Chapter 53 Graft Tensioning in Anterior Cruciate Ligament Reconstruction
Introduction
On the basis of clinical experience, pioneers of current ACL reconstruction procedures preferred to apply relatively high initial tension to not only the doubled pes tendon autograft but also the patellar tendon autograft at the time of fixation.1–4 For example, Clancy et al1 performed ACL reconstruction using the distally stacked and proximally free central third of the patellar tendon as an autograft and recommended that the patellar bone block be pulled with three sutures through the femoral tunnel as far as it would go within the tunnel. On the other hand, a number of in vitro and in vivo experimental studies suggested that a high initial tension had detrimental effects not only on the graft but also on the knee after ACL reconstruction. Some recent studies, however, reported that a high initial tension was better than a low initial tension in simulation of a middle- or long-term effect. Thus there has been considerable disagreement on the effects of initial graft tension among the previous studies. It has been necessary therefore to conduct randomized clinical trials on the effect of initial graft tension on the outcome after ACL reconstruction. At the present time, four articles on the effect of initial graft tension on the clinical outcome are available for review. In this chapter, the author reviews recent experimental and clinical studies on the effect of graft tensioning during ACL reconstruction on the graft and the ACL reconstructed knee and explains what has and has not been clarified at the present time.
In Vitro Biomechanical Studies on Graft Tensioning
The Effect of the Initial Tension on the Tension-Flexion Curve
In the normal knee, tension in the normal ACL decreases with knee flexion from the maximum value obtained at 0 degrees to the minimum value near 30 degrees and then slightly increases with further flexion.5,6 This relationship between the ACL tension and the knee flexion angle is well known as a tension-flexion curve. In ACL reconstruction, the initial tension is defined as a tension applied to the graft at a selected angle of knee flexion during surgery. Then we should know the effect of the initial tension on the tension-flexion curve in ACL reconstruction. In vitro biomechanical studies5,7 reported that in the standard single-bundle ACL reconstruction procedures, increase of the initial tension applied at some angle of knee flexion increased the graft tension by a constant magnitude at every flexion angle during knee motion and that consequently the shape of the tension-flexion curve was not changed (Fig. 53-1). Namely, it means that an increase of the initial graft tension at 30 degrees of knee flexion results in an increase of the graft tension at every knee flexion angle. In 2001, Fleming et al8 measured the laxity in nine different tensioning conditions: three tension magnitudes (30, 60, and 90N), each applied with the knee at three angles (30, 60, and 90 degrees), in a goat ACL reconstruction model using a bone–tendon–bone (BTB) graft. They stated that both the graft tension and the knee angle produced significant changes on anteroposterior laxity values.
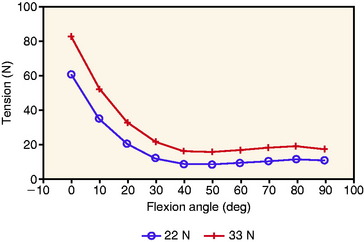
These in vitro studies indicated that both the initial tension value and the knee flexion angle at the time of tensioning and fixation are critical in the ACL reconstruction. In the standard ACL reconstruction procedures, when a surgeon applies a certain “initial” tension value at about 30 degrees of knee flexion, a graft tension value obtained at more extension positions or more flexion positions is greater than the initial tension value.7 Conversely, when a surgeon applies a certain initial tension value at the full extension position of the knee, graft tension values at flexion positions are lower than the initial tension value. Clinically, a number of surgeons have preferred to fix the graft at approximately 30 degrees of knee flexion in order to avoid an insufficient tension after surgery, specifically for the hamstring tendon graft. On the other hand, recently many surgeons who perform ACL reconstruction with the BTB graft have preferred to fix the graft at the full extension position to avoid postoperative flexion contracture of the knee due to overtensioning of the graft.
