HIP
SELECTED MOVEMENTS

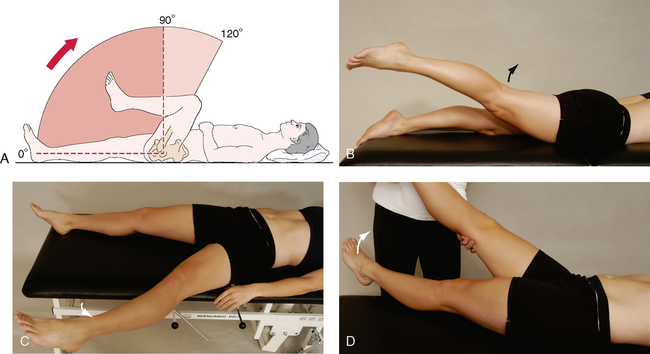
The active movements of the hip are performed with the most painful ones being done last. Some movements are done with the patient supine and some with the patient prone. If the history indicates that repetitive movements, sustained postures, or combined movements have caused symptoms, the examiner should make sure these movements are tested as well. For example, sustained extension of the hip may provoke gluteal pain in the presence of claudication in the common or internal iliac artery.1
• During the movement, if the abdominals are weak, the pelvis will rotate anteriorly. If the hip flexors are weak, the pelvis will rotate posteriorly.
• If sharp groin pain is elicited on flexion and medial rotation (combined movement), the pain may be the result of anterior impingement of the femoral neck against the acetabular rim.2–6
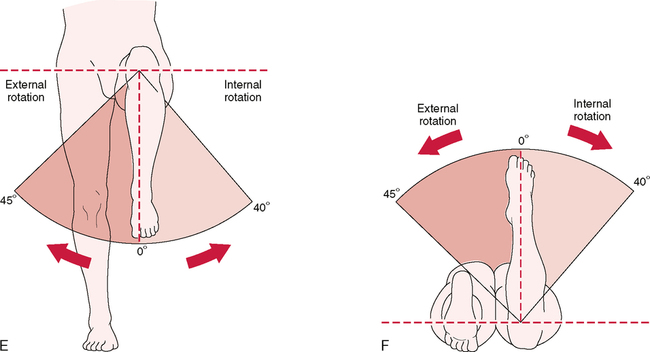
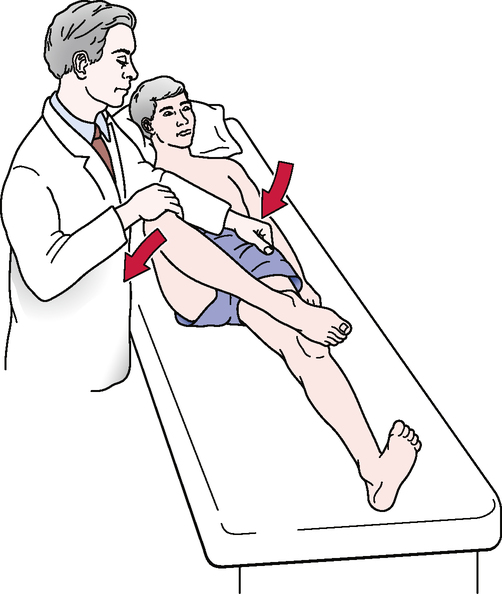
In the supine position, the patient simply rotates the straight leg on a balanced pelvis. Turning the foot or leg outward tests lateral rotation; turning the foot or leg inward tests medial rotation. The examiner can then measure hip rotation by having the patient hold the foot in plantigrade and measuring the angle of the foot to a vertical line from the middle of the heel. In another supine test, the patient is asked to flex both the hip and knee to 90º, as the patient would do when tested in sitting.7 When this method is used, it must be recognized that having the patient rotate the leg outward tests medial rotation, whereas having the patient rotate the leg inward tests lateral rotation.
SPECIAL TESTS FOR HIP PATHOLOGY8–13
Relevant Special Tests
Patrick’s test (flexion, abduction, and external rotation [FABER] or figure-four test)
Anterior labral tear test (flexion, adduction, and internal rotation [FADDIR] test)
Epidemiology and Demographics
• Osteoarthritis affects 10% to 25% of the population over age 55.
• Osteonecrosis can occur in people of any age, but it is most common in people in their 30s, 40s, and 50s.
• In children, the most common cause of hip pain is acute transient synovitis. The incidence of slipped capital femoral epiphysis is about 6.1 per 10,000 in boys and 3 per 10,000 in girls. The incidence of Leg!g-Calvé-Perthes disease is about 1.5 to 5 per 10,000.
• In newborns, the prevalence of developmental dysplasia of the hip (DDH) has been reported in screened populations at rates of 2.5 to 20 per 1000 births; however, it reaches 40 to 90 per 1000 births in some communities.
Mechanism of Injury
PATRICK’S TEST (FLEXION, ABDUCTION, AND EXTERNAL ROTATION [FABER] OR FIGURE-FOUR TEST)14–16 


