(Left) Graphic shows the ventral pancreatic anlagen developing as an outpouching of the hepatic-biliary diverticulum. As the stomach and duodenum elongate, the ventral pancreas and bile ducts rotate clockwise and posteriorly to fuse with the dorsal pancreas.
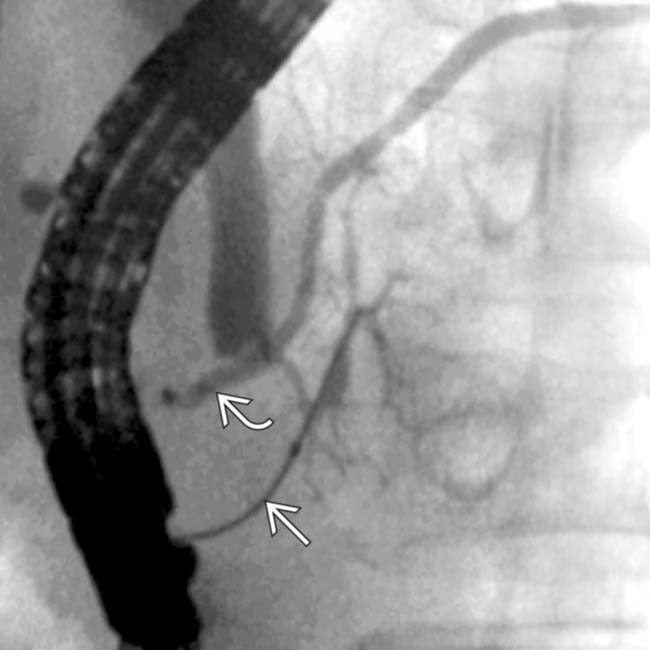
(Right) ERCP of pancreatic divisum shows that the main and accessory pancreatic ducts do not communicate. This results embryologically from failure of fusion of the ducts between the dorsal and ventral pancreatic anlagen.
(Left) Axial CECT shows normal senescent changes within the pancreas . The top image (A) is from a 30-year-old woman and the bottom image (B) is from a 78-year-old man. With aging, the pancreas decreases in size with increased fatty lobulation. Small calcifications and mild ductal dilatation may also be seen.
(Right) Coronal reformatted CECT shows the relationship of the pancreatic head to the 2nd portion of the duodenum .
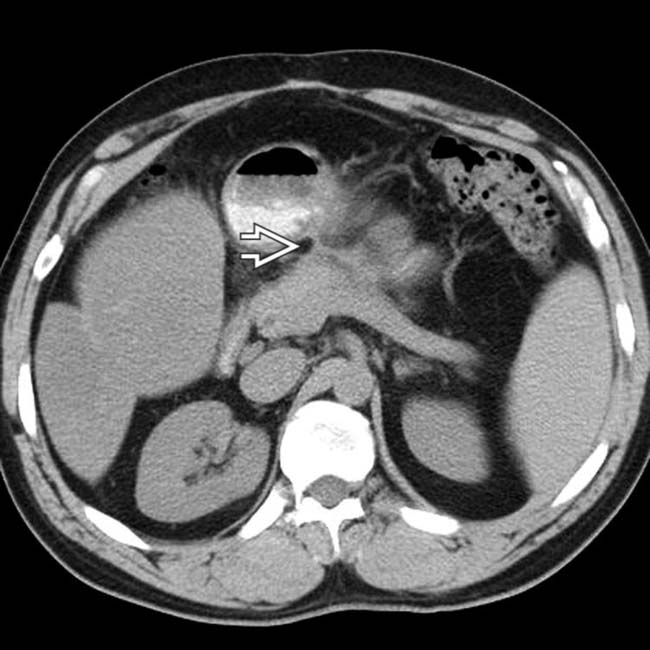
(Left) In this elderly man with painless jaundice, axial CECT shows a hypodense mass in the head of the pancreas and a distended gallbladder .
(Right) Coronal CT reformation in the same case shows the dilated pancreatic duct interrupted as it enters the hypodense mass , a typical presentation of pancreatic ductal carcinoma.
(Left) This 35-year-old man presented with jaundice and weight loss, with axial CECT showing a hypodense mass in the head of the pancreas causing biliary obstruction and dilation of the gallbladder .
(Right) Curved planar reformation of CECT in the same case shows the pancreatic “mass” causing partial obstruction of the bile duct , while the pancreatic duct is only mildly dilated. Further evaluation, including biopsy, confirmed a diagnosis of autoimmune (IgG4-related) pancreatitis.
(Left) In this 81-year-old man with painless jaundice, a curved planar reformatted CECT shows dilation of the common bile duct and pancreatic duct due to a small hypodense ampullary carcinoma .
