CHAPTER 25 Head and neck: overview and surface anatomy
This chapter contains an overview of the topographical anatomy of the head and neck described in detail in Chapters 26–34 Chapter 27 Chapter 28 Chapter 29 Chapter 30 Chapter 31 Chapter 32 Chapter 33 Chapter 34, and an account of the clinically relevant surface anatomy.
SKIN AND FASCIA
NECK
The superficial cervical fascia contains a variable amount of adipose tissue and platysma. The deep cervical fascia is conventionally subdivided into three sheets (investing, pretracheal and prevertebral layers) that surround the muscles and viscera of the neck to varying degrees, and the carotid sheath, a condensation of deep fascia around the common and internal carotid arteries, internal jugular vein, vagus and ansa cervicalis (see Ch. 28). The fascial layers of the neck define a number of potential tissue ‘spaces’ above and below the hyoid bone. In health, the tissues within these spaces are either closely applied to each other or are filled with relatively loose connective tissue. However, they offer potential routes by which unchecked infection may spread within the head and neck, and between the tissue spaces of the face and the mediastinum. They also offer convenient planes for intraoperative dissection during surgery.
BONES AND JOINTS
SKULL AND MANDIBLE
The skull is composed of 28 separate bones, most of them paired (Ch. 26). It can be divided into a robust calvarium that surrounds and protects the brain, and a delicate facial skeleton composed mainly of thin-walled bones, some of which contain air-filled cavities known collectively as the paranasal sinuses. The cranial cavity contains the brain and the intracranial portions of the cranial and spinal nerves; the blood vessels that supply and drain the brain and the haemopoietic marrow of the overlying bones; the meninges (dura, arachnoid and pia mater) and the cerebrospinal fluid (Ch. 27). The cavity is incompletely divided by dural partitions, notably the falx cerebri, lying between the cerebral hemispheres, and the tentorium cerebelli, lying between the cerebellum and occipital lobes. Almost all of the venous blood from the brain and cranial bones drains via sinuses lying between the endosteal and meningeal layers of the dura mater into the internal jugular vein (Ch. 27). Internally, the cranial base is divided into anterior, middle and posterior cranial fossae, which contain the frontal and temporal lobes of the cerebral hemispheres and the cerebellum respectively. Foramina in the bones of the skull base and facial skeleton transmit neurovascular bundles which may be compromised at these sites by pathology or trauma.
The skull provides attachments for numerous muscles. The craniofacial muscles arise from the bones of the facial skeleton, whereas the extrinsic muscles of the tongue, the muscles that act on the temporomandibular joint, the superior constrictor of the pharynx and the muscles of the soft palate all arise from sites on the cranial base. Movements of the mandible, which typically occur during mastication and articulation, take place at the temporomandibular joints (see Ch. 31). Movements of the skull on the cervical vertebrae occur at the atlanto-occipital joints (see Ch. 42).
CERVICAL VERTEBRAE
There are seven cervical vertebrae (see Ch. 42). They are the smallest of the movable vertebrae, and are characterized by a foramen in each transverse process, the foramen transversarium, and a disproportionately large vertebral canal. The first (atlas), second (axis) and seventh (vertebra prominens) cervical vertebrae are atypical.
HYOID BONE AND LARYNGEAL CARTILAGES
The hyoid bone (see Ch. 28) lies in the midline at the front of the neck at the level of the third cervical vertebra. It is suspended from the styloid processes by the stylohyoid ligaments and gives attachment to the supra- and infra-hyoid groups of muscles. The skeletal framework of the larynx is formed by a series of cartilages interconnected by ligaments and fibrous membranes, and moved by a number of muscles (Ch. 34). The laryngeal cartilages are the single cricoid, thyroid and epiglottic cartilages, and the paired arytenoid, cuneiform, corniculate and tritiate cartilages.
MUSCLES
The striated muscles of the head and neck produce the movements of the facial soft tissues that animate so many aspects of communication (Ch. 29); the movements at the temporomandibular joint that occur during mastication and speech (Ch. 31); the conjugate movements of the eyeballs (Ch. 39); and the co-ordinated movements that occur during activities such as swallowing, speaking and turning the head in response to visual and/or auditory stimuli. The ‘extrinsic’ muscles that run between the axial skeleton and upper limb act on the scapula and humerus (Ch. 46).
