[level-membership-for-surgery-category]
CHAPTER 20 Hand-assisted right colectomy
Step 1. Surgical anatomy
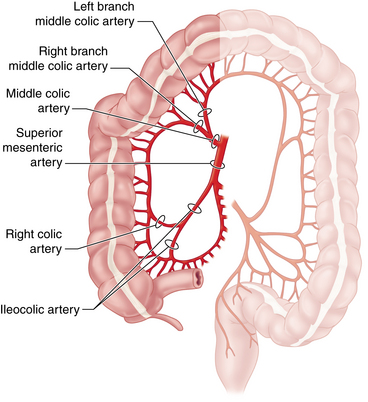
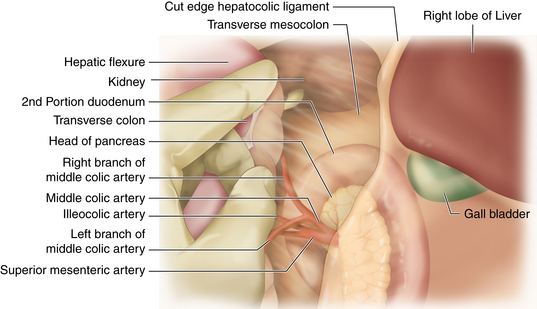
♦ Familiarity with the vascular anatomy of the right colon is essential to the safe conduct of a minimally invasive right colectomy (Figure 20-1). Vascular anatomy also significantly determines resection of colonic malignancies. Several key points guide the laparoscopic surgeon:





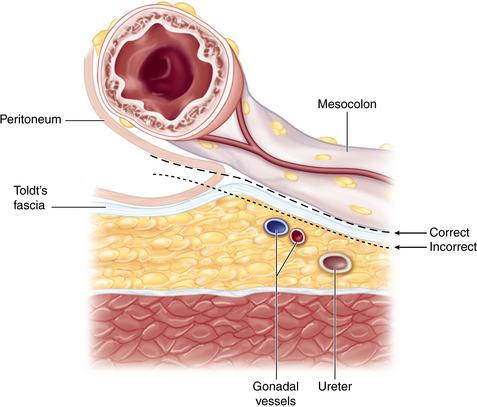
♦ The embryologic fusion plane originates laterally at the white line of Toldt, which occurs where the parietal peritoneum fuses with the visceral peritoneal reflection around the colon and its lateral extension (Figure 20-2). The correct dissection plane is the bloodless embryologic fusion plane. When properly mobilized in this plane, the colon reflects medially on its mesentery to become a nearly midline structure. When the dissection is carried posteriorly past the white line of Toldt, violating the parietal peritoneum as it extends across the retroperitoneal structures, the ureter and gonadal vessels are put at risk and mobilization of the colon is limited.
♦ Awareness of the relationships between the cecum, ascending colon, hepatic flexure, and proximal transverse colon to neighboring structures helps to maintain orientation during surgery and prevents injury:
 The duodenal sweep can be appreciated medial and caudal to the hepatic flexure mesocolon. Risk of injury to the portal triad can be averted by avoiding performance of a Kocher maneuver.
The duodenal sweep can be appreciated medial and caudal to the hepatic flexure mesocolon. Risk of injury to the portal triad can be averted by avoiding performance of a Kocher maneuver.



♦ Surface anatomy considerations principally help with optimal port placement:


Step 2. Preoperative considerations
Patient preparation
♦ Given that the majority of right colectomies are performed for neoplastic diseases (cancer or endoscopically unresectable polyps), staging must be complete before going to the operating room:
 A computed tomography (CT) scan of the chest, abdomen, and pelvis is central to the metastatic workup. A positron emission tomography (PET) scan is sometimes also necessary.
A computed tomography (CT) scan of the chest, abdomen, and pelvis is central to the metastatic workup. A positron emission tomography (PET) scan is sometimes also necessary.
♦ Lesions must be appropriately localized preoperatively. Although all of the patient’s physicians are concerned about making the correct diagnosis, only the surgeon has to perform a resection and must manage the technical details of this procedure:
 Review the colonoscopy report; note the expected location of the target lesion and the presence and character (including pathology report) of any other lesions.
Review the colonoscopy report; note the expected location of the target lesion and the presence and character (including pathology report) of any other lesions.


