Longitudinal muscle
Circular muscle
Submucosa
Mucosa
(Top) There are 5 layers of the bowel wall. The innermost is the mucosa, the absorptive surface of the gut. The other layers are the submucosa, circular muscle, longitudinal muscle, and serosa.
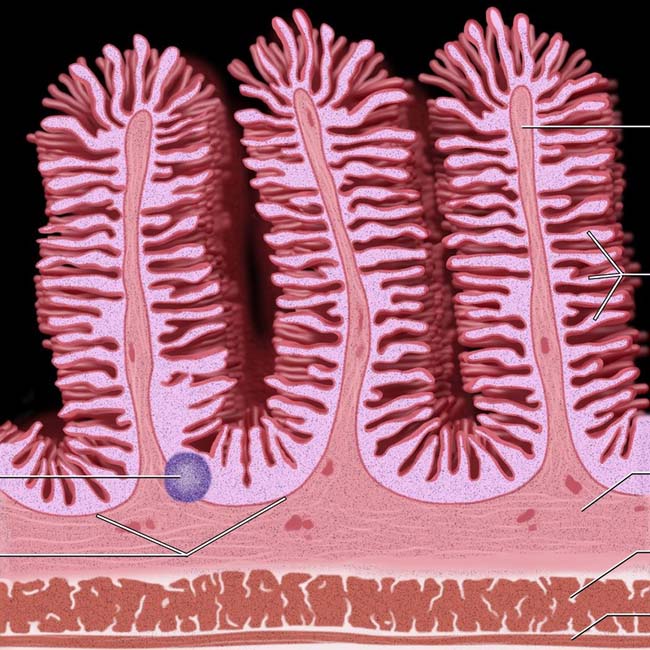
Muscularis mucosa
Circular fold & lamina propria
Villi
Submucosa
Circular muscle
Longitudinal muscle
(Bottom) The mucosal surface of the jejunum is increased by prominent villi, which are finger-like projections of mucosa. The submucosa has a network of capillaries, lymphatics, and a nerve plexus. The jejunum has few small, discrete lymphoid nodules. Although there is no sharp point of transition between the jejunum and ileum, the wall of the ileum becomes thinner and less vascular, with shorter and more widely spaced transverse folds, and more prominent lymphoid follicles.

 , but no ascites or ileus. These findings, along with no clinical evidence for bowel ischemia, correctly suggested benign, medication-induced pneumatosis.
, but no ascites or ileus. These findings, along with no clinical evidence for bowel ischemia, correctly suggested benign, medication-induced pneumatosis.
 within the kidneys.
within the kidneys.
 . This, along with the renal inflammatory or ischemic changes in a young patient, suggested the diagnosis of vasculitis as the underlying disease process, subsequently confirmed by renal biopsy.
. This, along with the renal inflammatory or ischemic changes in a young patient, suggested the diagnosis of vasculitis as the underlying disease process, subsequently confirmed by renal biopsy.
 with the intussusceptum and its mesenteric fat and vessels inside the intussuscipiens.
with the intussusceptum and its mesenteric fat and vessels inside the intussuscipiens.
 , a metastasis in the wall of the intussusceptum.
, a metastasis in the wall of the intussusceptum.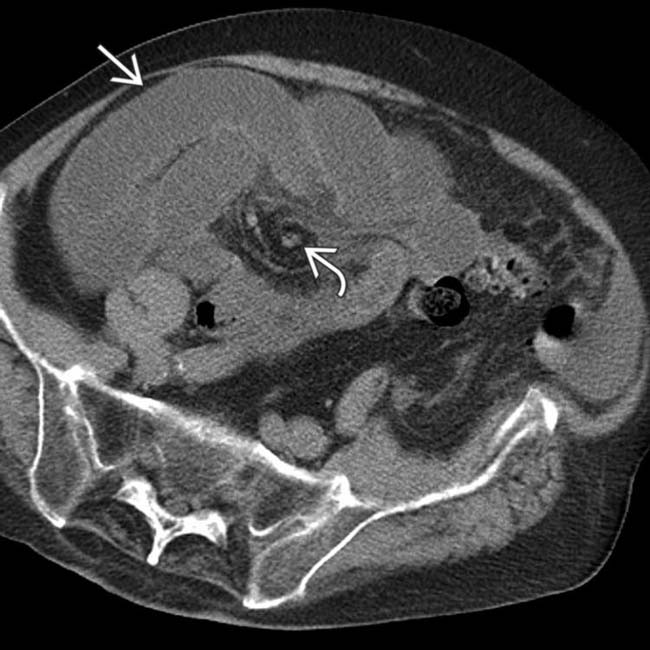
 with twisting and distortion of the mesenteric vessels
with twisting and distortion of the mesenteric vessels  .
.