Relaxation of Graft Tension after Surgery
In vitro biomechanical studies have shown that viscoelastic creep of the graft causes relaxation of graft tension. Howard et al9 quantified viscoelastic creep in the BTB graft using both an in vivo and an in vitro model. In the in vivo model, 10-mm BTB grafts were elongated by 14.0% after 89N was applied for a minimum of 4 minutes. In the in vitro model, grafts were elongated by 10.1% after 89N was applied for 15 minutes. This study highlights the importance of the time for preconditioning the graft before grafting.
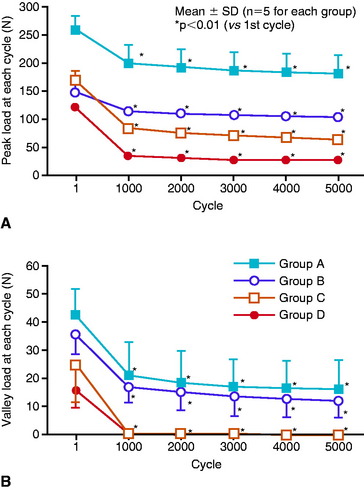
The author and his colleagues10–12 reported that more obvious relaxation of graft tension occurred due to elongation of a bone–graft–bone complex that is composed of bones, tendon grafts, and all artificial materials to be used for graft fixation. They measured the influence of 5000 cycles of submaximal cyclical displacement upon the tension of various types of the bone–graft–bone complex after ACL reconstruction. For example, Yamanaka et al10 showed that initial tension of 80N applied to the four-strand flexor tendon graft tethered to the screw post with a suture was reduced to 0N after 5000 cycles of 2-mm stretching, while the same initial tension applied to the BTB graft fixed with interference screws was reduced to 17N (Fig. 53-2). In addition, the relaxation rate in the BTB graft fixed with interference screws was less than that in the BTB graft fixed with sutures and screw posts, whereas the relaxation rate in the flexor tendon graft fixed with sutures and screw posts was greater than that in the BTB graft fixed with the sutures and screw points (see Fig. 53-2). Boylan et al13 applied an initial tension of 68N, 45N, and 23N to the hamstring graft at 30 degrees of flexion, fixed with a suture and post technique. After 1000 cycles of knee motion between 0 and 90 degrees, the tension in the graft decreased to 34.5N, 16.8N, and 15.4N, respectively. Arnold et al14 applied 40N initial tension to the BTB graft at 20 degrees of flexion in ACL reconstruction with cadavers, fixed with interference screws. The graft tension at 0 degrees of flexion dropped from 208N, or by 41% at 500 cycles. Anterior laxity increased from +1.4 to +2.8 mm by 500 cycles.
Effects of a High or Low Initial Tension on the Graft and the Knee
A number of in vitro studies with cadaver knees, which simulated conditions immediately after ACL reconstruction, showed that an increase of ACL tension decreased the degree of anterior translation of the tibia to the femur.7,15–17 Melby et al17 described that an 18N tension applied to the graft at 30 degrees of knee flexion restored the laxity and stiffness most closely resembling that of the intact knee, without inducing significant abnormal laxities, but that tensions greater than 54N overconstrained the knee. Several in vitro studies warned that overtensioning might result in restriction in range of motion and graft failure.18–20 For example, Nabors et al19 showed that when a high initial tension was applied to the BTB graft at 30 degrees of knee flexion, loss of knee extension frequently occurred after surgery. Graf et al20 indicated that a high tension induced wear-related graft failure. Eager et al21 reported that a high initial tension induced posterior subluxation of the tibia with respect to the femur, specifically when a graft having low stiffness was used. Thus the just-described in vitro studies recommended a low initial tension be applied to the graft in ACL reconstruction.
