Chapter 664 Growth and Development
Terms to describe some common deviations from normal are listed in Table 664-1. Congenital anomalies can be categorized into production problems and packaging problems. Production problems include abnormalities caused by malformation, dysplasia, or disruption that will not spontaneously resolve. Packaging problems include deformations caused by mechanical causes including in utero positioning and molding, and they usually resolve with time.
Table 664-1 TERMINOLOGIES FOR DEVIATIONS
| TERMINOLOGY | DESCRIPTION |
|---|---|
| Congenital | Anomaly that is apparent at birth |
| Deformation | A normally formed structure that is pushed out of shape by mechanical forces |
| Deformity | A body part altered in shape from normal, outside the normal range |
| Developmental | A deviation that occurs over time; one that might not be present or apparent at birth |
| Disruption | A structure undergoing normal development that stops developing or is destroyed or removed |
| Dysplasia | A tissue that is abnormal or wrongly constructed |
| Malformation | A structure that is wrongly built; failure of embryologic development or differentiation resulting in abnormal or missing structures |
Growth and Development
Anatomic Locations: Descriptive Terms
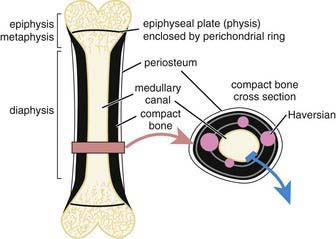
Typical long bones are divided into the physis, eiphysis, metaphysis, diaphysis, and perichondrial ring (Fig. 664-1). The physis is the growth plate located at the end of bone. The epiphysis is typically a secondary ossification center that contributes to joint development. The metaphysis is the bone adjacent to the physis on the side away from the joint. The diaphysis is the central part or shaft of long bones. The perichondrial ring contributes to appositional growth.
Important Growth and Developmental Milestones
Some important musculoskeletal growth considerations are summarized in Table 664-2.
Table 664-2 SKELETAL GROWTH CONSIDERATIONS
Growth Patterns in Upper and Lower Extremities
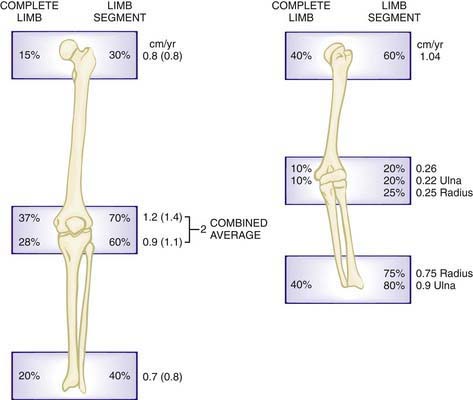
The upper extremity grows longitudinally, primarily from physes of the proximal humeral physis and the distal radial and ulnar physes. In the lower extremity, most of the longitudinal growth occurs around the knee, in the distal femoral and the proximal tibial physes (Fig. 664-2).
Ballock RT, O’Keefe RJ. The biology of the growth plate. J Bone Joint Surg Am. 2003;85:715-726.
Davids JR. Normal gait and assessment of gait disorders. In: Morrissy R, Weinstein S, editors. Lovell and Winter’s pediatric orthopedics. ed 5. Philadelphia: Lippincott Williams & Wilkins; 2001:131-156.
Dimeglio A. Growth in pediatric orthopedics. In: Morrissy R, Weinstein S, editors. Lovell and Winter’s pediatric orthopedics. ed 5. Philadelphia: Lippincott Williams & Wilkins; 2001:33-62.
Frick SL. Normal growth and development in pediatric orthopedics. In: Dormans JP, editor. Pediatric orthopedics: core knowledge in orthopedics. Philadelphia: Mosby; 2005:1-14.
Ogden J. Anatomy and physiology of skeletal development. In: Catterall A, editor. Skeletal injury in the child. ed 3. New York: Springer-Verlag; 2000:1-37.
Song KM, Little DG. Peak height velocity as a maturity indicator for males with idiopathic scoliosis. J Pediatr Orthop. 2000;20:286-288.
Westh RN, Menelaus MB. A simple calculation for the timing of the epiphyseal arrest. J Bone Joint Surg Br. 1981;63:117-119.