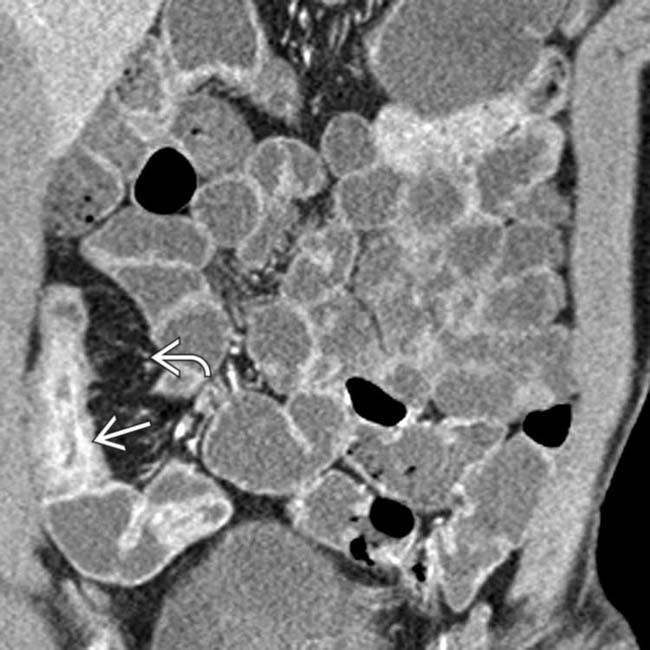
 , arrayed as “balloons on strings” representing the engorged mesenteric vessels
, arrayed as “balloons on strings” representing the engorged mesenteric vessels  , classic findings of a closed-loop SBO. Interloop ascites
, classic findings of a closed-loop SBO. Interloop ascites  , mesenteric edema and poor definition of the SB walls suggest ischemia. Closed-loop SBO with infarcted bowel was confirmed at surgery.
, mesenteric edema and poor definition of the SB walls suggest ischemia. Closed-loop SBO with infarcted bowel was confirmed at surgery.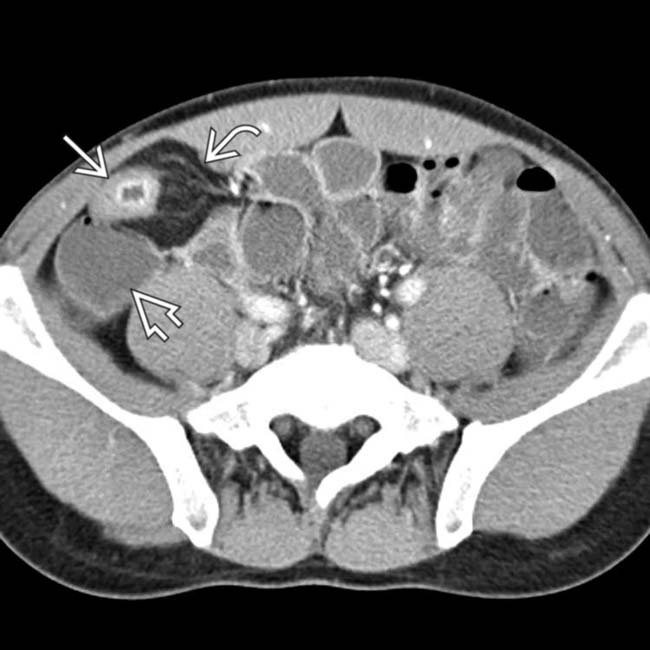
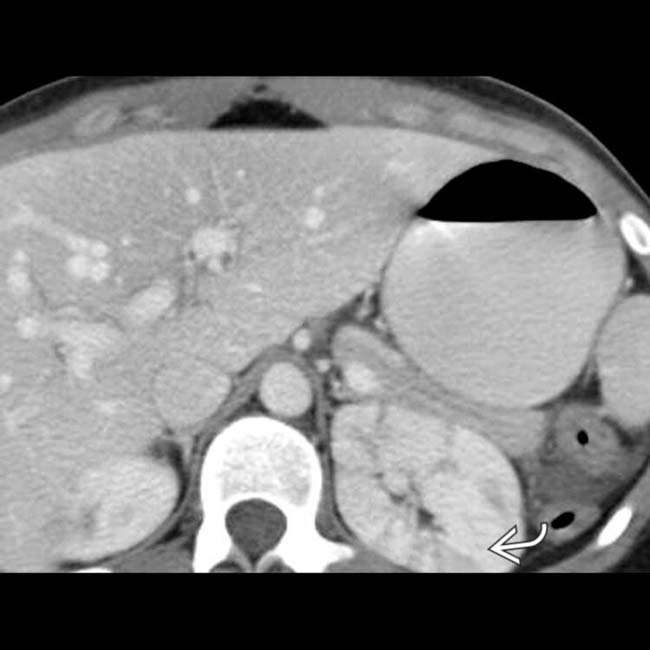
 with water density contrast medium. The SB is normal except for the terminal ileum
with water density contrast medium. The SB is normal except for the terminal ileum  which shows luminal narrowing, wall thickening, and mucosal hyperenhancement. Mesenteric vascular engorgement is present
which shows luminal narrowing, wall thickening, and mucosal hyperenhancement. Mesenteric vascular engorgement is present  .
.
 and local fibrofatty proliferation
and local fibrofatty proliferation  , typical features of Crohn disease.
, typical features of Crohn disease.
 arising from the ileum. Within the affected segment of bowel, there are high density foci of extravasated contrast material
arising from the ileum. Within the affected segment of bowel, there are high density foci of extravasated contrast material  indicating active bleeding from the mass.
indicating active bleeding from the mass.
 having an endoluminal and exophytic component, typical of a GI stromal tumor, confirmed at surgery.
having an endoluminal and exophytic component, typical of a GI stromal tumor, confirmed at surgery.