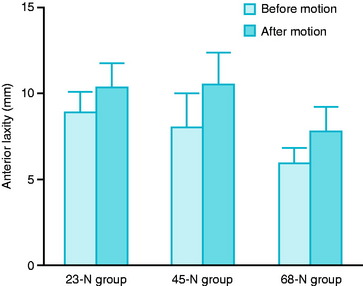
However, a criticism of these in vitro studies is that they did not take the graft relaxation into account. Beynnon et al15 reported that because the tension applied on a graft at the time of fixation was acutely decreased by creep elongation of an autograft or transposition of an autograft in the bone tunnel, insufficient initial tension applied on the graft during surgery might result in slackness of a reconstructed ligament tissue. In 2002, Numazaki et al12 stretched a few types of the femur–graft–tibia complex by 2 mm for 5000 cycles, after an initial tension of 20N, 80N, and 140N was applied for 2 minutes. In a four-strand flexor tendon graft with Endobutton fixation, the peak load values at the 5000th cycle were 17N, 40N, and 77N, respectively. The researchers stated that applying an initial graft tension of approximately 80N did not appear to be too high for the hamstring tendon graft with Endobutton fixation after graft relaxation. In 2003, Boylan et al13 applied an initial tension of 68N, 45N, and 23N to the hamstring graft at 30 degrees of flexion, fixed with a suture and post technique. The average laxity showed 6.0 mm, 8.1 mm, and 8.9 mm, respectively. After 1000 cycles of knee motion between 0 and 90 degrees, the tension in the graft decreased to 34.5N, 16.8N, and 15.4N, respectively, and the average laxity increased to 7.8 mm, 10.5 mm, and 10.3 mm, respectively (Fig. 53-3). They concluded that to restore anterior translation to within 3 mm of the native ACL condition after cyclical loading, a relatively high tension of approximately 68N was required using this fixation technique.
Clinical Relevance from the Previous In Vitro Studies
We should note that there are some agreements in the previous in vitro studies. First, an increase in graft tension decreases the degree of anterior translation of the tibia to the femur. Second, a high initial tension applied to the graft overconstrains the knee at least immediately after surgery. Third, relaxation of graft tension commonly occurs in a relatively early phase after surgery, and the degree and velocity of the graft relaxation depend on a combination of the graft and all artificial materials used for graft fixation. Fourth, although behaviors of the ACL reconstructed knee have been considered to be graft specific,16 we should now recognize that the behavior of the ACL reconstructed knee is graft fixation device–specific. However, we also should note that there is considerable disagreement among the clinical messages from the previous in vitro studies on clinical ACL reconstruction. The relaxation of the graft tension after surgery may be an important key to understand the causes of this disagreement. Also, we have found some serious limitations in the in vitro studies. Thus, in vivo studies with animal ACL reconstruction models have been necessary.
In Vivo studies with Animal Anterior Cruciate Ligament Reconstruction Models
Essential Effects of Tension on the Graft Properties
Before discussing the effect of graft tensioning on the outcome after ACL reconstruction, we should understand the essential effect of tension on the tendon graft. The author and his associates have performed a series of in vivo studies on the effect of stress on the in situ frozen-thawed patellar tendon and ACL, which are idealized extraarticular and intraarticular autograft models, respectively.22–26 Regarding the effect of low stress, Ohno et al22 and Majima et al23 demonstrated that reduction of stress dramatically reduced the mechanical properties of the in situ frozen-thawed rabbit patellar tendon at 3, 6, and 12 weeks after surgery. Regarding the effect of high stress, Tohyama and Yasuda25 reported that enhancement of stress also reduced the mechanical properties of the in situ frozen-thawed rabbit patellar tendon at 6 weeks after surgery. Also, Katsuragi et al26 applied a high tension to the in situ frozen-thawed canine ACL in which the applied high tension was proven to be continuously maintained in the experimental period. This study demonstrated that an unphysiologically high tension significantly deteriorated the mechanical properties of the in situ frozen canine ACL at 12 months after surgery when compared with physiological tension. These in vivo studies revealed the essential effects of stress to the tendon graft. Namely, continuous application of both excessively high and low initial tensions has detrimental effects on the graft. We should note that the latter is stronger than the former. However, we should recognize that the mechanical conditions surrounding the free tendon graft may be different from those in these scientific studies because an initially applied tension may be reduced to various degrees. Even in the idealized ACL reconstruction model with the canine in situ frozen-thawed ACL, the initial graft tension is chronically relaxed over time due to biological mechanisms.27
Effects of Initial Tension on Anterior Cruciate Ligament Reconstruction Models
Regarding the effect of initial tension on knee stability, function, and pathology, Yoshiya et al28 investigated the effects of 1N and 39N initial loads on a canine ACL reconstruction model with a free patellar tendon graft. They observed poor vascularity and focal myxoid degeneration within the graft pretensioned with a load of 39N, but not within the graft with 1N of tension applied. Although they detected no significant difference in the values for the ultimate failure load of the graft 3 months after reconstruction, they suggested that a high degree of tension might be detrimental to the patellar tendon autograft during surgical reconstruction of the ACL.
