[level-membership-for-orthopaedics-category]
Chapter 29 High-Stiffness, Slippage-Resistant Cortical Fixation Has Many Advantages over Intratunnel Fixation
Fixation Stiffness and Slippage: Critical Factors in Restoring Anterior Laxity
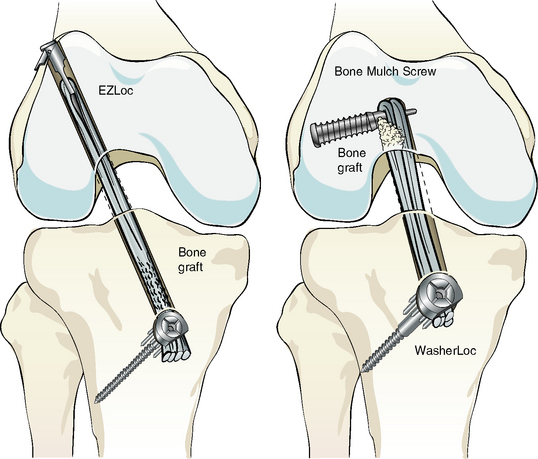
An ACL graft construct is composed of the ACL graft and the two fixation devices at either end (Fig. 29-1). Anterior laxity in the knee of the athlete returning to sport is determined by the stiffness of the ACL graft construct and the length of the ACL graft, not by the strength of the graft and the tension in the graft.1–4
The stiffness of the ACL graft construct determines anterior laxity, the firmness of the Lachman test, and the quality of the “endpoint.” The stiffness of the ACL graft construct is increased more by the use of stiffer fixation devices than by the use of a shorter graft. A short graft with elastic fixation does not restore anterior laxity as well as a longer graft with stiffer fixation.5,6 The concept that shortening the graft increases the stiffness of the ACL graft construct, as proposed by some studies,7–9 is incorrect when high-stiffness, slippage-resistant cortical fixation devices are used.4 The most effective way to construct a stiff ACL graft and restore a firm Lachman test is to use high-stiffness, slippage-resistant cortical fixation devices on both ends of the graft.1,3,5,6
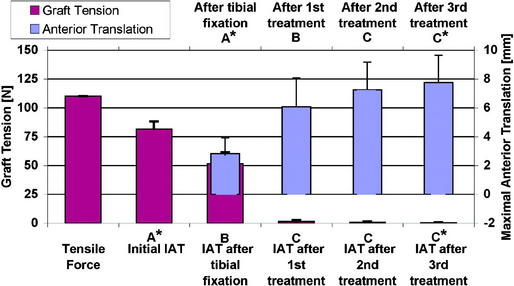
A determinant of anterior laxity that is as equally determinant as the stiffness of the ACL graft construct is maintenance of the length of the ACL graft set at the time of fixation. Maintaining the initial set length of the ACL graft after implantation requires the use of fixation devices that resist slippage during cyclical loading and exercise. Fortunately, there are fixation devices that do resist slippage and provide high stiffness; however, they are applied at the distal end of the tunnels and engage cortical bone, which is 30 times stronger than cancellous bone.5,10–12 The use of intratunnel devices such as the interference screw and IntraFix (DePuy Mitek, Norwood, MA) do not resist slippage, and the ACL graft readily elongates under cyclical load.5,13–15 Therefore the use of high-stiffness, slippage-resistant cortical fixation that purchases cortical bone is the best strategy for maintaining the initial length of the ACL graft and compensating for the obligatory loss in tension from cyclical movement of the knee and exercise (Fig. 29-2).2,3
Definition and Examples of High- and Low-Stiffness Fixation
High-stiffness fixation can be arbitrarily defined as a fixation stiffness that is greater than 400 N/mm when tested in young human bone. The WasherLoc with bone dowel (stiffness of 565 N/mm), the WasherLoc alone (506 N/mm), and tandem screws and washers placed on the cortex distal to the tibial tunnel (414 N/mm) all provide stiffness greater than 400 N/mm in young human bone (see Fig. 29-1). On the femoral side, the EZLoc (infinite stiffness) and Bone Mulch Screw (575 N/mm) are high-stiffness fixations because they purchase cortical bone, which is 30 times stronger than cancellous bone. Each of these high-stiffness cortical fixation devices resists slippage well during cyclical loading.5,6,11,16–20
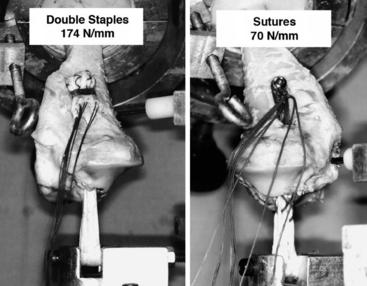
In contrast, low-stiffness fixation provides less than 400 N/mm in young human bone (Fig. 29-3). The interference screw (340 N/mm), double staples placed in the cortex distal to the tibial tunnel (174 N/mm), sutures tied to a post (70 N/mm), closed loop Endobutton (79 N/mm), IntraFix (49 N/mm), and sutures tied to an Endobutton (25 N/mm) are all examples of fixation devices that provide low stiffness. None of these low-stiffness intratunnel and cortical fixation devices resists slippage well during cyclical loading.*