♦ Plan the extent of resection with regard to both margins and vascular ligation:
 The right branch of the MCA should be included for resection of neoplasms of the cecum or the proximal ascending colon.
The right branch of the MCA should be included for resection of neoplasms of the cecum or the proximal ascending colon.

♦ Past surgical history and an abdominal examination may reveal risks that could present challenges to a minimally invasive approach:
 Surgical scars and history of adhesions or bowel obstruction may alter port site placement or technique of entry.
Surgical scars and history of adhesions or bowel obstruction may alter port site placement or technique of entry.


♦ Formal stoma marking should be made preoperatively if there is a chance that an ileostomy will be created.
Anesthesia
♦ Prophylactic antibiotics are given to cover gram-negative and anaerobic organisms preoperatively. Coverage is extended postoperatively only for special situations.
♦ Prophylactic anticoagulation is used unless there are specific contraindications.
♦ An orogastric tube is placed by anesthesia to decompress the stomach.








Step 3. Operative steps
 The hand port template is used to demarcate the incision length, which should be no larger than the surgeon’s glove size (e.g., size 7 glove would require a 6- to 7-cm hand port incision).
The hand port template is used to demarcate the incision length, which should be no larger than the surgeon’s glove size (e.g., size 7 glove would require a 6- to 7-cm hand port incision).


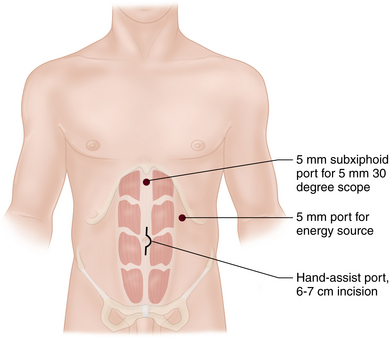
 Two additional ports (5 mm each) are placed. The subxiphoid port is placed just to the left of the midline (farther left if an extended right hemicolectomy is anticipated). The left upper quadrant port is placed at the midclavicular line, halving the distance between the costal margin and the superior end of the hand port incision (Figure 20-4).
Two additional ports (5 mm each) are placed. The subxiphoid port is placed just to the left of the midline (farther left if an extended right hemicolectomy is anticipated). The left upper quadrant port is placed at the midclavicular line, halving the distance between the costal margin and the superior end of the hand port incision (Figure 20-4).


 This is a top down approach. The anatomy is viewed from above and the dissection moves from the right upper quadrant to the right lower quadrant. Mobilization of the anatomy involves lifting the bowel and its mesentery up off of the retroperitoneum.
This is a top down approach. The anatomy is viewed from above and the dissection moves from the right upper quadrant to the right lower quadrant. Mobilization of the anatomy involves lifting the bowel and its mesentery up off of the retroperitoneum.





♦ The lymphovascular pedicles are identified and divided (Figure 20-5):
 Find the middle colic vessels near their origin by holding the transverse colon in the palm, elevate it, and use the index finger and thumb to palpate the base of the transverse mesocolon. One or more branches of the MCA will be divided depending on the extent of the resection. A bipolar vessel sealing (device can be used to divide the mesentery and vessels just caudal to the pancreas. Leave a stump of vessel behind in case there is bleeding so that a vascular load of a stapler Endostapler or an Endoloop can be applied.
Find the middle colic vessels near their origin by holding the transverse colon in the palm, elevate it, and use the index finger and thumb to palpate the base of the transverse mesocolon. One or more branches of the MCA will be divided depending on the extent of the resection. A bipolar vessel sealing (device can be used to divide the mesentery and vessels just caudal to the pancreas. Leave a stump of vessel behind in case there is bleeding so that a vascular load of a stapler Endostapler or an Endoloop can be applied.