(Right) Coronal 3D reformatted CT in the same case clearly shows the dilated bile duct , pancreatic duct , and ampullary tumor .
(Left) In this 63-year-old man with intractable peptic ulcers, axial CECT shows a thick-walled, hyperemic stomach .
(Right) Arterial phase CT in the same case shows a subcentimeter mass in the pancreatic head that proved to be a gastrinoma (1 type of pancreatic endocrine tumor) that was responsible for this patient’s Zollinger-Ellison syndrome.
(Left) In this elderly man, axial CECT shows a bulky, hypervascular mass originating from the pancreas with direct invasion of the splenic vein , typical features of a malignant neuroendocrine tumor.
(Right) In this 62-year-old woman with pancreatic metastasis from renal cancer (resected 10 years prior), axial CECT shows surgical absence of the left kidney but no evidence of recurrence in the surgical bed. There is a hypervascular mass with parenchymal atrophy and pancreatic ductal dilation upstream .
(Left) In this 50-year-old man who had a multivisceral organ transplantation, axial CECT shows a pseudoaneurysm of the arterial graft anastomosis that simulates a hypervascular pancreatic mass.
(Right) In this 52-year-old man with cirrhosis and portal vein thrombosis, axial CECT shows a mass of varices in and around the pancreatic head that might be mistaken for a hypervascular tumor of the pancreas.
(Left) In this 45-year-old man, axial T2WI MR shows a retrogastric pseudocyst that displaces the stomach .
(Right) Axial NECT scan in the same case taken 2 weeks later shows spontaneous resolution of the pseudocyst, which has emptied into the stomach through a visible tract . The patient’s clinical symptoms improved at the same time. Pseudocysts, unlike cystic pancreatic neoplasms, usually evolve in size quickly, which may aid in distinction.
(Left) In this 33-year-old woman, axial CECT shows an encapsulated cystic mass within the body-tail of the pancreas. Note the septa dividing it into several noncommunicating cystic spaces, a classic presentation for mucinous cystic neoplasm.
(Right) In this 57-year-old woman, CT shows an encapsulated cystic pancreatic mass that displaces, but does not involve, the pancreatic duct . The mass has a “honeycomb” or “sponge” appearance, characteristic of serous microcystic adenoma.
(Left) In this 21-year-old woman, axial CECT shows a complex cystic mass in the tail of the pancreas, with peripheral rim calcification and solid mural nodularity , typical features of a solid and papillary epithelial neoplasm (SPEN) of the pancreas.
(Right) In this 71-year-old woman, coronal reformatted CT shows a mixed solid and cystic pancreatic mass that proved to be a neuroendocrine tumor.
(Left) In this 44-year-old man with von-Hippel Lindau disease, axial CECT shows a cluster of benign cysts in the pancreatic body and tail as well as simple cysts in both kidneys .
(Right) Another CT section in the same case shows one of several solid enhancing renal masses , representing renal cell carcinoma.
(Left) In this 62-year-old man, axial CECT shows a multiseptate mass that abuts the pancreas, duodenum, and portal vein . The mass is not in the pancreas but is peripancreatic and is a lymphangioma.
(Right) In this woman with cirrhosis, axial CECT shows an “eggshell” calcification in or near the pancreas that might be mistaken for a cystic pancreatic neoplasm. This represents an aneurysmally dilated and thrombosed portal vein varix in a patient with severe cirrhosis and portal hypertension.
(Left) In this elderly woman with pain and steatorrhea, axial CECT shows massive dilation of the pancreatic duct throughout its length with cystic “masses” in communication with the main and side branches .
(Right) MRCP in the same case confirms the dilation of the main duct as well as the side branches . This appearance could be due to chronic pancreatitis, but main and side-branch IPMN was confirmed on endoscopic sonography.
(Left) In this middle-aged alcoholic man, axial CECT shows dilation of the intrahepatic bile ducts .
(Right) A more caudal CT section in the same case shows marked atrophy of the pancreatic parenchyma and dilation of the pancreatic duct , with extensive calcifications within the ducts and parenchyma. No soft tissue mass was seen and all findings were attributed to chronic pancreatitis.
(Left) Coronal curved planar CT reformation shows a sharp transition from normal to abnormal pancreatic duct caused by a small, subtle pancreatic ductal cancer. Multiplanar imaging greatly enhances the ability to evaluate pancreatic masses.
(Right) In this 73-year-old man, a curved planar CT shows dilation of the main pancreatic duct within the body-tail segment, tapering gradually to a normal caliber duct in the neck. ERCP with sampling of the mucinous pancreatic duct contents confirmed main duct IPMN.