Using the in situ frozen-thawed canine ACL model in which the applied high tension was proven to be continuously maintained in the experimental period, Katsuragi et al26 applied a high tension of 20N to the graft model. They demonstrated not only that an unphysiologically high tension significantly deteriorated the mechanical properties of the in situ frozen canine ACL at 12 months after surgery when compared with physiological tension, but also that it provided histological changes in the graft and mild cartilage degeneration at the same period. Namely, in the highly tensioned knee, ovoid and focal degenerative changes with a number of vacuoles were occasionally found in the matrix, and a small part of the articular cartilage surface showed mild softening and fibrillation in each knee, although neither meniscal tears nor tibiofemoral osteophyte formation was found.
On the other hand, Labs et al29 determined the effect of initial graft tension (1N, 7.5N, 17.5N) on the biomechanical and histological behavior of the ACL graft using a rabbit model at 2, 8, and 32 weeks. The load at failure was 40.5% of the normal ACL at 1N, 45.1% at 7.5N, and 50.8% at 17.5N at 32 weeks postoperatively. They stated that higher initial graft tension resulted in improved histological and biomechanical parameters. In addition, pathological changes in the graft or cartilage damage due to overconstraining of the knee were not observed at the selected initial tensions.
In 2003, Abramowitch et al30 performed a goat model study. They investigated whether the differences in knee stability, which were present immediately after ACL reconstruction with grafts fixed at low (5N) and high (35N) initial tension, remained after 6 weeks and whether the tensile properties of an ACL replacement graft were influenced by initial graft tension. Although the high initial graft tension could better replicate the normal knee kinematics at time-zero, these effects diminished during the early graft healing process. Further, the stiffness and ultimate load at failure of the graft were not significantly different between both reconstruction groups.
Randomized Clinical Trials on the Effect of Initial Graft Tension on the Outcome after Anterior Cruciate Ligament Reconstruction
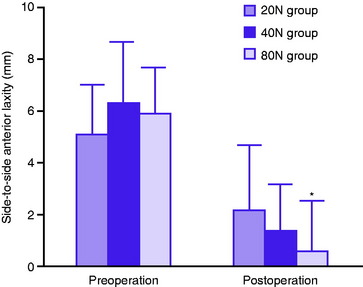
Only four randomized clinical trials have been reported to evaluate the effect of initial graft tension on the outcome after ACL reconstruction. In 1997, Yasuda et al31 reported the first randomized clinical trial using 72 patients. They applied initial tension of 20N, 40N, and 80N to the doubled hamstring tendon graft at 30 degrees of knee flexion and examined clinical outcome at 2 years after ACL reconstruction. The average side-to-side anterior laxity was 2.1, 1.4, and 0.6 mm in the 20N, 40N, and 80N groups, respectively (Fig. 53-4). The postoperative laxity in the 80N group was significantly less than that in the 20N group. All the patients restored full range of knee motion. There were no significant differences in subjective clinical results and muscle strength among the groups. Based on this study, Kim et al32 recently investigated whether initial tension of more than 80N provided any detrimental effects on the knee with hamstring ACL reconstruction, using 48 patients. They applied three different initial tensions of 8, 12, and 15 kg to the hamstring graft at 30 degrees of knee flexion. The patients were observed for 1 year or more after surgery. Postoperatively, the average side-to-side difference in anterior laxity was 1.3 mm in the 8-kg group, 2.1 mm in the 12-kg group, and 2.4 mm in the 15-kg group. The authors stated that there were no significant differences not only in the anterior laxity but also in subjective clinical results and knee extensor strength between the groups. However, we should note that the average laxity value in the 15-kg group was approximately twice as much as that in the 8-kg group. These two studies suggested that relatively high initial tension of approximately 80N reduces the postoperative anterior laxity of the knee joint after ACL reconstruction using the hamstring tendons. Any obvious detrimental effects were noted in these two trials, although long-term results were not known.