Smooth muscle occurs in the superior tarsal muscle, the sphincter and dilator pupillae and the ciliary muscle (Chs 39 and 40).
VASCULAR SUPPLY AND LYMPHATIC DRAINAGE
ARTERIAL SUPPLY
The main arterial supply of the head and neck is derived from branches of the carotid and subclavian arteries (Figs 25.1, 25.2). Branches of the internal carotid and vertebral arteries anastomose in the circle of Willis within the interpeduncular cistern on the ventral aspect of the brain (see Ch. 17).
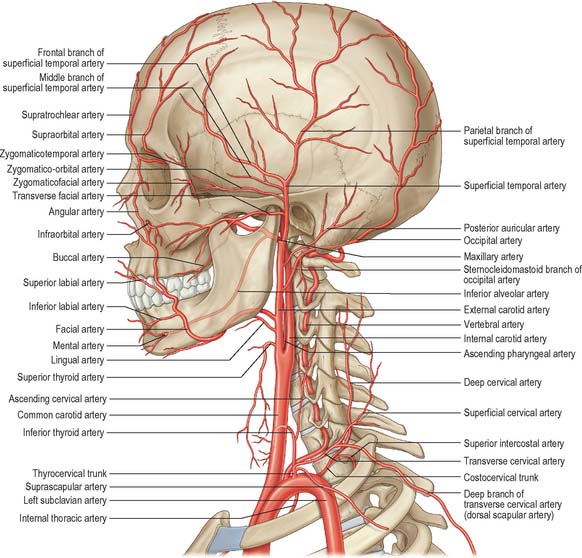

Carotid system
The cervical portion of the common carotid artery is similar on both sides. Each lies within the carotid sheath of deep cervical fascia, together with the internal jugular vein and vagus nerve. In the lower part of the neck the arteries are separated by a narrow gap which contains the trachea, and higher up they are separated by the thyroid gland, larynx and pharynx. At the level of the upper border of the thyroid cartilage (C4), the common carotid artery bifurcates into external and internal carotid arteries (see below). The external carotid artery passes upwards on either side of the neck, inclined at first slightly forwards and then backwards and a little laterally. It usually gives off the ascending pharyngeal, superior thyroid, lingual, facial, occipital and posterior auricular arteries, and then enters the parotid salivary gland where it divides into its terminal branches, the superficial temporal and maxillary arteries. The branches of the external carotid artery supply the face, scalp, tongue, upper and lower teeth and gingivae, palatine tonsil, paranasal sinuses and nasopharyngeal tube, external and middle ears, pharynx, larynx and superior pole of the thyroid gland. They also anastomose with branches of the internal carotid arteries on the scalp, forehead and face, and in the orbit, nasopharynx and nasal cavity, and with branches of the subclavian artery in the pharynx, larynx and thyroid glands.