(Left) In this 88-year-old woman with no clinical signs of chronic pancreatitis, axial CECT shows multiple focal calcifications within the pancreas that are separate from vascular calcifications. There is no pancreatic ductal dilation and these are considered normal senescent changes.
(Right) Another CT section in the same case shows additional pancreatic calcification that is somewhat larger than usually seen in senescent change of the pancreas, but the patient remained symptom-free.
 and accessory
and accessory  pancreatic ducts do not communicate. This results embryologically from failure of fusion of the ducts between the dorsal and ventral pancreatic anlagen.
pancreatic ducts do not communicate. This results embryologically from failure of fusion of the ducts between the dorsal and ventral pancreatic anlagen.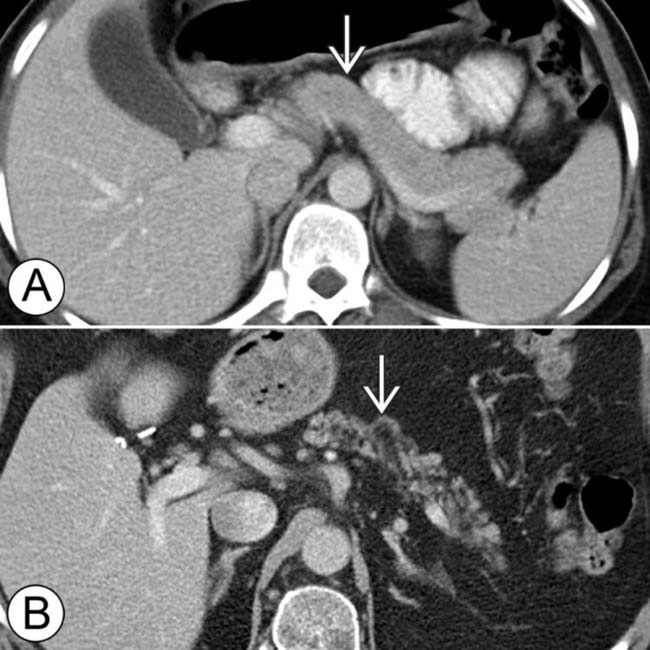
 . The top image (A) is from a 30-year-old woman and the bottom image (B) is from a 78-year-old man. With aging, the pancreas decreases in size with increased fatty lobulation. Small calcifications and mild ductal dilatation may also be seen.
. The top image (A) is from a 30-year-old woman and the bottom image (B) is from a 78-year-old man. With aging, the pancreas decreases in size with increased fatty lobulation. Small calcifications and mild ductal dilatation may also be seen.
 to the 2nd portion of the duodenum
to the 2nd portion of the duodenum  .
.
 in the head of the pancreas and a distended gallbladder
in the head of the pancreas and a distended gallbladder  .
.
 interrupted as it enters the hypodense mass
interrupted as it enters the hypodense mass  , a typical presentation of pancreatic ductal carcinoma.
, a typical presentation of pancreatic ductal carcinoma.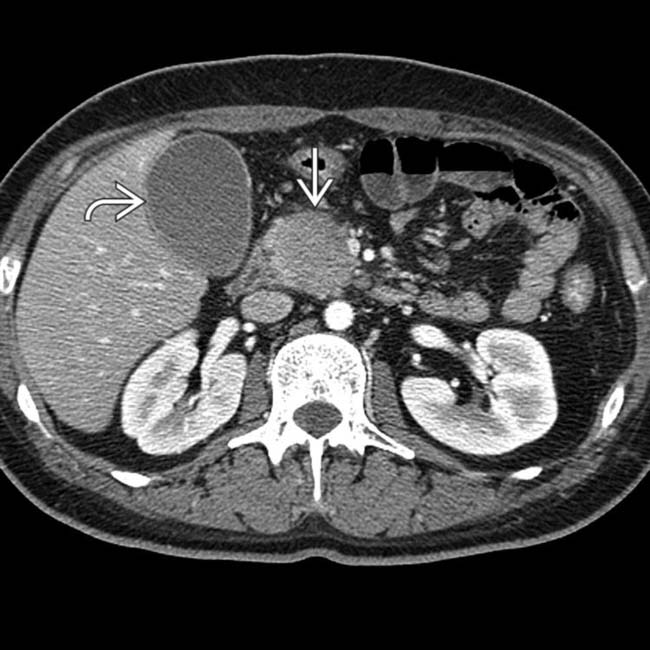
 in the head of the pancreas causing biliary obstruction and dilation of the gallbladder
in the head of the pancreas causing biliary obstruction and dilation of the gallbladder  .