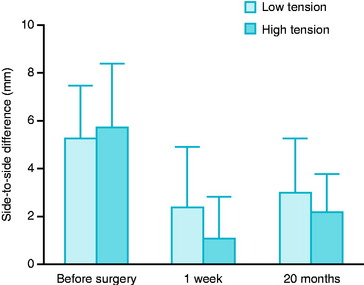
Regarding ACL reconstruction with the BTB graft, van Kampen et al33 reported a randomized trial with 38 patients in 1998. They applied 20N or 40N tension to the BTB graft at 20 degrees of knee flexion and examined clinical outcome at 1 year after surgery. The side-to-side anterior laxity averaged 2.6 mm in the 20N group and 2.5 mm in the 40N group. They found no significant differences. On the other hand, in 2004 Nicholas et al34 reported a randomized trial using 49 patients. They fixed the graft at 45N or 90N at the knee extension position and examined the clinical outcome at an average of 20 months after surgery. The side-to-side anterior laxity difference was significantly greater in the patients in the low-tension group (average 3.0 mm) than in the high-tension group (average 2.2 mm) (Fig. 53-5). The five patients with abnormal anterior tibial displacement (greater than 5 mm side-to-side difference) were only in the low-tension group. The patients regained full range of knee motion. Knee outcome scores and hop test deficits were not different between groups. There is disagreement on the effect of initial graft tension on the knee stability between these two studies on ACL reconstruction with the BTB graft. Nicholas et al34 pointed out that the forces in van Kampen’s study33 were lower than the tensions routinely applied to the BTB graft by experienced surgeons during graft tensioning, that initial graft tension affects the restoration of knee stability, and that a graft tension of 45N was not sufficient for restoring knee stability.
Thus at the present time, no consensus has been reached regarding the amount of graft tension needed to re-create normal knee mechanics after ACL reconstruction using each graft-device combination. However, we have found the following facts on the effect of initial tension in the four clinical studies. Namely, no studies reported that a low tension of less than 40N applied at 0 to 30 degrees of knee flexion was more beneficial to restore the nearly normal stability of the knee in the 1- to 2-year outcome after ACL reconstruction compared with a high tension of greater than 40 N. Also, no studies reported that a relatively high initial tension of approximately 80N, which overconstrained the knee immediately after surgery, provided detrimental effects to the knee function in the 1- to 2-year outcome. For example, the fact that postoperative range of knee motion was clearly not different between the high-tension and low-tension groups in each study demonstrated that the knee is not overconstrained at the follow-up period. It is of note that in the two studies with the hamstring or BTB graft, a relatively high initial tension of 80N or 90N was more beneficial than a relatively low tension of 20N or 45N in restoring the nearly normal stability of the knee in the 1- to 2-year outcome.31,34 This result may support the fact that current ACL reconstruction specialists prefer such degrees of high initial tension.35 According to Nicholas et al,34 two potential mechanisms are considered to explain why high tensions decreased the anterior laxity of the knee. The first potential mechanism is that tension of a ligament tissue reconstructed at the final follow-up examination may be increased depending on the degree of initial graft tension due to the fact that insufficient initial tension may result in slackness of a reconstructed ligament tissue, as the initial graft tension is acutely decreased by various causes.10–1215 The second potential mechanism is that the stiffness and the strength of a reconstructed ligament tissue may be increased depending on the degree of initial graft tension because a low tension significantly reduces the mechanical properties of tendon autograft models.22,23 In the near future, we should be able to determine which mechanism is correct. In addition, further randomized clinical studies are required to reach consensus on this issue.