Comment About Intratunnel Fixation with an Interference Screw
The location of fixation of an ACL graft with respect to the joint line has been a topic of debate.17,22–24 Proponents of fixation of an ACL graft at the level of the joint line with an interference screw base their opinion on two studies.7,9 The seminal study showed that anterior laxity was better restored with intratunnel fixation with an interference screw than with double staples applied distal to the tibial tunnel in porcine knees.7 A subsequent study showed that anterior laxity was better restored with intratunnel fixation with an interference screw than with sutures tied to a post in human knees.9 The explanation offered for the better restoration of anterior laxity with intratunnel fixation with an interference screw versus cortical fixation with double staples and sutures tied to a post was that intratunnel fixation shortens the effective length of the graft, which increases the stiffness of the knee.7–9
More recent studies have questioned the use of double staples, sutures tied to a post, and porcine knees to study the effect of the level of fixation on anterior laxity and knee stiffness. Double staples (174 N/mm) and sutures tied to a post (70 N/mm) are low-stiffness fixation devices (i.e., <200 N/mm), whereas distal tibial fixation devices such as tandem screws and washers (414 N/mm), WasherLoc (506 N/mm), and WasherLoc and bone dowel (565 N/mm) are high-stiffness fixation devices (i.e., >400 N/mm).5,17 Furthermore, these high-stiffness cortical fixation devices provide greater stiffness than interference screw fixation (340 N/mm) as well as greater strength and less slippage.5,9,16–18 Two studies have concluded that a porcine knee is not a reasonable surrogate for a human knee for evaluating the fixation structural properties of the interference screw in ACL reconstructions.5,15 Porcine bone overestimates the stiffness of the interference screw (476 N/mm) in comparison to young human tibia (340 N/mm) and overestimates the strength and underestimates slippage as well.5 Because the fixation structural properties of each of these high-stiffness cortical fixation devices are superior to those of the interference screw, they each might restore anterior laxity and knee stiffness in a human knee, even though the effective length of the graft is longer.5,17,18
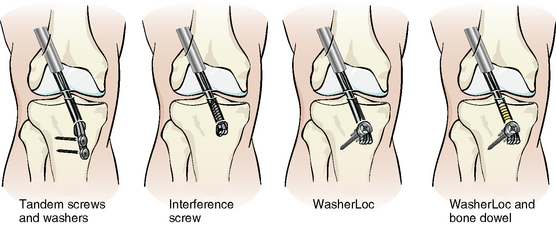
A more contemporary study that used high-stiffness, slippage-resistant cortical fixation has dispelled the dogma that intratunnel fixation with an interference screw provides more acute stability to the reconstructed knee (Fig. 29-4).4 This in vitro cadaver study using human bone evaluated the anterior laxity and knee stiffness provided by tandem screws and washers placed distal to the tibial tunnel, WasherLoc placed at the end of the tibial tunnel, and WasherLoc and bone dowel compared with an interference screw placed to the level of the joint line. Anterior laxity normalized to the intact knee with these three cortical fixation techniques of tandem washers, WasherLoc, WasherLoc and bone dowel. Each restored anterior laxity as well as intratunnel fixation with an interference screw. The additional stiffness provided by the cortical fixation device compensated for the slight reduction in ACL graft stiffness caused by the added length, which enabled the cortical fixation to restore anterior laxity as well as intratunnel fixation with an interference screw.