.
 causing partial obstruction of the bile duct
causing partial obstruction of the bile duct  , while the pancreatic duct
, while the pancreatic duct  is only mildly dilated. Further evaluation, including biopsy, confirmed a diagnosis of autoimmune (IgG4-related) pancreatitis.
is only mildly dilated. Further evaluation, including biopsy, confirmed a diagnosis of autoimmune (IgG4-related) pancreatitis.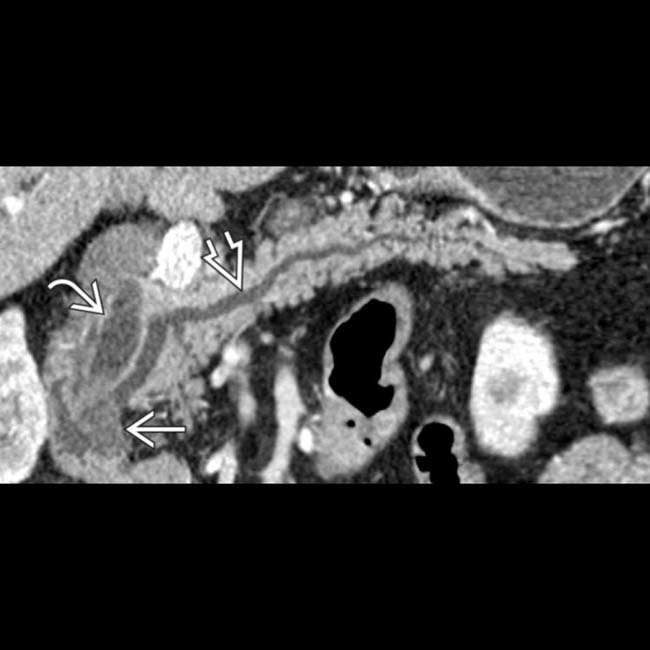
 and pancreatic duct
and pancreatic duct  due to a small hypodense ampullary carcinoma
due to a small hypodense ampullary carcinoma  .
.
 , pancreatic duct
, pancreatic duct  , and ampullary tumor
, and ampullary tumor  .
.
 .
.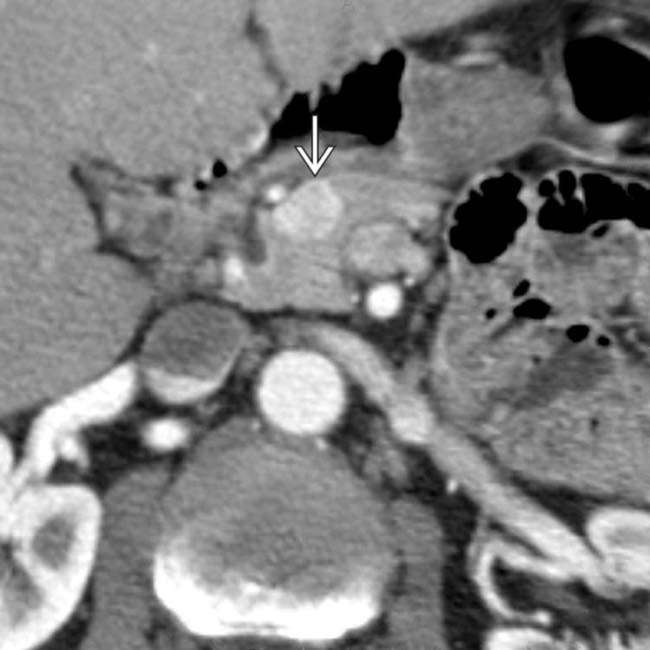
 in the pancreatic head that proved to be a gastrinoma (1 type of pancreatic endocrine tumor) that was responsible for this patient’s Zollinger-Ellison syndrome.