1 Clancy WG, Nelson DA, Reider B, et al. Anterior cruciate ligament reconstruction using one-third of the patellar ligament, augmented by extra-articular tendon transfers. J Bone Joint Surg. 1982;64A:352-359.
2 Jones KG. Reconstruction of the anterior cruciate ligament: a technique using the central one-third of the patellar ligament. J Bone Joint Surg. 1963;45A:925-932.
3 Noyes FR, Butler DL, Paulos LE, et al. Intra-articular cruciate reconstruction. I: perspectives on graft strength, vascularization, and immediate motion after replacement. Clin Orthop. 1983;172:71-77.
4 Zarins B, Rowe CR. Combined anterior cruciate-ligament reconstruction using semitendinosus tendon and iliotibial tract. J Bone Joint Surg. 1986;68A:160-177.
5 Fleming B, Beynnon BD, Johnson RJ, et al. Isometric versus tension measurements. A comparison for the reconstruction of the anterior cruciate ligament. Am J Sports Med. 1993;21:82-88.
6 Markolf KL, Gorek JF, Kabo JM, et al. Direct measurement of resultant forces in the anterior cruciate ligament. An in vitro study performed with a new experimental technique. J Bone Joint Surg. 1990;72A:557-567.
7 Bylski-Austrow DI, Grood ES, Hefzy MS, et al. Anterior cruciate ligament replacements: a mechanical study of femoral attachment location, flexion angle at tensioning, and initial tension. J Orthop Res. 1990;8:522-531.
8 Fleming BC, Abate JA, Peura GD, et al. The relationship between graft tensioning and the anterior-posterior laxity in the anterior cruciate ligament reconstructed goat knee. J Orthop Res. 2001;19:841-844.
9 Howard ME, Cawley PW, Losse GM, et al. Bone-patellar tendon-bone grafts for anterior cruciate ligament reconstruction: the effects of graft pretensioning. Arthroscopy. 1996;12:287-292.
10 Yamanaka M, Yasuda K, Nakano H, et al. The effect of cyclic displacement upon the biomechanical characteristics of anterior cruciate ligament reconstructions. Am J Sports Med. 1999;27:772-777.
11 Numazaki H, Tohyama H, Yasuda K, et al. The effect of initial graft tension on mechanical behaviors of the femur-graft-tibia complex with anterior cruciate ligament reconstruction during cyclic loading. Am J Sports Med. 2002;30:800-805.
12 Nakano H, Yasuda K, Tohyama H, et al. Interference screw fixation of doubled flexor tendon graft in anterior cruciate ligament reconstruction—biomechanical evaluation with cyclic elongation. Clin Biomech. 2000;15:188-195.
13 Boylan D, Greis PE, West JR, et al. Effects of initial graft tension on knee stability after anterior cruciate ligament reconstruction using hamstring tendons: a cadaver study. Arthroscopy. 2003;19:700-705.
14 Arnold MP, Lie DTT, Verdonschot N, et al. The remains of anterior cruciate ligament graft tension after cyclic knee motion. Am J Sports Med. 2005;33:536-542.
15 Beynnon BD, Johnson RJ, Fleming BC, et al. The measurement of elongation of anterior cruciate-ligament grafts in vivo. J Bone Joint Surg. 1994;76A:520-531.
16 Burks RT, Leland R. Determination of graft tension before fixation in anterior cruciate ligament reconstruction. Arthroscopy. 1988;4:260-266.
17 Melby AIII, Noble JS, Askew MJ, et al. The effects of graft tensioning on the laxity and kinematics of the anterior cruciate ligament reconstructed knee. Arthroscopy. 1991;7:257-266.
