• Pitfalls: Ileus plus ascites, and recent bowel surgery mimic SBO on plain films
CT can be used to resolve issue if necessary
(Left) Supine abdominal radiograph in an 88-year-old man with abdominal distension and hypokalemia from diuretic use shows proportional dilation of the large and small bowel with no clear transition point. The ileus resolved with electrolyte replacement.
(Right) Supine radiograph in a 90-year-old woman with abdominal distension and pain following a hip “pinning” shows gaseous dilation of the colon and the small bowel in a uniform pattern with no point of transition.
(Left) This 52-year-old woman has cirrhosis with increasing abdominal distention and nausea. A supine abdominal film, requested to evaluate possible SBO, shows dilated transverse colon and small bowel , but no gas in other colon segments. Ascites fills the pelvis and paracolic gutters.
(Right) CT in the same patient shows ascites and fluid-distended bowel . Gas fills only a portion of the nondependent bowel, while the dependent SB & colon are fluid-filled & less dilated. This may be misinterpreted as SB obstruction.
TERMINOLOGY
Synonyms
• Adynamic ileus
Definitions
• Proportional gaseous dilatation of large and small bowel (SB) due to lack of intestinal peristalsis, not mechanical obstruction
IMAGING
General Features
• Best diagnostic clue
Proportional dilatation of large and small intestine on plain films with no transition point
• Location
Large and small bowel
• Size
Small bowel > 3 cm
Imaging Recommendations
• Best imaging tool
Plain abdominal radiography, including supine and upright or decubitus views
Multiplanar CT is more accurate with fewer imaging pitfalls
• Protocol advice
Oral contrast may not be tolerated and is rarely necessary for CT
Radiographic Findings
• Radiography
Symmetric dilatation of large and small bowel
– SB diameter > 3 cm (larger than on CT measurements due to magnification on plain radiography)
Air-fluid levels on upright and decubitus films
Pitfall: Ileus plus ascites mimics small bowel obstruction (SBO)
– Gas collects mostly in mesenteric bowel (SB, transverse, and sigmoid colon)
– Retroperitoneal colon segments remain mostly gas-free, invisible on supine films
– CT can easily resolve this, showing generalized dilation of SB and colon without transition point
Recent bowel surgery; plain film findings mimic SBO
– SB will be dilated to point of bowel incision
– This can be a form of ileus and usually resolves spontaneously
Fluoroscopic Findings
• Upper GI
Delayed transit of contrast through small bowel
No mechanical obstruction or transition to collapsed SB
• Contrast enema
No colonic obstruction
Contrast flows to ileocecal valve without difficulty
CT Findings
• Dilated large and small bowel
SB diameter > 2.5 cm
DIFFERENTIAL DIAGNOSIS
Small Bowel or Colonic Obstruction
• Bowel dilated upstream from transition point, obstructing lesion
• Small bowel feces sign found just proximal to point of obstruction
• Etiology may be evident
Inguinal or internal hernia, intussusception, intrinsic or extrinsic masses
• Intraluminal etiologies
Gallstone ileus, foreign body
• Closed-loop obstruction suggested with certain findings









 of the large and small bowel with no clear transition point. The ileus resolved with electrolyte replacement.
of the large and small bowel with no clear transition point. The ileus resolved with electrolyte replacement.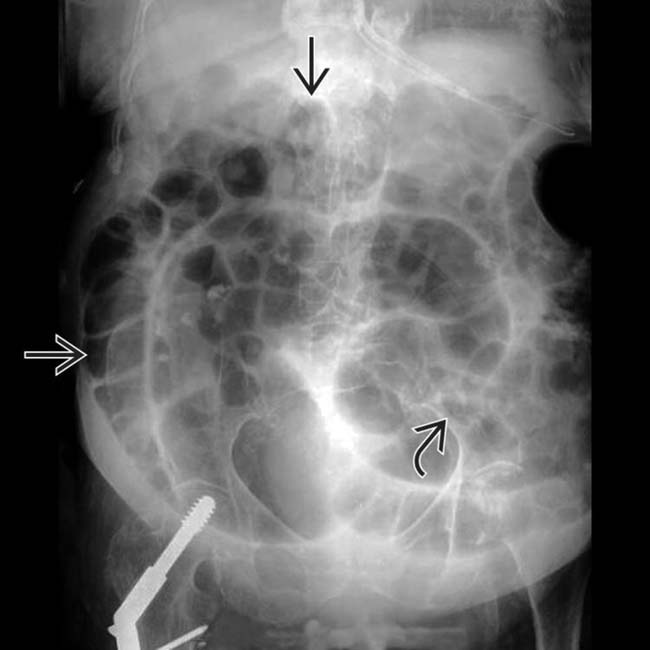
 and the small bowel
and the small bowel  in a uniform pattern with no point of transition.