in the pancreatic head that proved to be a gastrinoma (1 type of pancreatic endocrine tumor) that was responsible for this patient’s Zollinger-Ellison syndrome.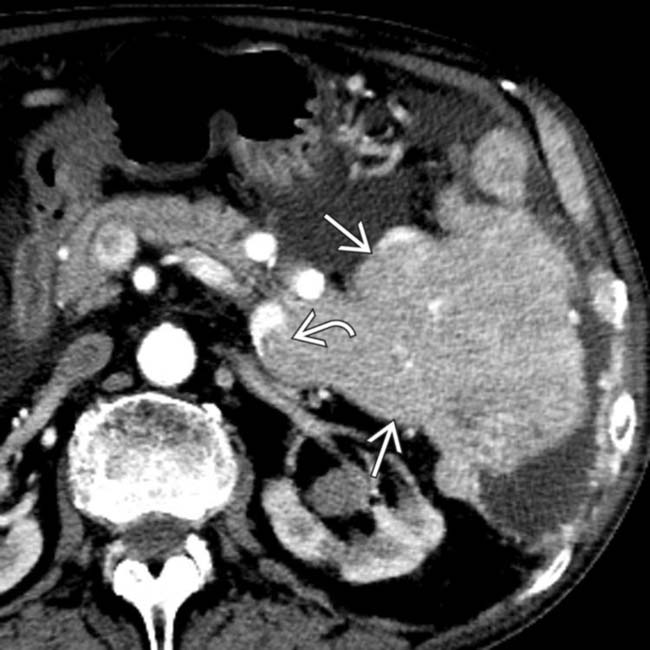
 originating from the pancreas with direct invasion of the splenic vein
originating from the pancreas with direct invasion of the splenic vein  , typical features of a malignant neuroendocrine tumor.
, typical features of a malignant neuroendocrine tumor.
 with parenchymal atrophy and pancreatic ductal dilation upstream
with parenchymal atrophy and pancreatic ductal dilation upstream  .
.
 that simulates a hypervascular pancreatic mass.
that simulates a hypervascular pancreatic mass.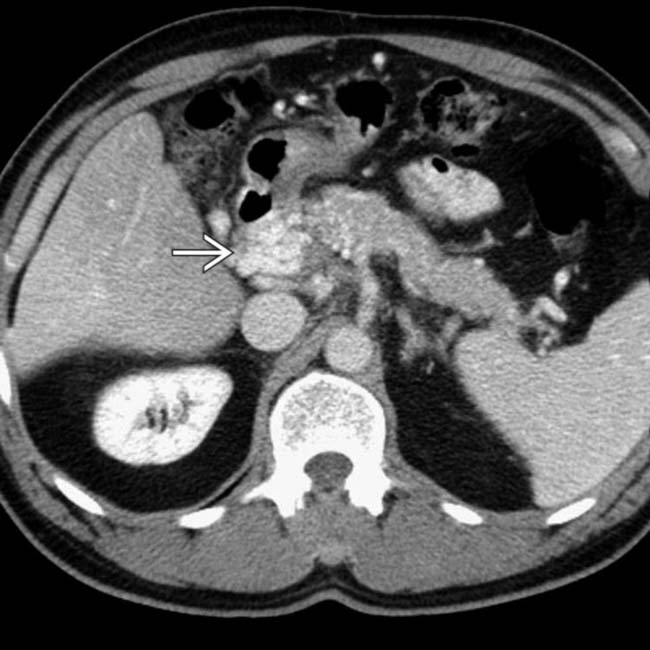
 in and around the pancreatic head that might be mistaken for a hypervascular tumor of the pancreas.
in and around the pancreatic head that might be mistaken for a hypervascular tumor of the pancreas.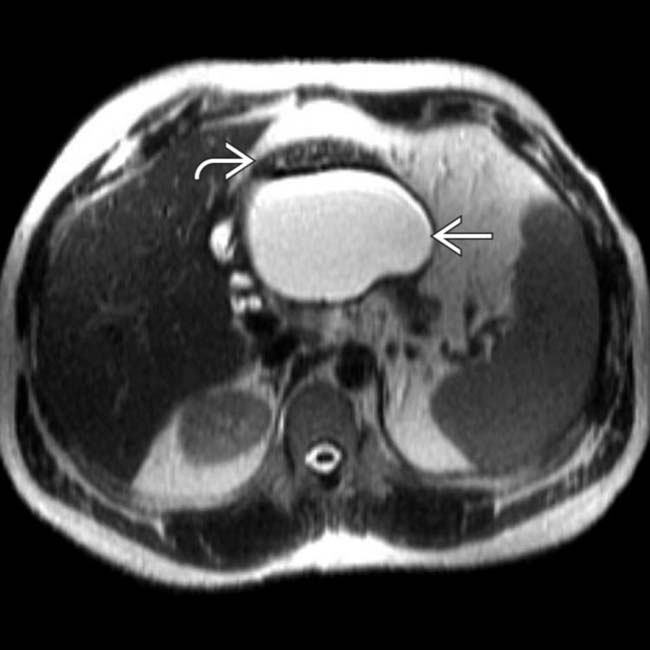
 that displaces the stomach
that displaces the stomach  .
.
 . The patient’s clinical symptoms improved at the same time. Pseudocysts, unlike cystic pancreatic neoplasms, usually evolve in size quickly, which may aid in distinction.