This finding is in contrast to Ishibashi’s study7 in porcine bone in which an interference screw placed at the joint line distal in the tibial tunnel provided better stability than staples placed distal to the tibial tunnel. One reason for these different findings in Ishibashi’s study compared with the study that used high-stiffness cortical fixation5 is that the interference screw provides 598 N/mm in porcine bone but only 350 N/mm in human bone. The cancellous bone has a higher density in a porcine knee than in a knee from a young individual, which overestimates the stiffness and strength and underestimates slippage of interference screw fixation when compared with young human tibia.5,15 Another reason for these different findings is that Ishibashi’s study underestimated the performance of the cortical fixation because it evaluated one of the least stiff cortical fixations—the double staples (174 N/mm)—instead of a high-stiffness, slippage-resistant cortical fixation. The overestimation of the performance of the interference screw in porcine bone suggests Ishibashi et al’s findings (i.e., that the level of fixation in porcine bone affects anterior laxity) should not be applied to a knee in young individuals.4
A second study by Sheffler et al confirmed Ishibashi et al’s findings by showing that low-stiffness cortical fixation does not restore anterior laxity as well as intratunnel fixation with an interference screw in human bone. Again, the authors underestimated the performance of the cortical fixation because they used the least stiff cortical fixation, which is a suture tied to a post (74 N/mm).9
In conclusion, high-stiffness, slippage-resistant cortical fixation devices restore anterior laxity and knee stiffness as well as intratunnel fixation with an interference screw fixation. This is different from the use of low-stiffness cortical fixation, which does not restore anterior laxity as well as intratunnel fixation with an interference screw. This leads to the principle that anterior laxity and knee stiffness are determined by the stiffness of the fixation device and not the location of the fixation device with respect to the joint line.1,4,6
Example of Stiffness Principle
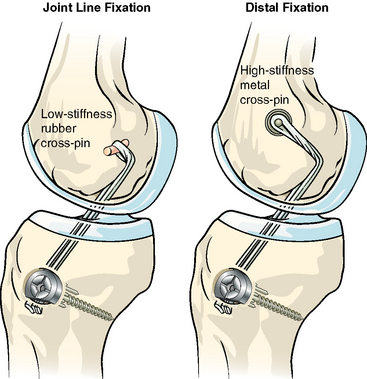
The importance of including the stiffness of the fixation device when determining the effect of the fixation device on the anterior laxity of the knee can be illustrated by the following example (Fig. 29-5). Consider a knee reconstructed with a soft tissue graft in which the femoral fixation is a rubber (low-stiffness) cross-pin placed near the joint line, and the tibial fixation is high-stiffness, slippage-resistant cortical fixation with a WasherLoc and bone dowel. Compare the anterior laxity with a low-stiffness rubber cross-pin placed at the joint line to a knee with a high-stiffness steel cross-pin placed farther from the joint line. The stiffness of the knee with the rubber cross-pin is extremely low even though the effective length of the graft is short. The stiffness of the knee with the metal cross-pin is high even though the effective length of the graft is long. Anterior laxity is better restored in the knee with the metal cross-pin and the longer effective graft length because the added stiffness provided by the fixation device more than compensates for the small increase in the effective length of the graft and because the graft is generally stiffer than the fixation device. 1,3–6
Biological and Mechanical Advantages of Cortical Fixation Over Intratunnel Fixation
The biological advantages of high-stiffness, slippage-resistant cortical fixation over intratunnel fixation with an interference screw include better healing because of the longer tunnel, circumferential healing of all sides of the graft to the tunnel wall, and the ability to bone graft the tunnel (Fig. 29-6). The biological bond between the tendon and tunnel wall is significantly stiffer and stronger in a longer tunnel than in a shorter tunnel because there is more bone surface area for the tendon to heal.27 Cortical fixation also allows circumferential biologic healing so that all sides of the tendon within the tunnel can heal to the bone. The interference screw blocks or “interferes” with healing on one side of the tendon, which causes a reduction of stiffness, slippage, and loss of strength 4 weeks after implantation that does not occur with cortical fixation.24 The use of high-stiffness, slippage-resistant fixation also allows bone grafting of the tibial tunnel.17 Bone grafting increases the snugness of fit between the tendon and tunnel wall and, as a biologically active component, may promote tendon tunnel healing.17,27,28
