[level-membership-for-endocrinology-diabetes-and-metabolism-category]CHAPTER 9
Glucocorticoid-induced osteoporosis
1. How common is glucocorticoid-induced osteoporosis (GIOP)?
Glucocorticoid-induced osteoporosis (GIOP) is the most common cause of secondary osteoporosis. Significant bone loss and skeletal fractures may occur within 6 months of starting glucocorticoid therapy, and up to 50% of people undergoing long-term glucocorticoid treatment have osteoporotic fractures.
2. What are the important determinants of bone loss with glucocorticoid therapy?
Bone loss is related mainly to the dose and the duration of glucocorticoid therapy. Prednisone doses of 7.5 mg or higher (or equivalent doses of other glucocorticoids) are associated with the greatest risk. However, a large cohort study showed a significantly increased fracture risk even in those whose median prednisolone doses had been as low as 2.5 mg daily. Decreased bone mass and increased fracture risk have also been demonstrated with inhaled glucocorticoids.
3. Explain the pathogenesis of GIOP.
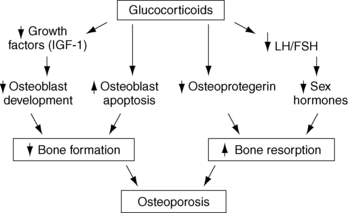
Glucocorticoids adversely affect three phases of bone remodeling. Bone formation is impaired by apoptosis (cell death) of existing osteoblasts and decreased recruitment of new osteoblasts. Glucocorticoids also promote apoptosis of osteocytes, the mechanoreceptors that normally maintain bone strength by coordinating bone remodeling so that older, weaker bone is continuously replaced by newer, stronger bone. Finally, bone resorption is initially increased through various mechanisms, including decreased production of sex steroids and osteoprotegerin, an endogenous inhibitor of bone resorption (Fig. 9-1).
4. What are the BMD criteria for a diagnosis of GIOP?
The ideal bone mineral density (BMD) criteria for the diagnosis of GIOP are still being debated, but the best existing evidence suggests that the fracture risk per BMD decrement is higher in GIOP than in primary osteoporosis. The same BMD criteria are currently used to diagnose osteoporosis in patients taking glucocorticoids as in those who are not taking glucocorticoids, but active treatment should be considered at an earlier stage (T-score ≤ −1.0) because of the rapidity of bone loss in GIOP.
5. In which patients taking glucocorticoids should BMD be tested?
Patients who are starting glucocorticoid therapy (prednisone dose ≥ 5-7.5 mg/day or equivalent) with planned treatment duration of 3 months or longer or who have been receiving treatment for 3 months or longer.
 BMD (spine and hip) should be measured at the initiation of glucocorticoid therapy or as soon as possible thereafter.
BMD (spine and hip) should be measured at the initiation of glucocorticoid therapy or as soon as possible thereafter.
 BMD should be repeated every 6 to 12 months as long as glucocorticoid therapy is continued.
BMD should be repeated every 6 to 12 months as long as glucocorticoid therapy is continued.
7. What measures should be instituted in all patients taking glucocorticoids?
All glucocorticoid-treated patients should be advised to consume adequate calcium (1200-1500 mg daily; combination of dietary intake plus supplements) and vitamin D (800-1200 U/day), to exercise regularly (aerobic and resistance), to stop smoking, and to limit alcohol and caffeine consumption.
8. Who should be considered for pharmacologic therapy?
The American College of Rheumatology (ACR) recommends pharmacologic therapy for anyone who will receive or has received ≥ 7.5 mg/day of prednisone (or equivalent) for at least 3 months but recommends therapy for high-risk patients undergoing glucocorticoid therapy of any dose or duration. The National Osteoporosis Foundation recommends therapy for anyone who will receive or has received ≥ 5 mg/day of prednisone (or equivalent) for at least 3 months.
9. Which medications are effective in preventing and treating GIOP?
Bisphosphonates increase bone mass and prevent fractures in patients with GIOP. Alendronate, risedronate, and zoledronic acid are all approved by the U.S. Food and Drug Administration (FDA) for this disorder. In a randomized controlled trial, teriparatide was reported to increase bone density more than alendronate and to reduce fractures by 90% in patients with GIOP. The ACR currently recommends bisphosphonates as first-line therapy, with teriparatide reserved for those at highest risk or in whom bisphosphonate therapy fails. Denosumab is a potentially effective option but is not yet approved by the FDA for this condition. The dose regimens for these agents are discussed in the chapter on osteoporosis (see Chapter 8).
10. When should gonadal steroids be considered?
Gonadal steroids may be considered, usually in combination with other agents, in postmenopausal women and hypogonadal men (men with low serum testosterone).
 KEY POINTS 1: PREVALENCE AND PATHOPHYSIOLOGY OF GIOP
KEY POINTS 1: PREVALENCE AND PATHOPHYSIOLOGY OF GIOP
1. Glucocorticoid-induced osteoporosis is the most common type of secondary osteoporosis.
2. High doses and prolonged use of glucocorticoids produce greater risk, but all doses of oral glucocorticoids and even inhaled steroids increase the risk of osteoporotic fractures.
3. Glucocorticoid-induced osteoporosis results from suppressed bone formation, impaired osteocyte function, and enhanced bone resorption, accounting for the rapid bone loss and disproportionately low bone strength seen in glucocorticoid-treated patients.
 KEY POINTS 2: PREVENTION AND TREATMENT OF GIOP
KEY POINTS 2: PREVENTION AND TREATMENT OF GIOP
1. Bone mineral density (BMD) testing is recommended before initiation of glucocorticoid therapy in patients who will receive ≥ 5 to 7.5 mg/day of prednisone (or equivalent) for ≥ 3 months, duration and every 6 to 12 months thereafter as long as glucocorticoid therapy is continued.