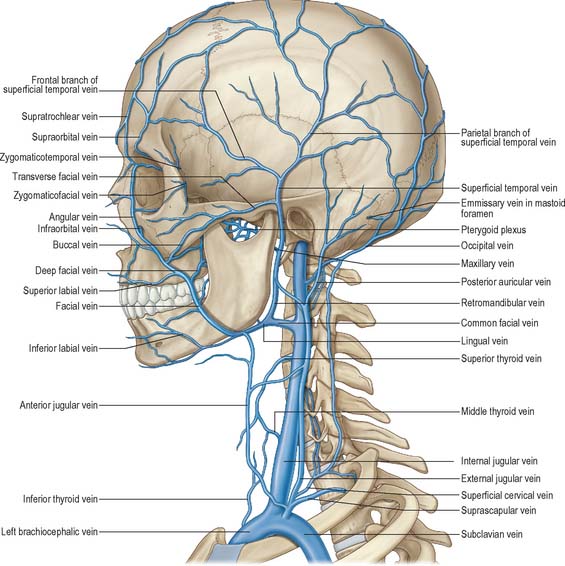
VENOUS DRAINAGE
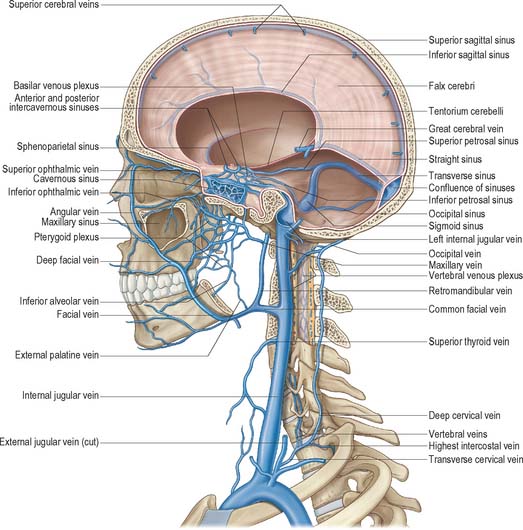
Veins of the neck lie superficial or deep to the deep investing fascia. Superficial veins ultimately drain into either the external, anterior or posterior external jugular veins, and drain a much smaller volume of tissue than the deep veins. Deep veins tend to drain into either the internal jugular vein or the subclavian vein. The internal jugular vein drains blood from the skull, brain, superficial face and much of the neck. It descends in the neck within the carotid sheath and unites with the subclavian vein behind the sternal end of the clavicle to form the brachiocephalic vein (Figs 25.3, 25.4). At its junction with the internal jugular vein, the left subclavian vein usually receives the thoracic duct and the right subclavian vein receives the right lymphatic duct.
LYMPHATIC DRAINAGE
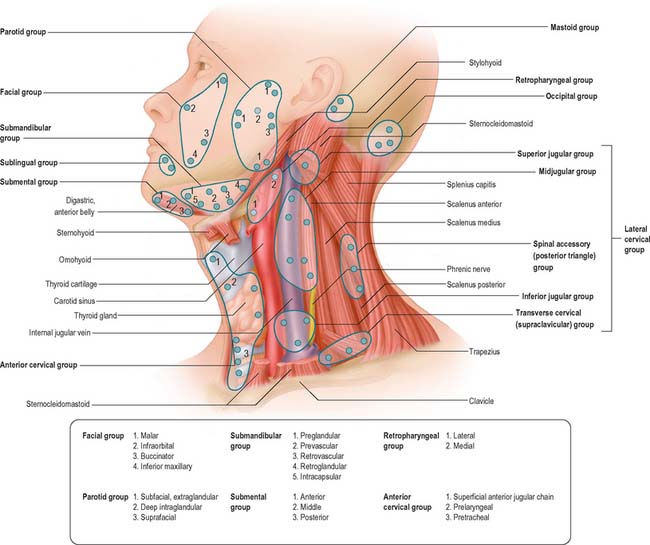
Lymph nodes in the head and neck are arranged in two horizontal rings and two vertical chains on either side of the neck (Fig. 25.5). The outer, superficial, ring consists of the occipital, preauricular (parotid), submandibular and submental nodes, and the inner, deep, ring is formed by clumps of mucosa associated lymphoid tissue (MALT) located primarily in the naso- and oro-pharynx (Waldeyer’s ring). The vertical chain consists of superior and inferior groups of nodes related to the carotid sheath. All lymph vessels of the head and neck drain into the deep cervical nodes, either directly from the tissues or indirectly via nodes in outlying groups. Lymph is returned to the systemic venous circulation via either the right lymphatic duct or the thoracic duct.