The mechanical advantage of cortical fixation over intratunnel fixation is that the cortical fixation device grips cortical bone instead of cancellous bone.10 Cortical bone is 30 times stronger than cancellous bone and is not as affected by other variables such as disuse, gender, age, alcohol, and smoking. Cortical fixation is stiffer, slips less, and is stronger than cancellous fixation with devices such as the interference screw or IntraFix.5,6,10,12,13 Cortical fixation permits bone grafting of the tunnel, which increases the stiffness 58 N/mm on the tibial side and 41 N/mm on the femoral side.6,17
Preferred Fixation Technique
Based on these observations of these various studies and the “stiffness principle,” we prefer to fix a soft tissue graft with high-stiffness, slippage-resistant cortical fixation that purchases cortical bone (Fig. 29-7). On the femoral side, the EZLoc rigidly suspends the graft from the cortex, which moves the fixation point from the cortical surface to inside the femoral tunnel. This tends to shorten the graft length but also preserves 25 to 30 mm of graft in the femoral tunnel so that circumferential biological healing can take place. Slippage of this construct does not occur because the lever arm sits directly on cortical bone and the graft is looped within a rigid metal slot. On the tibial side, the WasherLoc engages cortical bone and allows access to the tibial tunnel for the addition of a bone dowel or bone graft. The WasherLoc placed at the end of the tibial tunnel also preserves 30 to 35 mm of graft in the tunnel and allows circumferential tendon tunnel healing to take place.

1 Eagar P, Hull ML, Howell SM. How the fixation method stiffness and initial tension affect anterior load-displacement of the knee and tension in anterior cruciate ligament grafts: a study in cadaveric knees using a double-loop hamstrings graft. J Orthop Res. 2004;22:613-624.
2 Grover DM, Howell SM, Hull ML. Early tension loss in an anterior cruciate ligament graft. A cadaver study of four tibial fixation devices. J Bone Joint Surg. 2005;87A:381-390.
3 Karchin A, Hull ML, Howell SM. Initial tension and anterior load-displacement behavior of high-stiffness anterior cruciate ligament graft constructs. J Bone Joint Surg. 2004;86A:1675-1683.
4 Liu-Barba D, Howell SM, Hull ML. High stiffness cortical fixation restores anterior laxity and knee stiffness as well as intratunnel fixation with an interference screw: a cadaveric study of human knees reconstructed with a soft tissue anterior cruciate ligament graft. In press
5 Magen HE, Howell SM, Hull ML. Structural properties of six tibial fixation methods for anterior cruciate ligament soft tissue grafts. Am J Sports Med. 1999;27:35-43.
6 To JT, Howell SM, Hull ML. Contributions of femoral fixation methods to the stiffness of anterior cruciate ligament replacements at implantation. Arthroscopy. 1999;15:379-387.
7 Ishibashi Y, Rudy TW, Livesay GA, et al. The effect of anterior cruciate ligament graft fixation site at the tibia on knee stability: evaluation using a robotic testing system. Arthroscopy. 1997;13:177-182.
8 Morgan CD, Stein DA, Leitman EH, et al. Anatomic tibial graft fixation using a retrograde bio-interference screw for endoscopic anterior cruciate ligament reconstruction. Arthroscopy. 2002;18:E38.
9 Scheffler SU, Sudkamp NP, Gockenjan A, et al. Biomechanical comparison of hamstring and patellar tendon graft anterior cruciate ligament reconstruction techniques: the impact of fixation level and fixation method under cyclic loading. Arthroscopy. 2002;18:304-315.
10 Amis AA. The strength of artificial ligament anchorages. A comparative experimental study. J Bone Joint Surg Br. 1988;70:397-403.
11 Bailey SB, Grover DM, Howell SM, et al. Foam-reinforced elderly human tibia approximates young human tibia better than porcine tibia: a study of the structural properties of three soft tissue fixation devices. Am J Sports Med. 2004;32:755-764.
12 Kousa P, Jarvinen TL, Vihavainen M, et al. The fixation strength of six hamstring tendon graft fixation devices in anterior cruciate ligament reconstruction. Part I: femoral site. Am J Sports Med. 2003;31:174-181.