in a uniform pattern with no point of transition.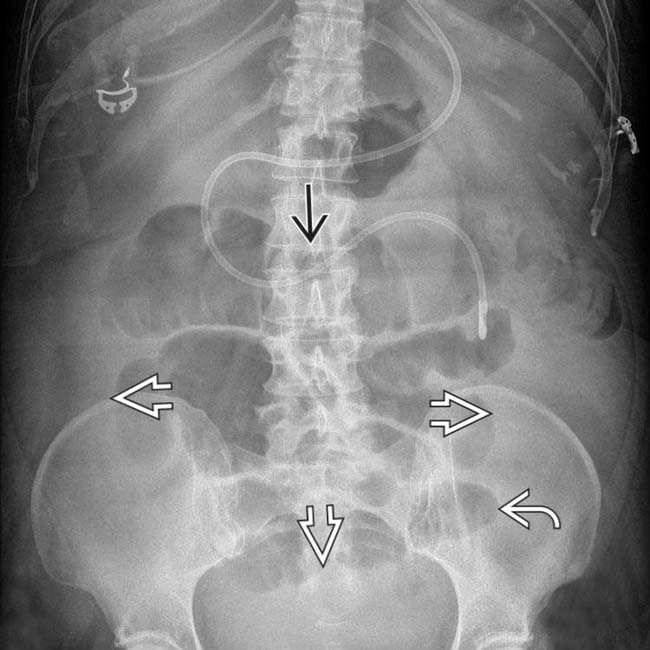
 and small bowel
and small bowel  , but no gas in other colon segments. Ascites
, but no gas in other colon segments. Ascites  fills the pelvis and paracolic gutters.
fills the pelvis and paracolic gutters.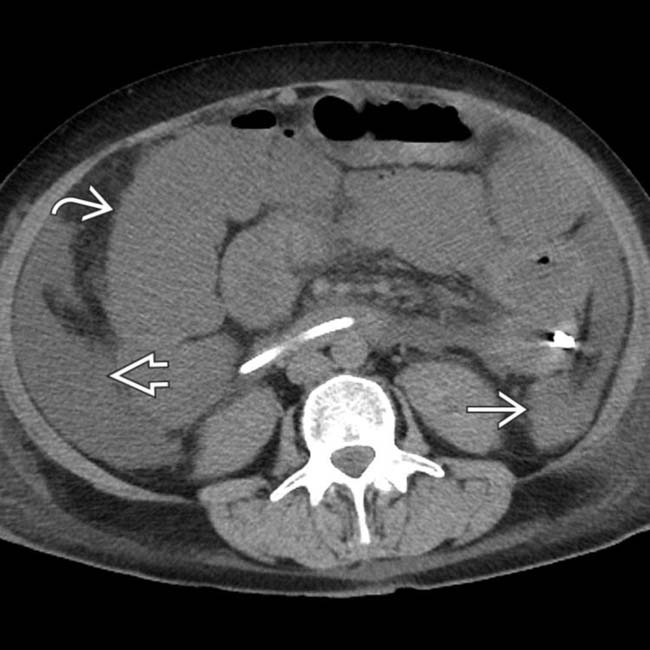
 and fluid-distended bowel
and fluid-distended bowel  . Gas fills only a portion of the nondependent bowel, while the dependent SB & colon
. Gas fills only a portion of the nondependent bowel, while the dependent SB & colon  are fluid-filled & less dilated. This may be misinterpreted as SB obstruction.
are fluid-filled & less dilated. This may be misinterpreted as SB obstruction.













































