Chapter 51
Heart Disease in Pregnancy
1. What cardiac physiologic changes occur during pregnancy?
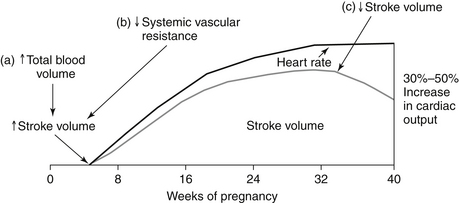
Hormonal changes cause an increase in both plasma volume (from water and sodium retention) and red blood cell volume (from erythrocytosis) during a normal pregnancy. A disproportionate increase in plasma volume explains the physiologic anemia of pregnancy. Maternal heart rate (HR) increases throughout the 40 weeks, mediated partially by increased sympathetic tone and heat production. Stroke volume subsequently continues to increase until the third trimester, when inferior vena cava (IVC) return may be compromised by the gravid uterus. Maternal cardiac output increases by 30% to 50% during a normal pregnancy. Systolic blood pressure drops during the first half of pregnancy and returns to normal levels by delivery. The physiologic changes related to cardiac output that occur during pregnancy are shown in Figure 51-1.
2. Are there independent vascular changes that occur during a normal pregnancy?
3. What are normal cardiac signs and symptoms of pregnancy?
 Hyperventilation (as a result of increased minute ventilation)
Hyperventilation (as a result of increased minute ventilation)
 Peripheral edema (from volume retention and vena caval compression by the gravid uterus)
Peripheral edema (from volume retention and vena caval compression by the gravid uterus)
 Dizziness/lightheadedness (from reduced SVR and vena caval compression)
Dizziness/lightheadedness (from reduced SVR and vena caval compression)

4. What are pathologic cardiac signs and symptoms of pregnancy?
 Anasarca (generalized edema) and paroxysmal nocturnal dyspnea are not components of normal pregnancy and warrant workup.
Anasarca (generalized edema) and paroxysmal nocturnal dyspnea are not components of normal pregnancy and warrant workup.



5. What are normal cardiac examination findings during pregnancy?
 Blood pressure (BP) will decline and HR will increase.
Blood pressure (BP) will decline and HR will increase.
 The point of maximum impulse will be displaced laterally as the uterus enlarges.
The point of maximum impulse will be displaced laterally as the uterus enlarges.

 A physiologic pulmonic flow murmur is common because of elevated stroke volume passing through a normal valve.
A physiologic pulmonic flow murmur is common because of elevated stroke volume passing through a normal valve.

6. What are pathologic cardiac exam findings during pregnancy?
 Clubbing and cyanosis are not a part of normal pregnancy; desaturation for any reason is abnormal and warrants investigation.
Clubbing and cyanosis are not a part of normal pregnancy; desaturation for any reason is abnormal and warrants investigation.



 Audible S4 is unusual during pregnancy and may reflect underlying hypertension.
Audible S4 is unusual during pregnancy and may reflect underlying hypertension.
7. What are the cardiac changes that occur during labor and delivery?
8. Which women should undergo infective endocarditis (IE) prophylaxis at the time of delivery?
IE prophylaxis is optional in vaginal delivery for patients with prior IE, prosthetic valves, and congenital heart disease (CHD) within the first 6 months of repair, or after 6 months if there is residual shunting, surgically constructed systemic-to-pulmonary shunts or conduits, or posttransplantation valvulopathy. It is not indicated in cesarean section, per 2007 American Heart Association (AHA) guidelines, although it is often given.
9. What maternal cardiac tests can be performed safely?
 Electrocardiograms and echocardiograms are safe, with no known risk to the fetus.
Electrocardiograms and echocardiograms are safe, with no known risk to the fetus.
 Chest radiographs can be performed with proper pelvic shielding.
Chest radiographs can be performed with proper pelvic shielding.
 MRI is considered safe (although there is little data during the first trimester).
MRI is considered safe (although there is little data during the first trimester).

 Transesophageal echocardiography (TEE) can be performed with appropriate sedation and monitoring.
Transesophageal echocardiography (TEE) can be performed with appropriate sedation and monitoring.

