[level-membership-for-critical-care-medicine-category]
Chapter 41 Hypertension
1 What are the hemodynamic determinants of blood pressure (BP)?
Arterial BP is the product of cardiac output (CO) and systemic vascular resistance (SVR).

3 What are the target organs affected by hypertensive crisis?




9 Outline the typical long-term antihypertensive regimen after successful treatment of malignant hypertension or hypertensive crisisss
10 What is the appropriate short-term treatment for hypertension in a patient with pheochromocytoma?
13 Why is BP elevated in patients with CVA?

 Failure of autoregulation of cerebral blood flow and response to increased intracranial pressure (ICP)
Failure of autoregulation of cerebral blood flow and response to increased intracranial pressure (ICP)

14 How should hypertension be treated in patients with CVA?




The consensus guidelines on treatment of intracerebral bleeding:




15 Describe the short-term treatment of hypertension in patients with ischemic heart disease and ongoing angina
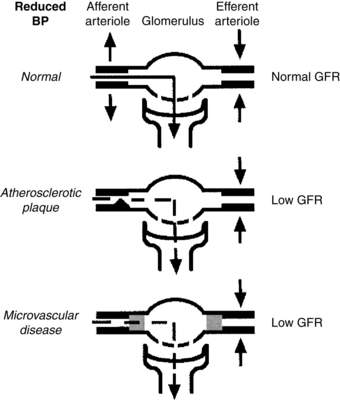
19 Why does lowering of BP potentially result in a decline in glomerular filtration rate (GFR) in severe hypertension?
Normally, GFR is maintained despite decreases in BP by compensatory increases in efferent arteriolar tone (Fig. 41-1) Two major causes exist of loss of GFR after reduction of BP in the setting of severe hypertension:


20 When should an evaluation for secondary hypertension be considered?
 At initial presentation of malignant hypertension (especially if the patient is white, younger than 30 years, or older than 50 years of age)
At initial presentation of malignant hypertension (especially if the patient is white, younger than 30 years, or older than 50 years of age)
 When rapid onset of severe hypertension occurs within less than 5 years
When rapid onset of severe hypertension occurs within less than 5 years
 When an increase in serum creatinine level occurs after the initiation of ACE inhibitor treatment
When an increase in serum creatinine level occurs after the initiation of ACE inhibitor treatment

21 What are the important causes of secondary hypertension?
Secondary hypertension accounts for 5% of cases of hypertension.
 Renal: renovascular disease, renal parenchymal disease, polycystic kidney disease, Liddle syndrome, syndrome of apparent mineralocorticoid excess, hypercalcemia
Renal: renovascular disease, renal parenchymal disease, polycystic kidney disease, Liddle syndrome, syndrome of apparent mineralocorticoid excess, hypercalcemia


 Neurogenic: increased intracranial pressure, spinal cord section
Neurogenic: increased intracranial pressure, spinal cord section
 Miscellaneous: coarctation of aorta, obstructive sleep apnea, polycythemia vera
Miscellaneous: coarctation of aorta, obstructive sleep apnea, polycythemia vera
22 What are the causes of primary aldosteronism, and how should they be distinguished?
Key Points Hypertension
1. Hypertensive crisis (or hypertensive emergency) is the turning point in the course of hypertension when the immediate management of elevated BP plays a decisive role in limiting or preventing target organ damage.
2. Hypertensive crises can damage four main target organ systems: eye, brain, heart, and kidney.
3. The short-term treatment of choice for malignant hypertension is IV sodium nitroprusside.
4. Long-term therapy for malignant hypertension should include a vasodilator such as hydralazine or minoxidil, a β-blocker, and a diuretic agent.
5. Nitroglycerin and β-blockers are the initial agents of choice for patients with ischemic heart disease and angina.
1 Adams H.P.Jr., del Zoppo G., Alberts M.J., et al. Guidelines for the early management of adults with ischemic stroke. Stroke. 2007;5:1655–1711.
2 Kaplan N.M. Pheochromocytoma. In: Kaplan N.M., ed. Clinical Hypertension. 7th ed. Philadelphia: Lippincott Williams & Wilkins; 1998:345–363.
3 Kelleher C.L., Linas S.L. Hypertensive crisis: emergency and urgency. In: Fink M.P., Abraham E., Vincent J.-L., et al. Textbook of Critical Care. 5th ed. Philadelphia: Saunders; 2005:879–888.
4 Kitiyakara C., Guzman N.J. Malignant hypertension and hypertensive emergencies. J Am Soc Nephrol. 1998;9:133–142.
5 Lange R.A., Hillis L.D. Cardiovascular complications of cocaine use. N Engl J Med. 2001;345:351–358.
6 Pohl M.A. Renal artery stenosis, renal vascular hypertension, and ischemic nephropathy. In: Schrier R.W., ed. Diseases of the Kidney. 7th ed. Philadelphia: Lippincott Williams & Wilkins; 2001:1399–1457.
7 Qureshi A.I. Acute hypertensive response in patients with stroke: pathophysiology and management. Circulation. 2008;118:176–187.
8 Qureshi A.I., Ezzeddine M.A., Nasar A., et al. Prevalence of elevated blood pressure in 563,704 adult patients with stroke presenting to the ED in the United States. Am J Emerg Med. 2007;25:32–38.
9 Vaughan C.J., Delanty N. Hypertensive emergencies. Lancet. 2000;356:411–417.
[/level-membership-for-critical-care-medicine-category][not-level-membership-for-critical-care-medicine-category]
Chapter 41 Hypertension
1 What are the hemodynamic determinants of blood pressure (BP)?
Arterial BP is the product of cardiac output (CO) and systemic vascular resistance (SVR).