ANTERIOR LABRAL TEAR TEST (FLEXION, ADDUCTION, AND INTERNAL ROTATION [FADDIR] TEST)20,21 


INDICATIONS OF A POSITIVE TEST
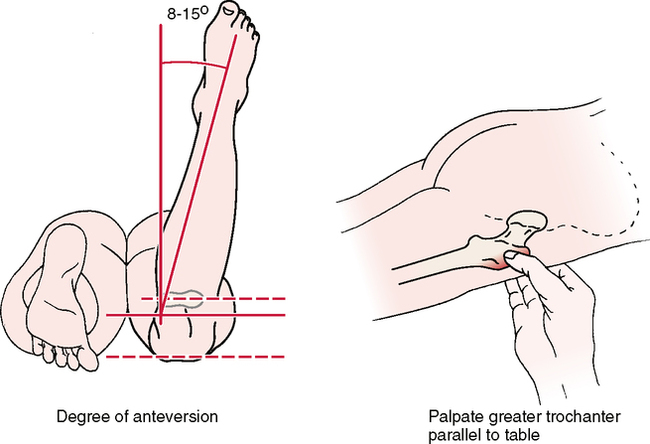
At birth, the mean angle is approximately 30°; in the adult, the mean angle is 8° to 15°.
• Craig’s test has been found to correlate well with radiographic findings (within 4°) in children.
• The test is also called the Ryder method for measuring anteversion or retroversion.
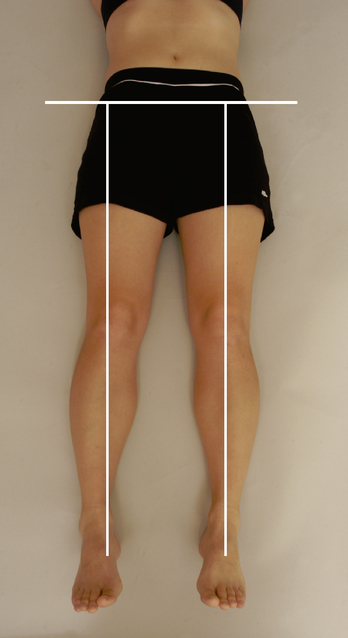
• Anteversion of the hip is measured by the angle made by the femoral neck with the femoral condyles. It is the degree of forward projection of the femoral neck from the coronal plane of the shaft, and it decreases during the growing period.
• Increased anteversion leads to squinting patellae and toeing-in. Excessive anteversion is twice as common in girls as in boys. A common clinical finding of excessive anteversion is excessive medial hip rotation (more than 60°) and decreased lateral rotation in extension. Gelberman et al.29 pointed out, however, that rotation should be viewed both in neutral (as in the Craig’s test) and with 90° of hip flexion, because rotation shows greater variability in flexion. These researchers felt that greater medial rotation than lateral rotation in both positions was a better indicator of increased femoral anteversion.
• With retroversion, the plane of the femoral neck rotates backward in relation to the coronal condylar plane, or the acetabulum itself may be retroverted.
SPECIAL TESTS FOR LEG LENGTH
Relevant Special Tests
Definition
A leg length discrepancy is the difference in the longitudinal length of one leg compared with the other. Leg length discrepancies can be classified in two ways: as actual (true) leg length discrepancies or as apparent (functional) leg length discrepancies. In true leg length discrepancies, the length of one leg is truly different from the length of the other leg. In functional leg length discrepancies, one leg appears different from the other, but when the two legs are measured, the lengths are identical. The apparent length discrepancy can be caused by biomechanical factors (e.g., pelvic rotation) or foot pronation (see Table 9-1).
Epidemiology and Demographics
Freiberg30 studied patients with low back pain and discovered that those with a leg length discrepancy greater than 15 mm were five times more likely to have low back pain. Hip and sciatic pain occurred in the longer leg 78% of the time. In patients with leg length discrepancies greater than 3 cm, an asymmetrical lateral side bend of the spine occurs on the side of the longer leg. This results in abnormal loading mechanics of the spine. Leg length discrepancies of this magnitude are present in 40% of the general population.31
ten Brinke et al.31 reported that in 64 (62%) of 104 patients with a leg length discrepancy of 1 mm or more, the back pain radiated into the shorter leg.
Relevant Signs and Symptoms
• Leg length differences themselves are not usually painful.
• Difference is clinically relevant as a contributing cause of symptoms and pathological conditions in other regions, such as the lumbar spine, pelvis, sacroiliac joint, or lower extremity.
• An objective examination of any of these regions should include an examination of leg length.
Mechanism of Injury