13 Caborn DN, Brand JCJr, Nyland J, et al. A biomechanical comparison of initial soft tissue tibial fixation devices: the IntraFix versus a tapered 35-mm bioabsorbable interference screw. Am J Sports Med. 2004;32:956-961.
14 Giurea M, Zorilla P, Amis AA, et al. Comparative pull-out and cyclic-loading strength tests of anchorage of hamstring tendon grafts in anterior cruciate ligament reconstruction. Am J Sports Med. 1999;27:621-625.
15 Nurmi JT, Sievanen H, Kannus P, et al. Porcine tibia is a poor substitute for human cadaver tibia for evaluating interference screw fixation. Am J Sports Med. 2004;32:765-771.
16 Coleridge SD, Amis AA. A comparison of five tibial-fixation systems in hamstring-graft anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2004;12:391-397.
17 Howell SM, Roos P, Hull ML. Compaction of a bone dowel in the tibial tunnel improves the fixation stiffness of a soft tissue anterior cruciate ligament graft: an in vitro study in calf tibia. Am J Sports Med. 2005;33:719-725.
18 Kousa P, Jarvinen TLN, Vihavainen M, et al. The fixation strength of six hamstring tendon graft fixation devices in anterior cruciate ligament reconstruction. Part II: tibial site. Am J Sports Med. 2003;31:182-188.
19 Roos PJ, Hull ML, Howell SM. Lengthening of double-looped tendon graft constructs in three regions after cyclic loading: a study using Roentgen stereophotogrammetric analysis. J Orthop Res. 2004;22:839-846.
20 Smith CK, Hull ML, Howell SM. Lengthening of a single-loop tibialis tendon graft construct after cyclic loading: a study using roentgen stereophotogrammetric analysis. J Biomech Eng. 2006;128:437-442.
21 Hoher J, Livesay GA, Ma CB, et al. Hamstring graft motion in the femoral bone tunnel when using titanium button/polyester tape fixation. Knee Surg Sports Traumatol Arthrosc. 1999;7:215-219.
22 Brown CHJr, Wilson DR, Hecker AT, et al. Graft-bone motion and tensile properties of hamstring and patellar tendon anterior cruciate ligament femoral graft fixation under cyclic loading. Arthroscopy. 2004;20:922-935.
23 Ma CB, Francis K, Towers J, et al. Hamstring anterior cruciate ligament reconstruction: a comparison of bioabsorbable interference screw and endobutton-post fixation. Arthroscopy. 2004;20:122-128.
24 Singhatat W, Lawhorn KW, Howell SM, et al. How four weeks of implantation affect the strength and stiffness of a tendon graft in a bone tunnel: a study of two fixation devices in an extraarticular model in ovine. Am J Sports Med. 2002;30:506-513.
25 Morgan CD, Kalmam VR, Grawl DM. Isometry testing for anterior cruciate ligament reconstruction revisited. Arthroscopy. 1995;11:647-659.
26 Weiler A, Hoffmann RF, Stahelin AC, et al. Hamstring tendon fixation using interference screws: a biomechanical study in calf tibial bone. Arthroscopy. 1998;14:29-37.
27 Greis PE, Burks RT, Bachus K, et al. The influence of tendon length and fit on the strength of a tendon-bone tunnel complex. A biomechanical and histologic study in the dog. Am J Sports Med. 2001;29:493-497.
28 Kyung HS, Kim SY, Oh CW, et al. Tendon-to-bone tunnel healing in a rabbit model: the effect of periosteum augmentation at the tendon-to-bone interface. Knee Surg Sports Traumatol Arthrosc. 2003;11:9-15.
