silicone oil was removed 3 month after the second surgery and the retina remained attached.
Dislocated Phakic IOL
A 28-year-old patient presented with a history of previous implantation of a phakic refractive lens in the right eye. Six months after implantation, the implanted lens dislocated into the vitreous cavity. Pars plana vitrectomy was performed to extract the lens. This was particularly difficult due to the size of the lens and the phakic status of the patient. The usage of a chandelier light enabled bimanual grasping and cutting the lens in the vitreous cavity. The smaller lens fragments were removed via the pars plana sclerotomies.
Dislocation of the Tip of the Soft Tip Cannula
Patient underwent pars plana vitrectomy for proliferative diabetic retinopathy. During the injection of triamcinolone acetonide into the eye (to better visualize the vitreous), the tip of the silicone tipped cannula separated from the cannula and was dislodged into the vitreous cavity. The surgery was continued and the dislocated tip was left alone. Towards the end of the surgery; however, the silicone tip moved between the lens and pars plana. This was a challenging situation since any manipulation could lead to either cataract formation or iatrogenic peripheral breaks. Using the vitreous cutter at the suction mode, the silicone tip was re-located into the posterior pole. At this point, it was decided to remove the cannula tip with forceps; however, the flow of the fluid inside the eye guided the cannula tip into the trochar and outside the eye.
It is important to remember that the soft tip cannula is designed for aspiration of fluid rather than injection of fluid into the eye. Further, always examine the tip of the soft tip cannula when exiting the eye to assure that it is not dislodged inside the eye.
Iatrogenic Peripheral Retinal Breaks during IOFB Extraction
Peripheral retinal tears are not an unusual finding in patients with intraocular foreign body (IOFB) injury. These patients are generally young and present with an attached hyaloid. During the removal of the foreign body the vitreous manipulation and traction may lead to peripheral tears.
It is important to perform a thorough vitrectomy prior to IOFB removal. At the conclusion of the surgery the peripheral retina must be examined very carefully. Any suspicious are must be treated with retinopexy i.e. endolaser and adequate tamponade.
Peri-silicone Proliferation
Peri-silicone proliferation is a subtype of epiretinal proliferation that occurs in eyes filled with silicone oil. In the eye, silicone oil floats over a meniscus of fluid rich in cytokines that could stimulate a severe inferior proliferation. Peri-silicone proliferation is observed in more tan 50% of these patients, and may lead to proliferative vitreoretinopathy (PVR) and recurrent inferior retinal detachment requiring repeat vitreous surgery.
A case of peri-silicone proliferation associated with retinal detachment involving the posterior pole is presented. Three-port 23-gauge pars plana vitrectomy with two aspirating syringes was performed to remove the silicone oil. Trypan blue staining was used to visualize the epiretinal proliferation, followed by Perfluorocarbon injection to reattach and stabilize the detached retina. All the scar tissue was peeled from the retinal surface with forceps.
Excellent visualization of the peri-silicone proliferation with trypan blue staining and careful and meticulous peeling ensures the complete removal of all the scar tissue while avoiding iatrogenic retinal breaks, reducing the risk of recurrent PVR.
Miragel Buckle Removal
An 83-year-old patient presented with a superior orbital mass and a history of retinal surgery 16 years ago. The proptosis had increased in the past 6 months causing diplopia. It was decided to remove the expanding Miragel buckle.
During surgery, the Miragel implant was gel-like, brittle, and swollen. It measured 14.5×12.4×7.0 mm about two to three times the original width and thickness.
Surgical removal was complicated by a thick, fibrous capsule, which has fixated the swollen buckle element to the tenon’s capsule, limiting the mobility of the globe.
The implant was removed in its entirety as described below:
After opening the conjunctiva and isolating the Miragel implant, it was removed by pushing it out: exerting pressure to it with a blunt instrument rather than grasping it. Using sharp forceps as in the conventional silicone buckle removal would make the removal of the Miragel implant very difficult since forceps would bite through it rather than grasping it leading to its disintegration.
The Miragel implant was associated with a massive periocular fibrosis. During the dissection of this fibrotic tissue, great care was given to avoid any damage to the peri-ocular muscles (blunt dissection). Following the removal of the Miragel implant, the underlying sclera was examined carefully to assure its full integrity and that there were not any areas of perforation. The pressure induced by the expansion of the Miragel implant may lead to scleral thinning and sclera rupture during this type of surgery. It is important to have graft or synthetic tissue available in case of scleral rupture.
Subconjunctival Silicone Oil Removal
A 48-year-old myopic patient presented with chronic pain and redness in the right eye. Patient had a history of 2 sutureless vitrectomies in the past (latter surgery with silicone oil). On exam patient had an elevated intraocular pressure, subconjunctival silicone oil, reduced globe motility, and an inferior retinal detachment with a break at 6 o’clock.
The video demonstrates the removal of subconjunctival pockets of silicone oil.
When silicone is used during vitrectomy surgery, suturing the sclerotomies would prevent the subsequent leakage of oil that can occur immediately after surgery or over time. This is specially the case in patients with high myopia with a thin sclera.