. The patient’s clinical symptoms improved at the same time. Pseudocysts, unlike cystic pancreatic neoplasms, usually evolve in size quickly, which may aid in distinction.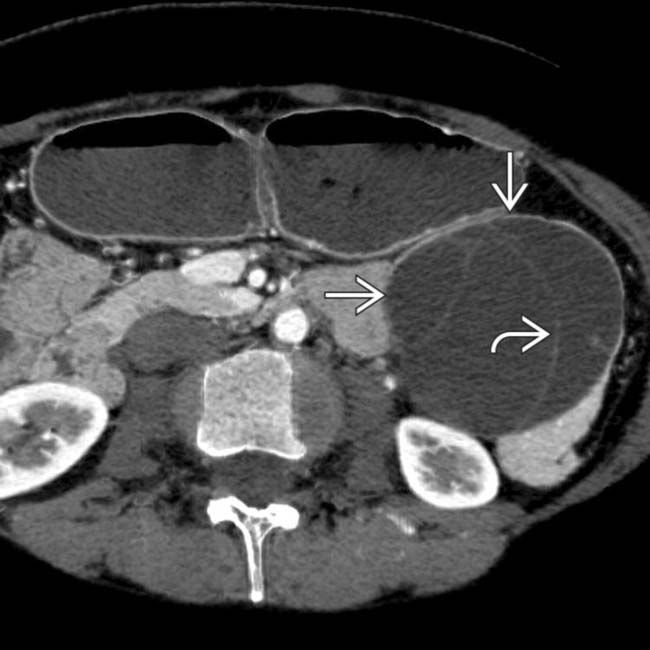
 within the body-tail of the pancreas. Note the septa
within the body-tail of the pancreas. Note the septa  dividing it into several noncommunicating cystic spaces, a classic presentation for mucinous cystic neoplasm.
dividing it into several noncommunicating cystic spaces, a classic presentation for mucinous cystic neoplasm.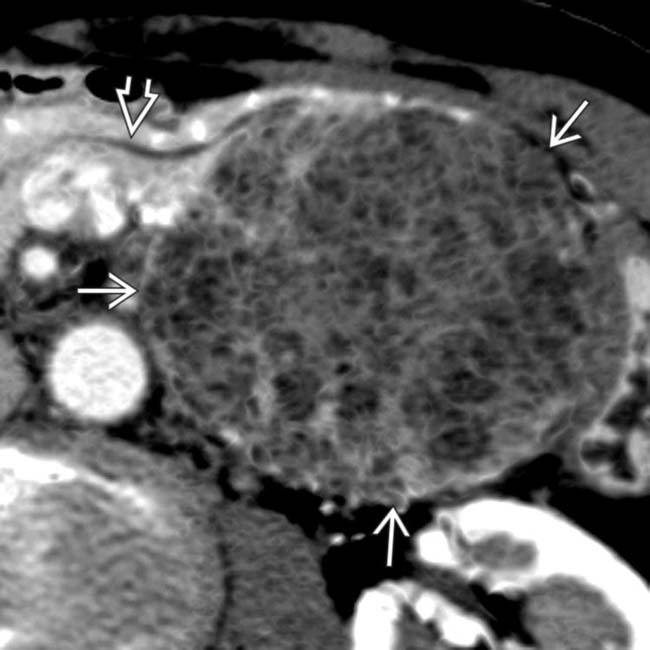
 that displaces, but does not involve, the pancreatic duct
that displaces, but does not involve, the pancreatic duct  . The mass has a “honeycomb” or “sponge” appearance, characteristic of serous microcystic adenoma.
. The mass has a “honeycomb” or “sponge” appearance, characteristic of serous microcystic adenoma.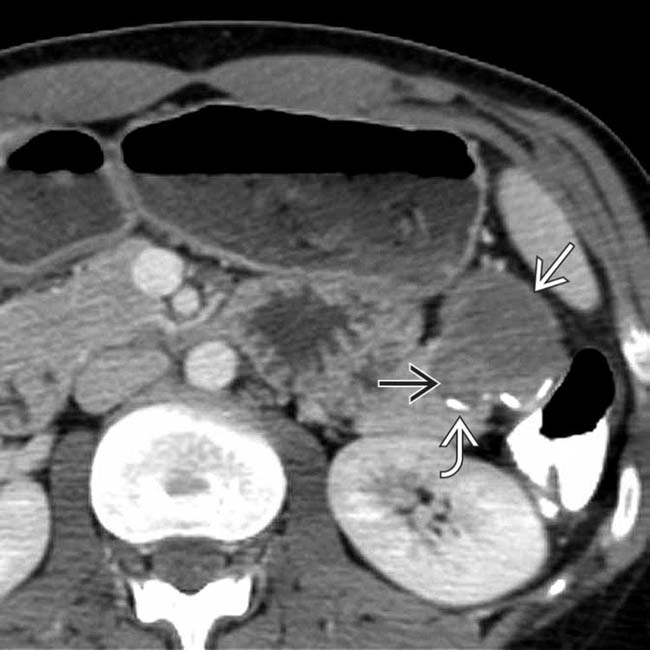
 in the tail of the pancreas, with peripheral rim calcification
in the tail of the pancreas, with peripheral rim calcification  and solid mural nodularity
and solid mural nodularity  , typical features of a solid and papillary epithelial neoplasm (SPEN) of the pancreas.