INNERVATION
CRANIAL NERVES
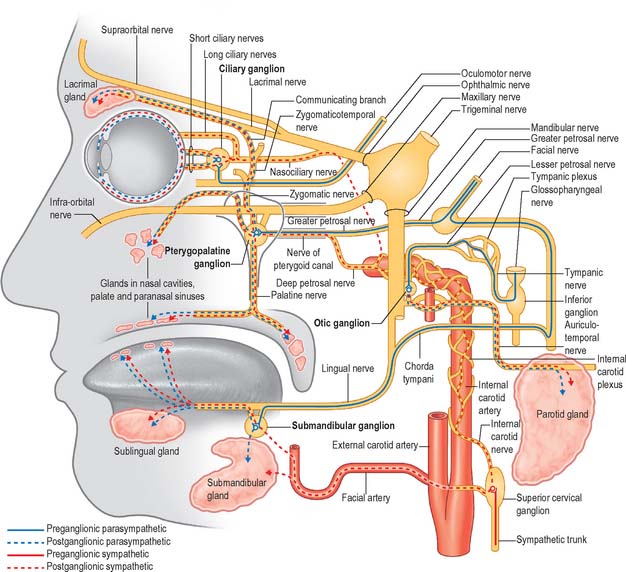
There are 12 pairs of cranial nerves. They are individually named and numbered (using Roman numerals) in a rostrocaudal sequence (see Table 15.1). Some are functionally mixed, others are either purely motor or purely sensory, and some also carry pre- or post-ganglionic parasympathetic fibres that are secretomotor to the salivary and lacrimal glands or motor to some of the smooth muscle within the eyeball. Branches of the oculomotor, trochlear, trigeminal, abducens, facial, glossopharyngeal, vagus, accessory and hypoglossal nerves supply muscle groups within the eyeball, face, pharynx, larynx and tongue. Branches of the trigeminal, glossopharyngeal and vagus nerves transmit general sensory information from the skin of the face and part of the scalp; the epithelium lining the oral and nasal cavities, the paranasal sinuses, middle ear, pharynx and larynx, and the dorsal surface of the tongue and the cornea; the intracranial meninges; the periosteum and bones of the skull. Branches of the trigeminal nerve innervate the temporomandibular joint. The olfactory, optic, trigeminal, facial, vestibulocochlear and vagus contain axons that transmit the special sensations of olfaction, vision, hearing, balance, and taste. The olfactory nerve is the only sensory cranial nerve that projects directly to the cerebral cortex rather than indirectly via the thalamus. The optic nerve terminates in the thalamus. The other ten pairs of cranial nerves are attached to the brainstem; their component fibres arise from or terminate in named cranial nerve nuclei (Ch. 19). The cranial nerves pass through named foramina in the skull, often with named vessels.
Reflexes
A number of reflexes involving structures in the head and neck are mediated by sensory and motor branches of certain of the cranial nerves, co-ordinated via appropriate nuclei in the brain stem. They include swallowing, gagging, retching and vomiting (Fig. 19.12); sneezing and coughing (Fig. 19.13); lacrimation (Fig. 39.25); jaw jerk (Fig. 19.17); visual reflexes (pupillary light reflex and accommodation) (see Ch. 40); corneal ‘blink’ reflex (Fig. 19.15); stapedial reflex (see p. 628, Ch. 36). Reflexes that involve energetic exhalation, e.g. sneezing and coughing, also involve the recruitment of cervical and thoracic spinal neurones to mediate the co-ordinated contraction of intercostal and abdominal wall muscles this activity requires.
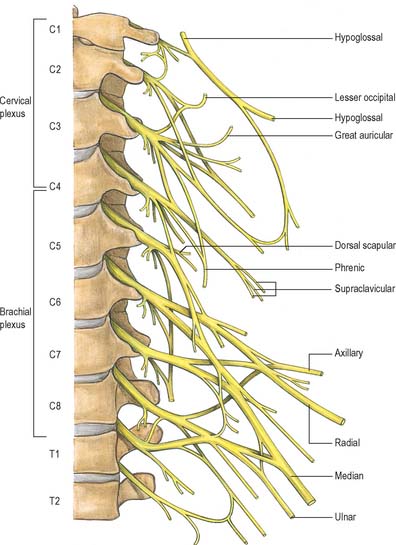
SPINAL NERVES
There are eight pairs of cervical spinal nerves (Fig. 25.6). Cutaneous branches of the dorsal rami of the second, third, fourth and fifth cervical nerves innervate the scalp and the skin over the back of the neck, and motor branches of all of the cervical dorsal rami supply cervical postvertebral muscles. All of the cervical ventral rami supply anterior and lateral groups of prevertebral muscles. The upper four cervical ventral rami form the cervical plexus whose branches collectively innervate the infrahyoid strap muscles and the diaphragm, and the skin covering the lateral and anterior parts of the neck, and the angle of the mandible. The lower four cervical ventral rami, together with most of the first thoracic ventral ramus, form the brachial plexus.