[/level-membership-for-orthopaedics-category][not-level-membership-for-orthopaedics-category]
Chapter 29 High-Stiffness, Slippage-Resistant Cortical Fixation Has Many Advantages over Intratunnel Fixation
Fixation Stiffness and Slippage: Critical Factors in Restoring Anterior Laxity
An ACL graft construct is composed of the ACL graft and the two fixation devices at either end (Fig. 29-1). Anterior laxity in the knee of the athlete returning to sport is determined by the stiffness of the ACL graft construct and the length of the ACL graft, not by the strength of the graft and the tension in the graft.1–4
The stiffness of the ACL graft construct determines anterior laxity, the firmness of the Lachman test, and the quality of the “endpoint.” The stiffness of the ACL graft construct is increased more by the use of stiffer fixation devices than by the use of a shorter graft. A short graft with elastic fixation does not restore anterior laxity as well as a longer graft with stiffer fixation.5,6 The concept that shortening the graft increases the stiffness of the ACL graft construct, as proposed by some studies,7–9 is incorrect when high-stiffness, slippage-resistant cortical fixation devices are used.4 The most effective way to construct a stiff ACL graft and restore a firm Lachman test is to use high-stiffness, slippage-resistant cortical fixation devices on both ends of the graft.1,3,5,6
A determinant of anterior laxity that is as equally determinant as the stiffness of the ACL graft construct is maintenance of the length of the ACL graft set at the time of fixation. Maintaining the initial set length of the ACL graft after implantation requires the use of fixation devices that resist slippage during cyclical loading and exercise. Fortunately, there are fixation devices that do resist slippage and provide high stiffness; however, they are applied at the distal end of the tunnels and engage cortical bone, which is 30 times stronger than cancellous bone.5,10–12 The use of intratunnel devices such as the interference screw and IntraFix (DePuy Mitek, Norwood, MA) do not resist slippage, and the ACL graft readily elongates under cyclical load.5,13–15 Therefore the use of high-stiffness, slippage-resistant cortical fixation that purchases cortical bone is the best strategy for maintaining the initial length of the ACL graft and compensating for the obligatory loss in tension from cyclical movement of the knee and exercise (Fig. 29-2).2,3
Definition and Examples of High- and Low-Stiffness Fixation
High-stiffness fixation can be arbitrarily defined as a fixation stiffness that is greater than 400 N/mm when tested in young human bone. The WasherLoc with bone dowel (stiffness of 565 N/mm), the WasherLoc alone (506 N/mm), and tandem screws and washers placed on the cortex distal to the tibial tunnel (414 N/mm) all provide stiffness greater than 400 N/mm in young human bone (see Fig. 29-1). On the femoral side, the EZLoc (infinite stiffness) and Bone Mulch Screw (575 N/mm) are high-stiffness fixations because they purchase cortical bone, which is 30 times stronger than cancellous bone. Each of these high-stiffness cortical fixation devices resists slippage well during cyclical loading.5,6,11,16–20
In contrast, low-stiffness fixation provides less than 400 N/mm in young human bone (Fig. 29-3). The interference screw (340 N/mm), double staples placed in the cortex distal to the tibial tunnel (174 N/mm), sutures tied to a post (70 N/mm), closed loop Endobutton (79 N/mm), IntraFix (49 N/mm), and sutures tied to an Endobutton (25 N/mm) are all examples of fixation devices that provide low stiffness. None of these low-stiffness intratunnel and cortical fixation devices resists slippage well during cyclical loading.*
Comment About Intratunnel Fixation with an Interference Screw
The location of fixation of an ACL graft with respect to the joint line has been a topic of debate.17,22–24 Proponents of fixation of an ACL graft at the level of the joint line with an interference screw base their opinion on two studies.7,9 The seminal study showed that anterior laxity was better restored with intratunnel fixation with an interference screw than with double staples applied distal to the tibial tunnel in porcine knees.7 A subsequent study showed that anterior laxity was better restored with intratunnel fixation with an interference screw than with sutures tied to a post in human knees.9 The explanation offered for the better restoration of anterior laxity with intratunnel fixation with an interference screw versus cortical fixation with double staples and sutures tied to a post was that intratunnel fixation shortens the effective length of the graft, which increases the stiffness of the knee.7–9
More recent studies have questioned the use of double staples, sutures tied to a post, and porcine knees to study the effect of the level of fixation on anterior laxity and knee stiffness. Double staples (174 N/mm) and sutures tied to a post (70 N/mm) are low-stiffness fixation devices (i.e., <200 N/mm), whereas distal tibial fixation devices such as tandem screws and washers (414 N/mm), WasherLoc (506 N/mm), and WasherLoc and bone dowel (565 N/mm) are high-stiffness fixation devices (i.e., >400 N/mm).5,17
[/not-level-membership-for-orthopaedics-category]