, typical features of a solid and papillary epithelial neoplasm (SPEN) of the pancreas.
 that proved to be a neuroendocrine tumor.
that proved to be a neuroendocrine tumor.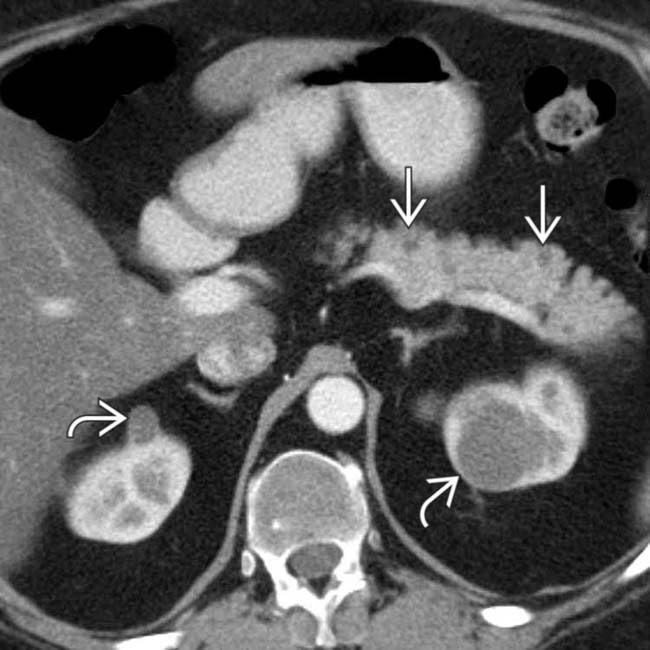
 in the pancreatic body and tail as well as simple cysts in both kidneys
in the pancreatic body and tail as well as simple cysts in both kidneys  .
.
 , representing renal cell carcinoma.
, representing renal cell carcinoma.
 that abuts the pancreas, duodenum, and portal vein
that abuts the pancreas, duodenum, and portal vein  . The mass is not in the pancreas but is peripancreatic and is a lymphangioma.
. The mass is not in the pancreas but is peripancreatic and is a lymphangioma.
 in or near the pancreas that might be mistaken for a cystic pancreatic neoplasm. This represents an aneurysmally dilated and thrombosed portal vein varix in a patient with severe cirrhosis and portal hypertension.
in or near the pancreas that might be mistaken for a cystic pancreatic neoplasm. This represents an aneurysmally dilated and thrombosed portal vein varix in a patient with severe cirrhosis and portal hypertension.
 throughout its length with cystic “masses” in communication with the main and side branches
throughout its length with cystic “masses” in communication with the main and side branches  .
.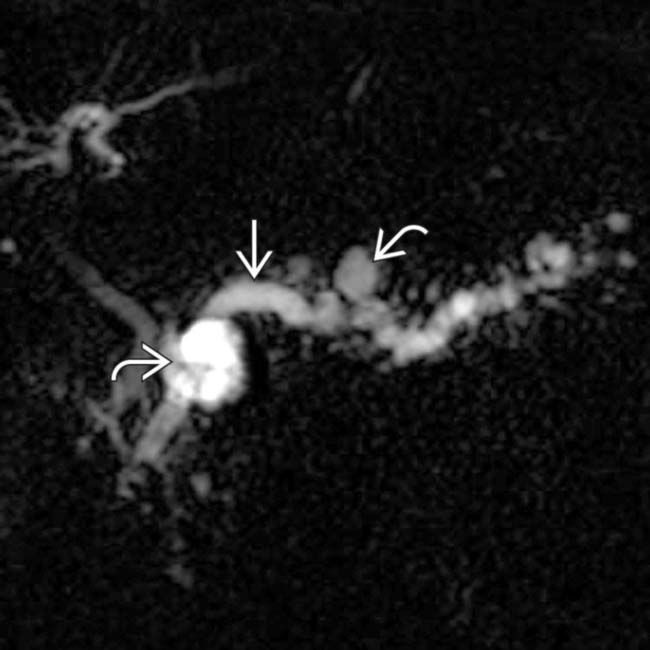
 as well as the side branches
as well as the side branches  . This appearance could be due to chronic pancreatitis, but main and side-branch IPMN was confirmed on endoscopic sonography.