♦ Desufflate the abdomen through the ports. This is particularly important in cancer resections to avoid seeding port sites with aerosolized tumor cells.
♦ Exteriorize the right colon through the gel port:

♦ Perform an ileocolic anastomosis. This can be done as for conventional open resections. Take care to avoid twisting the ileum, especially if it was divided intracorporally. Return bowel to the abdomen.
♦ Examine the specimen to be sure the target lesion is in the specimen.
♦ Close the incisions. No fascial closure is required for the 5-mm ports. Close the skin with a 4-0 absorbable deep dermal running suture followed by application of a wound sealant.
Step 4. Postoperative care
♦ A fast-track plan is encouraged.
♦ Analgesia. A PCA pump or Toradol with intermittent parenteral narcotics can be used, transitioning promptly to oral analgesics once solid food is started.
♦ Nasogastric tube. This is not routinely used unless there is extensive lysis of adhesions.
♦ Diet. Clear liquids are offered on postoperative day 1 and a soft diet on postoperative day 2 unless the patient has nausea, vomiting, distention, or significant belching.
♦ Urinary catheter. This is removed on postoperative day 1 or 2.
♦ Activity. The patient is encouraged to sit or stand at the bedside the day of surgery and to sit in a chair the morning following surgery. Ambulation is ordered on postoperative day 1.
♦ Discharge. The patient can be discharged once a diet is tolerated and bowel function has resumed. This usually happens by postoperative day 3 to 5.
Step 5. Pearls and pitfalls
♦ The learning curve for laparoscopic colon resection can be shortened by utilizing the hand-assisted approach:
 It is estimated that one must perform 25 to 50 pure laparoscopic colon resections to become proficient.
It is estimated that one must perform 25 to 50 pure laparoscopic colon resections to become proficient.
♦ The goal of the operation is to perform a safe operation (and a curative operation in the setting of cancer). Patients need a good operation, not necessarily a laparoscopic one.
♦ A periumbilical hand port incision is preferred to a Pfannenstiel incision for several reasons.
♦ Mobilization of the mesocolon around the duodenum should involve gentle, posterior displacement of the duodenum. Care should be taken to avoid mobilization of the duodenum (the Kocher maneuver) to avoid exposure of the porta hepatis and risk of injury to those structures.
♦ Avoid the temptation to ligate the vascular pedicles extracorporally. It’s never possible to reach the mesentery well once bowel is exteriorized, and it’s harder to control bleeding.
♦ Taking at least one branch of the middle colic artery helps assure good length of exteriorized transverse colon and avoid traction injury of the middle colic artery when exteriorizing the bowel.
♦ Leave a short stump of vessel behind when dividing vessels with a vessel sealing and cutting device.
♦ Adhesions in the lesser sac (fusion of the gastrocolic or hepatocolic ligaments with the retroperitoneum or adhesions between the posterior stomach and retroperitoneum) can interfere with adequate exposure of the transverse mesocolon and safe identification of the middle colic artery.
♦ Hand-assisted laparoscopic surgery is still image-based surgery. The hand is a sophisticated retraction device.
♦ This procedure safely handles bowel and protects it from the power source.
♦ Manipulation can thin tissue and help identify vessels.
♦ Typically, the index finger leads the way, the next three fingers provide retraction, and the thumb provides countertraction.
Cima RR, Pattana-arun J, Larson DW, et al. Experience with 969 minimal access colectomies: the role of hand-assisted laparoscopy in expanding minimally invasive surgery for complex colectomies. J Am Coll Surg. 2008;206;5:946-950. discussion 950-52
Hassan I, You YN, Cima RR, et al. Hand-assisted versus laparoscopic-assisted colorectal surgery: practice patterns and clinical outcomes in a minimally-invasive colorectal practice. Surg Endosc. 2008;22;3:739-743.
