Chapter 12 Hamstring Harvest Technique for Anterior Cruciate Ligament Reconstruction
Technique of Hamstring Graft Harvest
The graft harvest can be the most difficult aspect of this operation. Videotapes of this technique by Fowler, Prodromos, and Fox are available from the AAOS library.1
The anatomy of the hamstrings has been described in the literature by Ferrari and Ferrari.2 The strength of the hamstrings after harvest of the tendons was initially reported by Lipscomb et al3 to be the same as the opposite side. Since then, weakness of knee flexion above 90 degrees of knee flexion has been reported.4 Based on these reports, one should be cautious in recommending hamstring grafts for sprinters, who require full, active knee flexion strength. Yasuda et al5 have described the harvest site morbidity as minimal. Gobbi et al6 recommend preservation of the gracilis to prevent postoperative knee flexion weakness. The regeneration of the hamstring tendons after the harvest was described by Cross et al.7
Skin Incision
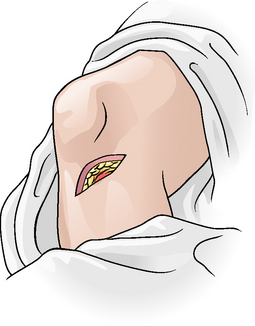
The skin incision for hamstring harvest should be made with the knee flexed in the figure-four position (Fig. 12-1). An oblique, 3-cm skin incision is made 5 cm below the joint line over the proximal edge of the pes anserine. The incision should start 1 cm medial to the tibial tubercle and then continue posteromedially. The oblique incision is preferable to the vertical incision for two reasons: It gives a greater exposure to the top of the pes anserine, and it also has less potential to injure the infrapatellar branch of the saphenous nerve. Plan to harvest the graft and drill the tibial tunnel through this incision. Incise the subcutaneous fat, and strip the fat off the pes anserine with a sponge.
Exposure of the Tendon
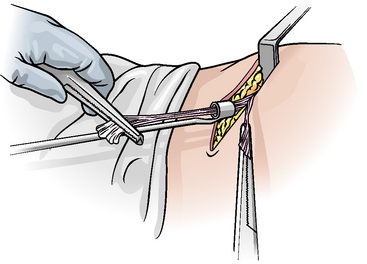
Identify the superior border of the pes by palpating the superior edge with your finger. Lift up this superior border, and incise the fascia. Identify the bursa between the pes and the medial collateral ligament by placing the tip of the scissors in the space. With the scissors, continue the incision medially down the tibia, in an L-shaped fashion, removing the tendons distally. Use a Kocher to apply traction to this top corner. Turn the pes down to look on the underside for the most inferior tendon, the semitendinosus (Fig. 12-2). Lift the tendon up with the tip of the scissors, and grasp it with a Kocher. Lift up the gracilis, and grasp it in a similar fashion with a Kocher. Divide the conjoined tendon between the semitendinosus and the gracilis.

Tendon Release
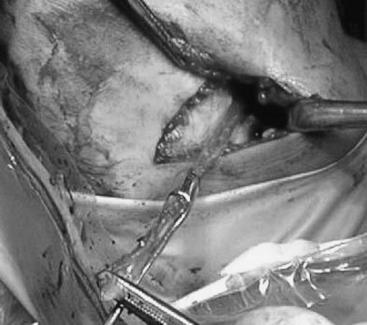
Free the distal end of the tendon with the scissors. Make sure you get the full length distally. Grasp it with a Kocher, and pull it firmly into the incision. Many of the bands can be released with the traction and by blunt finger dissection. The main band that goes to the medial head of the gastrocnemius will usually have to be cut with the scissors (Fig. 12-3). Pull firmly on the tendon, and cut away from the tendon (to avoid cutting the tendon with the scissors) (Fig. 12-4). The tendon should not retract proximally if all the bands are cut. When the tendon is pulled distally, there is no dimpling posteriorly over the gastrocnemius.