. This appearance could be due to chronic pancreatitis, but main and side-branch IPMN was confirmed on endoscopic sonography.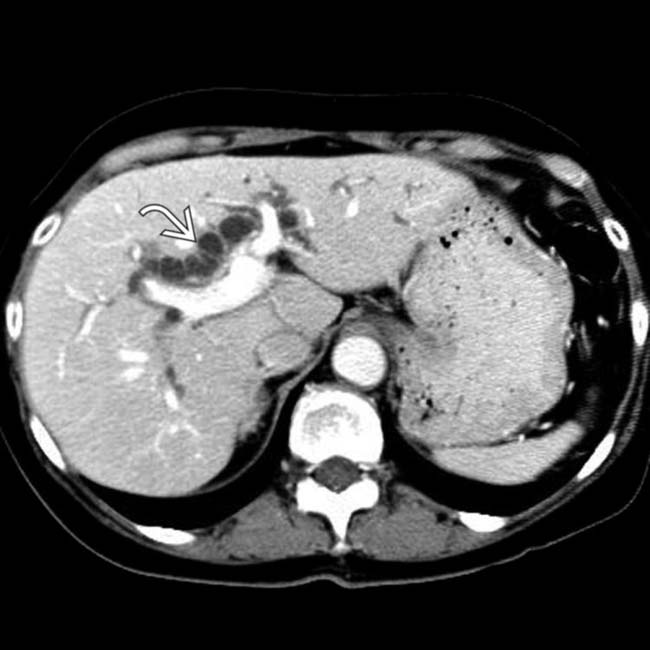
 .
.
 , with extensive calcifications within the ducts and parenchyma. No soft tissue mass was seen and all findings were attributed to chronic pancreatitis.
, with extensive calcifications within the ducts and parenchyma. No soft tissue mass was seen and all findings were attributed to chronic pancreatitis.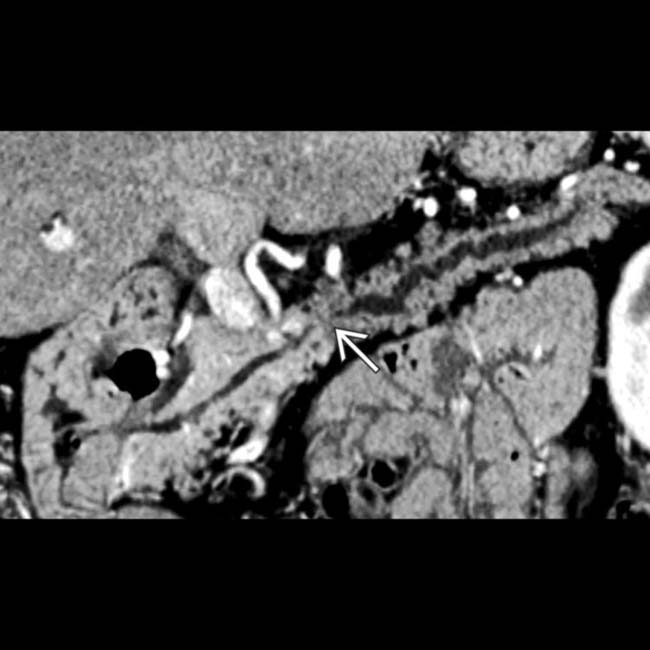
 caused by a small, subtle pancreatic ductal cancer. Multiplanar imaging greatly enhances the ability to evaluate pancreatic masses.
caused by a small, subtle pancreatic ductal cancer. Multiplanar imaging greatly enhances the ability to evaluate pancreatic masses.
 within the body-tail segment, tapering gradually to a normal caliber duct in the neck. ERCP with sampling of the mucinous pancreatic duct contents confirmed main duct IPMN.
within the body-tail segment, tapering gradually to a normal caliber duct in the neck. ERCP with sampling of the mucinous pancreatic duct contents confirmed main duct IPMN.
 within the pancreas that are separate from vascular calcifications. There is no pancreatic ductal dilation and these are considered normal senescent changes.
within the pancreas that are separate from vascular calcifications. There is no pancreatic ductal dilation and these are considered normal senescent changes.
 that is somewhat larger than usually seen in senescent change of the pancreas, but the patient remained symptom-free.
that is somewhat larger than usually seen in senescent change of the pancreas, but the patient remained symptom-free.