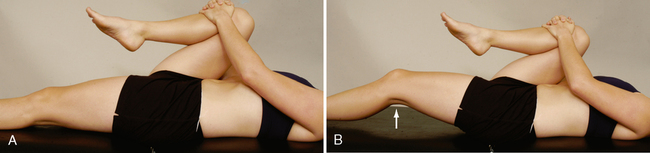
WEBER-BARSTOW MANEUVER (VISUAL METHOD)38 

The patient lies supine with the hips and knees flexed and the feet flat on the table (crook lying).
INDICATIONS OF A POSITIVE TEST
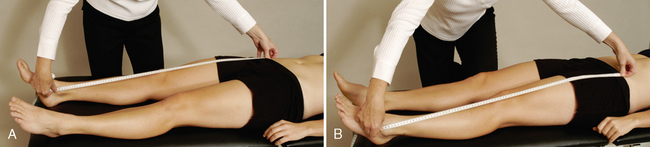
• From the iliac crest to the greater trochanter of the femur (for coxa vara or coxa valga). The neck-shaft angle of the femur normally is 150° to 160° at birth and decreases to 120° to 135° in the adult. In an adult, if this angle is less than 120°, the condition is known as coxa vara; if it is more than 135°, it is known as coxa valga.
• From the greater trochanter of the femur to the knee joint line on the lateral aspect (for femoral shaft shortening).
• From the knee joint line on the medial side to the medial malleolus (for tibial shaft shortening).
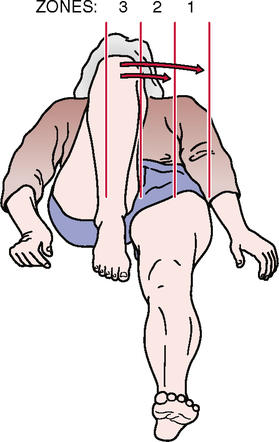
• The femoral lengths can be compared by having the patient lie supine with the hips and knees flexed to 90° (crook lying). If one femur is longer than the other, its height will be higher.
• The relative length of the tibia may also be examined with the patient lying prone. The examiner places the thumbs transversely across the soles of the feet just in front of the heels. The knees are flexed 90°, and the relative heights of the thumbs are noted. Care must be taken to ensure that the legs are perpendicular to the examining table.
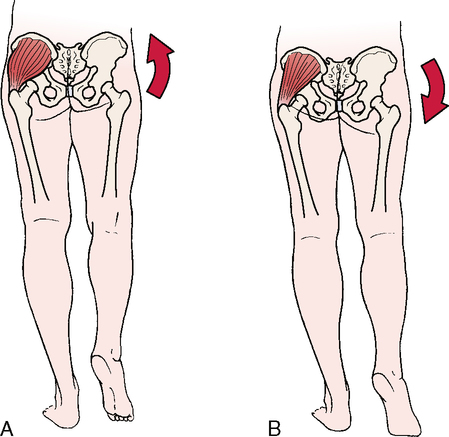
• Apparent or functional shortening of the leg is evident if the patient has a lateral pelvic tilt when the measurement is taken.
• Apparent or functional shortening of the limb is the result of adaptations the patient has made in response to a pathological condition or contracture somewhere in the spine, pelvis, or lower limbs. In reality, there is no structural or anatomical difference in bone lengths.


INDICATIONS OF A POSITIVE TEST
If the asymmetry has been corrected by “correcting” the position of the limb, the leg is structurally normal (i.e., the bones are the proper length); however, abnormal joint mechanics (i.e., a functional deficit) are producing a functional leg length difference (see Table 9-1). Therefore, if the asymmetry is corrected by proper positioning, the test result is positive for a functional leg length difference.
• Functional limb length testing helps the clinician determine whether leg length discrepancies play a role in the patient’s pain and dysfunction when in weight-bearing positions.
• The amount of limb length discrepancy can be gauged by sequentially placing magazines or thin books under the patient’s foot until the pelvis is level.
SPECIAL TESTS FOR MUSCLE TIGHTNESS
Relevant Special Tests
Rectus femoris contracture test (Kendall test)
Ely’s test (tight rectus femoris)
Mechanism of Injury