18 Gertel TH, Lew WD, Lewis JL, et al. Effect of anterior cruciate ligament graft tensioning direction, magnitude, and flexion angle on knee biomechanics. Am J Sports Med. 1993;21:572-581.
19 Nabors ED, Richmond JC, Vannah WM, et al. Anterior cruciate ligament graft tensioning in full extension. Am J Sports Med. 1995;23:488-492.
20 Graf BK, Henry J, Rothenberg M, et al. Anterior cruciate ligament reconstruction with patellar tendon. An ex vivo study of wear-related damage and failure at the femoral tunnel. Am J Sports Med. 1994;22:131-135.
21 Eagar P, Hull ML, Howell SM. How the fixation method stiffness and initial tension affect anterior load-displacement of the knee and tension in anterior cruciate ligament grafts: a study in cadaveric knees using a double-loop hamstrings graft. J Orthop Res. 2004;22:613-624.
22 Ohno K, Yasuda K, Yamamoto N, et al. Effects of complete stress shielding on the mechanical properties and histology of in situ frozen patellar tendon. J Orthop Res. 1993;11:592-602.
23 Majima T, Yasuda K, Yamamoto N, et al. Deterioration of mechanical properties of the autograft in controlled stress-shielded augmentation procedures. An experimental study with rabbit patellar tendon. Am J Sports Med. 1994;22:821-829.
24 Tsuchida T, Yasuda K, Kaneda K, et al. Effects of in situ freezing and stress-shielding on the ultrastructure of rabbit patellar tendons. J Orthop Res. 1997;15:904-910.
25 Tohyama H, Yasuda K. The effects of stress enhancement on the extracellular matrix and fibroblasts in the patellar tendon. J Biomech. 2000;33:559-565.
26 Katsuragi R, Yasuda K, Tsujino J, et al. The effect of nonphysiologically high initial tension on the mechanical properties of in situ frozen anterior cruciate ligament in a canine model. Am J Sports Med. 2000;28:47-56.
27 Mikami S, Yasuda K, Katsuragi R, et al. Reduction of initial tension in the in situ frozen anterior cruciate ligament. Clin Orthop Relat Res. 2004;419:207-213.
28 Yoshiya S, Andrish JT, Manley MT, et al. Graft tension in anterior cruciate ligament reconstruction: an in vivo study in dogs. Am J Sports Med. 1987;15:464-469.
29 Labs K, Perka C, Schneider F. The biological and biomechanical effect of different graft tensioning in anterior cruciate ligament reconstruction: an experimental study. Arch Orthop Trauma Surg. 2002;122:193-199.
30 Abramowitch SD, Papageorgiou CD, Withrow JD, et al. The effect of initial graft tension on the biomechanical properties of a healing ACL replacement graft: a study in goats. J Orthop Res. 2003;21:708-715.
31 Yasuda K, Tsujino J, Tanabe Y, et al. Effects of initial graft tension on clinical outcome after anterior cruciate ligament reconstruction. Am J Sports Med. 1997;25:99-106.
32 Kim SG, Kurosawa H, Sakuraba K, et al. The effect of initial graft tension on postoperative clinical outcome in anterior cruciate ligament reconstruction with semitendinosus tendon. Arch Orthop Trauma Surg. 2005;28:1-5.
33 van Kampen A, Wymenga AB, van der Heide HJ, et al. The effect of different graft tensioning in anterior cruciate ligament reconstruction: a prospective randomized study. Arthroscopy. 1998;14:845-850.
34 Nicholas SJ, D’Amato MJ, Mullaney MJ, et al. A prospectively randomized double-blind study on the effect of initial graft tension on knee stability after anterior cruciate ligament reconstruction. Am J Sports Med. 2004;32:1881-1886.
35 Cunningham R, West JR, Greis PE, et al. A survey of the tension applied to a doubled hamstring tendon graft for reconstruction of the anterior cruciate ligament. Arthroscopy. 2002;18:983-988.