Lee SW, Yoo J, Dujovny N, et al. Laparoscopic vs. hand-assisted laparoscopic sigmoidectomy for diverticulitis. Dis Colon Rectum. 2006;49(4):464-469.
Marcello PW, Fleshman JW, Milsom JW, et al. Hand-assisted laparoscopic vs. laparoscopic colorectal surgery: a multicenter, prospective, randomized trial. Dis Colon Rectum. 2008;51;6:818-826. discussion 826-28
Ringley C, Lee YK, Iqbal A, et al. Comparison of conventional laparoscopic and hand-assisted oncologic segmental colonic resection. Surg Endosc. 2007;21(12):2137-2141.
Stein S, Whelan RL. The controversy regarding hand-assisted colorectal resection. Surg Endosc. 2007;21(12):2123-2126.
Targarona EM, Gracia E, Garriga J, et al. Prospective randomized trial comparing conventional laparoscopic colectomy with hand-assisted laparoscopic colectomy: applicability, immediate clinical outcome, inflammatory response, and cost. Surg Endosc. 2002;16;2:234-239.
Yamaguchi S, Kuroyanagi H, Milsom JW, et al. Venous anatomy of the right colon: precise structure of the major veins and gastrocolic trunk in 58 cadavers. Dis Colon Rectum. 2002;45;10:1337-1340.
[/level-membership-for-surgery-category][not-level-membership-for-surgery-category]
CHAPTER 20 Hand-assisted right colectomy
Step 1. Surgical anatomy
♦ Familiarity with the vascular anatomy of the right colon is essential to the safe conduct of a minimally invasive right colectomy (Figure 20-1). Vascular anatomy also significantly determines resection of colonic malignancies. Several key points guide the laparoscopic surgeon:
♦ The embryologic fusion plane originates laterally at the white line of Toldt, which occurs where the parietal peritoneum fuses with the visceral peritoneal reflection around the colon and its lateral extension (Figure 20-2). The correct dissection plane is the bloodless embryologic fusion plane. When properly mobilized in this plane, the colon reflects medially on its mesentery to become a nearly midline structure. When the dissection is carried posteriorly past the white line of Toldt, violating the parietal peritoneum as it extends across the retroperitoneal structures, the ureter and gonadal vessels are put at risk and mobilization of the colon is limited.
♦ Awareness of the relationships between the cecum, ascending colon, hepatic flexure, and proximal transverse colon to neighboring structures helps to maintain orientation during surgery and prevents injury:
The duodenal sweep can be appreciated medial and caudal to the hepatic flexure mesocolon. Risk of injury to the portal triad can be averted by avoiding performance of a Kocher maneuver.♦ Surface anatomy considerations principally help with optimal port placement:
Step 2. Preoperative considerations
Patient preparation
♦ Given that the majority of right colectomies are performed for neoplastic diseases (cancer or endoscopically unresectable polyps), staging must be complete before going to the operating room:
A computed tomography (CT) scan of the chest, abdomen, and pelvis is central to the metastatic workup. A positron emission tomography (PET) scan is sometimes also necessary.♦ Lesions must be appropriately localized preoperatively. Although all of the patient’s physicians are concerned about making the correct diagnosis, only the surgeon has to perform a resection and must manage the technical details of this procedure:
Review the colonoscopy report; note the expected location of the target lesion and the presence and character (including pathology report) of any other lesions.♦ Plan the extent of resection with regard to both margins and vascular ligation:
The right branch of the MCA should be included for resection of neoplasms of the cecum or the proximal ascending colon.♦ Past surgical history and an abdominal examination may reveal risks that could present challenges to a minimally invasive approach:
Surgical scars and history of adhesions or bowel obstruction may alter port site placement or technique of entry.[/not-level-membership-for-surgery-category]