 Computerized tomography is relatively contraindicated due to radiation risk to the fetus.
Computerized tomography is relatively contraindicated due to radiation risk to the fetus.
 Nuclear imaging is contraindicated due to radiation risk to the fetus.
Nuclear imaging is contraindicated due to radiation risk to the fetus.
10. What are the highest-risk maternal cardiac conditions during pregnancy?
Moderate to severe mitral, aortic, and pulmonic stenosis are tolerated poorly during pregnancy. Patients should be counseled, with consideration of valvuloplasty or valve replacement before conception. These procedures can be performed during high-risk pregnancies if the patient decompensates. Pulmonary hypertension (pHTN) is also a high-risk condition, with historic maternal mortality rates of 30% to 56%. Although mortality remains unacceptably high, improvements in both the treatment of pHTN as well as the management of high-risk pregnancy have led to significant mortality reductions. Women with pHTN should be counseled regarding these risks. See Question 14 for discussion of CHD.
11. Are regurgitant lesions equally risky?
12. What are maternal complications seen in pregnant women with cardiac disease? What are some predictors of fetal complications?
13. How are pregnant women anticoagulated during pregnancy?
 Aggressive adjusted-dose twice-daily low-molecular-weight heparin (LMWH) throughout pregnancy with doses adjusted to achieve target peak anti–activated factor X (anti-Xa) level 4 hours postinjection, or
Aggressive adjusted-dose twice-daily low-molecular-weight heparin (LMWH) throughout pregnancy with doses adjusted to achieve target peak anti–activated factor X (anti-Xa) level 4 hours postinjection, or


Long-term anticoagulants should be resumed postpartum with all regimens, as early as the same evening. Low-dose aspirin can be optionally added for high-risk patients with mechanical heart valves. Mothers taking warfarin may nurse after delivery.
14. How are the common congenital lesions tolerated during pregnancy?
15. Which cardiac arrhythmias can complicate pregnancy?
16. How do you treat a pregnant woman with an acute myocardial infarction?
17. How do women with hypertrophic cardiomyopathy (HCM) tolerate pregnancy?
18. What are the recommendations for patients with Marfan syndrome?
19. Which commonly used cardiac medications should be avoided during pregnancy?
Common cardiac medications that should be avoided during part or all of pregnancy are listed in Box 51-1.
Box 51-1 SAFETY OF CARDIAC MEDICATIONS IN PREGNANCY
 Women should be counselled that warfarin is a class X drug per US Food and Drug Administration. LMWH or UFHs should replace warfarin in the first trimester and after 36 weeks of pregnancy.
Women should be counselled that warfarin is a class X drug per US Food and Drug Administration. LMWH or UFHs should replace warfarin in the first trimester and after 36 weeks of pregnancy.

 ACE inhibitors, ARBs, atenolol, and amiodarone are class D.
ACE inhibitors, ARBs, atenolol, and amiodarone are class D.
 Hydralazine with nitrates should replace ACE inhibitors and ARBs in patients with heart failure.
Hydralazine with nitrates should replace ACE inhibitors and ARBs in patients with heart failure.
 ACE inhibitors can be used in nursing mothers.
ACE inhibitors can be used in nursing mothers.
 Metoprolol, propranolol, or labetalol should be used instead of atenolol.
Metoprolol, propranolol, or labetalol should be used instead of atenolol.
Bibliography, Suggested Readings, and Websites
1. Bates, S.M., Greer, I.A., Middeldorp, S., et al. VTE, thrombophilia, antithrombotic therapy, and pregnancy: antithrombotic therapy and prevention of thrombosis, ed 9: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141:e691S–e736S.
2. Bédard, E., Dimopoulos, K., Gatzoulis, M.A. Has there been any progress made on pregnancy outcomes among women with pulmonary arterial hypertension? Eur Heart J. 2009;30:256–265.
3. Bonow, R.O., Carabello, B.A., Kanu, C., et al. ACC/AHA Guidelines for management of patients with valvular heart disease. Circulation. 2006;114:493–496.
4. Drenthen, W., Pieper, P., Roos-Hesselink, J., et al. Outcome of pregnancy in women with congenital heart disease: a literature review. J Am Coll Cardiol. 2007;49:2303–2311.
5. Elkayam, U., Bitar, F. Valvular heart disease in pregnancy, parts I (native) and II (prosthetic). J Am Coll Cardiol. 2005;46:223–230. 403–410
6. James, A.H., Brancazio, L.R., Price, T. Aspirin and reproductive outcomes. Obstet Gynecol Surv. 2008;63:49–57.
7. Kusters, D.M., Lahsinoui, H.H., van de Post, J.A. Statin use during pregnancy: a systematic review and meta-analysis. Expert Rev Cardiovasc Ther. 2012;10:363–378.
8. Reimold, S.C., Rutherford, J.D. Clinical practice: valvular heart disease in pregnancy. N Eng J Med. 2003;349:52–59.
9. Weiss, B.M., Zemp, L., Seifert, B., et al. Outcome of pulmonary vascular disease in pregnancy: a systematic overview from 1978 through 1996. J Am Coll Cardiol. 1998;31:1650–1657.
10. Wilson, W., Taubert, K., Gewitz, M., et al. Prevention of infective endocarditis: Guidelines from the AHA. Circulation. 2007;116:1736–1754.