2. The American College of Rheumatology recommends treatment for all patients who will be treated or have been treated with ≥ 7.5 mg/day of prednisone (or equivalent) for ≥ 3 months. The National Osteoporosis Foundation recommends treatment at ≥ 5 mg daily of prednisone.
3. Bisphosphonates are recommended as first-line agents for GIOP, and teriparatide is usually reserved for the highest risk patients or those in whom bisphosphonate therapy fails.
Adachi, JD, Olszynski, WP, Hanley, DA, et al. Management of corticosteroid-induced osteoporosis. Semin Arthritis Rheum. 2000;29:228–251.
Amin, S, LaValley, MP, Simms, RW, et al, The comparative efficacy of drug therapies used for the management of corticosteroid-induced osteoporosis. a meta-regression. J Bone Miner Res 2002;17:1512–1526.
Canalis, E. Glucocorticoid-induced osteoporosis. Curr Opin Endocrinol Diabetes. 2000;7:320–324.
Devogelaer, JP, Glucocorticoid-induced osteoporosis. mechanisms and therapeutic approach. Rheum Dis Clin North Am 2006;32:733–756.
Gourlay, M, Franceschini, N, Sheyn, Y. Prevention and treatment strategies for glucocorticoid induced osteoporotic fractures. Clin Rheumatol. 2007;26:144–153.
Grossman, JM, Gordon, R, Ranganath, VK, et al. American College of Rheumatology 2010. Recommendations for the prevention and treatment of glucocorticoid-induced osteoporosis. Arthritis Care Res (Hoboken). 2010;62:1515–1526.
Hanson, KE, Wilson, HA, Zapalowski, C, et al. Uncertainties in the prevention and treatment of glucocorticoid-induced osteoporosis. J Bone Min Res. 2011;26:1989–1996.
Isreal, E, Banerjee, TR, Fitzmaurice, GM, et al. Effects of inhaled glucocorticoids on bone density in premenopausal women. N Engl J Med. 2001;345:941–947.
Rubin, MR, Bilezikian, JP, The role of parathyroid hormone in the pathogenesis of glucocorticoid-induced osteoporosis. a re-examination of the evidence. J Clin Endocrinol Metab 2002;87:4033–4041.
Saag, KG, Shane, E, Boonen, S, et al. Teriparatide or alendronate in glucocorticoid-induced osteoporosis. N Engl J Med. 2007;357:2028–2039.
Sambrook, PN. How to prevent steroid induced osteoporosis. Ann Rheum Dis. 2007;64:176–178.
Van Staa, TP, Leufkens, HGM, Abenhaim, L, et al. Use of oral corticosteroids and risk of fractures. J Bone Miner Res. 2000;15:993–1000.
Van Staa, TP, Leufkens, HGM, Cooper, C. Use of inhaled corticosteroids and risk of fractures. J Bone Miner Res. 2001;16:581–588.
Weinstein, RS. Glucocorticoid induced bone loss. N Engl J Med. 2011;365:62–70.
[/level-membership-for-endocrinology-diabetes-and-metabolism-category][not-level-membership-for-endocrinology-diabetes-and-metabolism-category]CHAPTER 9
Glucocorticoid-induced osteoporosis
1. How common is glucocorticoid-induced osteoporosis (GIOP)?
Glucocorticoid-induced osteoporosis (GIOP) is the most common cause of secondary osteoporosis. Significant bone loss and skeletal fractures may occur within 6 months of starting glucocorticoid therapy, and up to 50% of people undergoing long-term glucocorticoid treatment have osteoporotic fractures.
2. What are the important determinants of bone loss with glucocorticoid therapy?
Bone loss is related mainly to the dose and the duration of glucocorticoid therapy. Prednisone doses of 7.5 mg or higher (or equivalent doses of other glucocorticoids) are associated with the greatest risk. However, a large cohort study showed a significantly increased fracture risk even in those whose median prednisolone doses had been as low as 2.5 mg daily. Decreased bone mass and increased fracture risk have also been demonstrated with inhaled glucocorticoids.
3. Explain the pathogenesis of GIOP.
Glucocorticoids adversely affect three phases of bone remodeling. Bone formation is impaired by apoptosis (cell death) of existing osteoblasts and decreased recruitment of new osteoblasts. Glucocorticoids also promote apoptosis of osteocytes, the mechanoreceptors that normally maintain bone strength by coordinating bone remodeling so that older, weaker bone is continuously replaced by newer, stronger bone. Finally, bone resorption is initially increased through various mechanisms, including decreased production of sex steroids and osteoprotegerin, an endogenous inhibitor of bone resorption (Fig. 9-1).
4. What are the BMD criteria for a diagnosis of GIOP?
The ideal bone mineral density (BMD) criteria for the diagnosis of GIOP are still being debated, but the best existing evidence suggests that the fracture risk per BMD decrement is higher in GIOP than in primary osteoporosis. The same BMD criteria are currently used to diagnose osteoporosis in patients taking glucocorticoids as in those who are not taking glucocorticoids, but active treatment should be considered at an earlier stage (T-score ≤ −1.0) because of the rapidity of bone loss in GIOP.
5. In which patients taking glucocorticoids should BMD be tested?
Patients who are starting glucocorticoid therapy (prednisone dose ≥ 5-7.5 mg/day or equivalent) with planned treatment duration of 3 months or longer or who have been receiving treatment for 3 months or longer.
[/not-level-membership-for-endocrinology-diabetes-and-metabolism-category]