• If measurements are taken during the test, the examiner must be sure the restriction is in the hip and not the pelvis or lumbar spine. If the leg does not lift off the table but abducts as the other leg is flexed to the chest, this is called the J sign or stroke and indicates a tight iliotibial band on the extended leg side.
• The examiner also may passively hold the flexed limb in position instead of having the patient hold the knee to the chest. When a patient actively holds the knee to the chest, some contraction of the hip flexors may be present and the patient may not be able to fully relax the test limb.
RECTUS FEMORIS CONTRACTURE TEST (KENDALL TEST) 
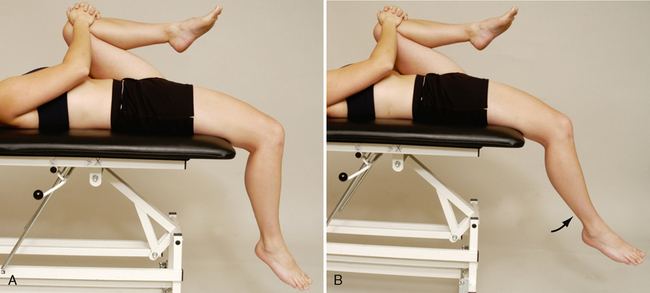
• The examiner may attempt to passively flex the knee to see whether it remains at 90° of its own volition and to test the end feel.
• The examiner should always palpate for muscle tightness when doing any contracture test. If no palpable tightness is noted, the probable cause of restriction is tight joint structures (e.g., the capsule), and the end feel will be different (muscle stretch versus capsular end feel).
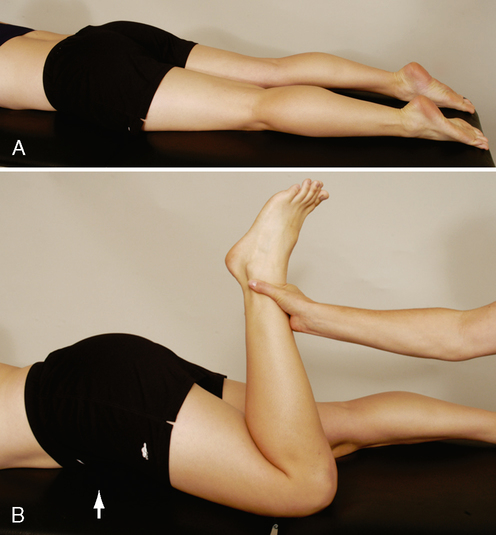
ELY’S TEST (TIGHT RECTUS FEMORIS)41 


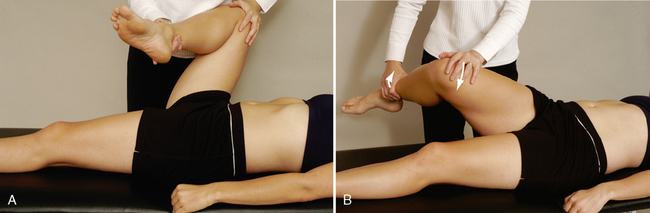
• Ober originally described the test with the knee flexed.42 However, a greater stretch is put on the iliotibial band when doing the test with the knee extended. Also, when the knee is flexed during the test, greater stress is placed on the femoral nerve. If neurological signs (i.e., neurological pain, paresthesia) occur during the test, the examiner should consider a pathological condition affecting the femoral nerve.
• Tenderness over the greater trochanter should lead the examiner to consider trochanteric bursitis.





• Patients, especially children, with adductor spasticity may also be tested by abduction. The patient is supine. The examiner quickly abducts the leg. If a “grab” or “kicking in” of the stretch reflex occurs at less than 30°, the test result is considered positive for adductor spasticity. The test should be repeated with the knee flexed to rule out medial hamstring contracture.

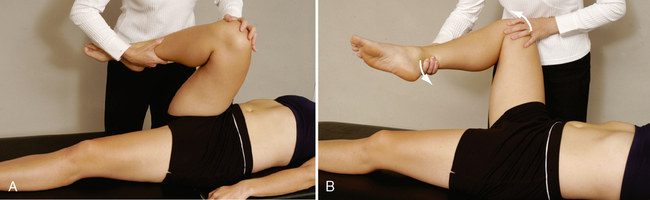
90-90 STRAIGHT LEG RAISE TEST (HAMSTRINGS CONTRACTURE)46–48 
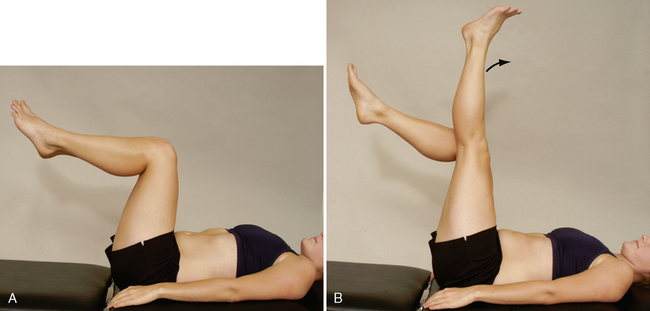
INDICATIONS OF A POSITIVE TEST
For normal flexibility in the hamstrings, knee extension should be within 20° of full extension. Kuo et al.48 called this angle the popliteal angle (the angle between two lines; one line along the shaft of the femur and one line along the line of the tibia). They reported this angle to be 180° from birth to age 2; the angle then decreased to about 155° by age 6 and remained fairly constant after that. If the angle was less than 125°, the hamstrings were considered tight.