Stripping of the Tendon
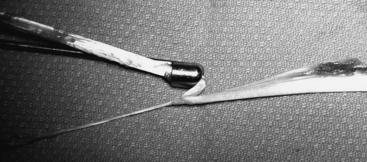
Advance the tendon stripper up over the tendon to free it from the muscle proximally (Fig. 12-5). The key to a successful harvest is to keep tension on the distal end. This will prevent the tendon from folding over and being cut off short (Fig. 12-6). Make sure that the tendon stripper is heading up the thigh in the same direction as the tendon. There is often resistance at the muscle tendon junction, and the stripper should be rotated to slip it up along the surface of the muscle. This gives extra length. The total length is usually 28 to 30 cm. Strip the gracilis tendon in a similar fashion.
Preparation of the Graft
Preparation of the Four-Bundle Semitendinosus and Gracilis Graft
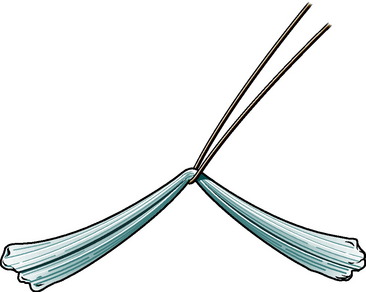
Take the graft to the graft master on the back table. Lay out, measure, and cut the graft to 22 cm. Remove the muscle with the periosteal elevator. Loop the two tendons over a #5 braided nonabsorbable suture to produce an 11-cm graft (Fig. 12-7). With this length, 2.5 cm is in the femur, 2.5 cm is intraarticular, and 5 cm is in the tibial tunnel. This ensures a small portion of the graft is at the cortex of the tibia for fixation with the screw. Whipstitch the individual ends of the tendons with a #2 nonabsorbable suture for a distance of 4 cm (Fig. 12-8). Make sure that each tendon has a suture in it. This allows you to tension each bundle of the composite graft. The completed four-bundle graft should be 11 cm in length. This four-bundle graft will be three times the strength of a single strand of semitendinosus, assuming all bundles are equally tensioned.8 Incorporate the graft into the bone tunnel by Sharpey fibers.9 This will take about 10 to 12 weeks to heal. This graft will have at least 2.5 cm of graft in each tunnel. The depth of graft in the tunnel can be determined by the suture marks at each end.


Tips for Harvesting the Hamstring Grafts to avoid complications
2 Ferrari JD, Ferrari DA. The semitendinosus: anatomic considerations in tendon harvesting. Orthop Rev. 1991;20:1085-1088.
3 Lipscomb AB, Johnston RK, Snyder RB, et al. Evaluation of hamstring strength following use of semitendinosus and gracilis tendons to reconstruct the anterior cruciate ligament. Am J Sports Med. 1982;10:340-342.
4 Tashiro T, Kurosawa H, Kawakami A, et al. Influence of medial hamstring tendon harvest on knee flexor strength after anterior cruciate ligament reconstruction. A detailed evaluation with comparison of single- and double-tendon harvest. Am J Sports Med. 2003;31:522-529.
5 Yasuda K, Tsujino J, Ohkoshi Y, et al. Graft site morbidity with autogenous semitendinosus and gracilis tendons. Am J Sports Med. 1995;23:706-714.
6 Gobbi A, Domzalski M, Pascual J, et al. Hamstring anterior cruciate ligament reconstruction: is it necessary to sacrifice the gracilis? Arthroscopy. 2005;21:275-280.
7 Cross MJ, Roger G, Kujawa P, et al. Regeneration of the semitendinosus and gracilis tendons following their transection for repair of the anterior cruciate ligament. Am J Sports Med. 1992;20:221-223.
8 Hamner DLB, Steiner CHJr, Hecker ME, et al. Hamstring tendon grafts for reconstruction of the anterior cruciate ligament: biomechanical evaluation of the use of multiple strands and tensioning techniques. J Bone Joint Surg Am. 1999;81:549-557.
9 Weiler A, Hoffmann RF, Bail HJ, et al. Tendon healing in a bone tunnel. Part II: histologic analysis after biodegradable interference fit fixation in a model of anterior cruciate ligament reconstruction in sheep. Arthroscopy. 2002;18:124-135.






