Chapter 1 General Appearance, Facies, and Body Habitus
General Appearance
2 Which aspects of the patient should be assessed?












A. Posture
3 What information can be obtained from observing the patient’s posture?
In abdominal pain the posture is often so typical as to localize the disease:
 Patients with pancreatitis usually lie in the fetal position: on one side, with knees and legs bent over.
Patients with pancreatitis usually lie in the fetal position: on one side, with knees and legs bent over.
 Patients with peritonitis are very still and avoid any movement that might worsen the pain.
Patients with peritonitis are very still and avoid any movement that might worsen the pain.
 Patients with intestinal obstruction are instead quite restless.
Patients with intestinal obstruction are instead quite restless.
 Patients with renal or perirenal abscesses bend toward the side of the lesion.
Patients with renal or perirenal abscesses bend toward the side of the lesion.


 Patients with a large pleural effusion tend to lie on the affected side to maximize excursions of the unaffected side. This, however, worsens hypoxemia (see Chapter 13, questions 48–51).
Patients with a large pleural effusion tend to lie on the affected side to maximize excursions of the unaffected side. This, however, worsens hypoxemia (see Chapter 13, questions 48–51).



4 What is the posture of patients with dyspnea?
An informative alphabet soup of orthopnea, paroxysmal nocturnal dyspnea, platypnea and orthodeoxia, trepopnea, respiratory alternans, and abdominal paradox. These can determine not only the severity of dyspnea, but also its etiology (see Chapter 13, questions 35–51).
B. State of Hydration
5 What is hypovolemia?
A condition characterized by volume depletion and dehydration:
 Volume depletion is a loss in extracellular salt, through either kidneys (diuresis) or the gastrointestinal tract (hemorrhage, vomiting, diarrhea). This causes contraction of the total intravascular pool of plasma, which results in circulatory instability and thus an increase in the serum urea nitrogen-to-creatinine ratio—a valuable biochemical marker for volume depletion.
Volume depletion is a loss in extracellular salt, through either kidneys (diuresis) or the gastrointestinal tract (hemorrhage, vomiting, diarrhea). This causes contraction of the total intravascular pool of plasma, which results in circulatory instability and thus an increase in the serum urea nitrogen-to-creatinine ratio—a valuable biochemical marker for volume depletion.



9 How do you determine the presence of hypovolemia?
Through the “tilt test,” which measures postural changes in heart rate and blood pressure (BP):
1. Ask the patient to lie supine.
3. Measure heart rate and blood pressure in this position.
6. Measure heart rate and then blood pressure while the patient is standing. Measure rate by counting over 30 seconds and multiplying by two, which is more accurate than counting over 15 seconds and multiplying by four.
12 Should the patient lie supine for more than 2 minutes before standing up?
No. A longer period does not increase the sensitivity of the test.
14 What is the normal response to the tilt test?
Going from supine to standing, a normal patient exhibits the following:



18 So what are the findings of a positive tilt test for hypovolemia?








29 What is the significance of dry mucous membranes in children?



C. State of Nutrition
33 Why is the BMI important?
Because a high BMI is associated with increased risk for serious medical problems:










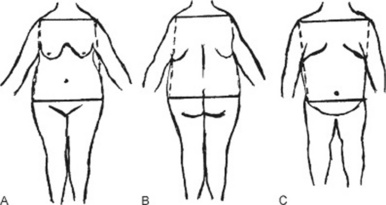
38 How important is the distribution of body fat?
Very important, since it strongly determines the impact of obesity on health. Fat deposition may be central (mostly in the trunk) or peripheral (mostly in the extremities) (Fig. 1-1).


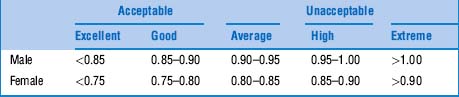
42 What is the WHR threshold for cardiovascular risk?
The cutoff seems to be a waist-to-hip ratio of 0.83 for women and 0.9 for men. Favoring WHR over BMI would result in a threefold increase in the population at risk for myocardial infarction. This would be especially valuable in Asia, where obesity by BMI is rare, but WHRs can be quite abnormal (Table 1-1).



48 What are the physical examination components of the SGA?
 The best locations for assessing subcutaneous fat are the triceps regions of the arms, the midaxillary line at the costal margin, the interosseous and palmar areas of the hand, and the deltoids of the shoulder. Loss of subcutaneous fat appears as lack of fullness, with skin loosely fitting over the deeper tissues.
The best locations for assessing subcutaneous fat are the triceps regions of the arms, the midaxillary line at the costal margin, the interosseous and palmar areas of the hand, and the deltoids of the shoulder. Loss of subcutaneous fat appears as lack of fullness, with skin loosely fitting over the deeper tissues.






D. Facies
51 Which disease processes are associated with a typical facies?
Quite a few. The following list is not necessarily exhaustive (Table 1-2):
 Facies bovina: The cowlike face of Greig’s syndrome: large cranial vault, huge forehead, high bregma, and occasional hypertelorism (widely spaced eyes)—all due to an enlarged sphenoid bone. It is often associated with other congenital deformities, such as osteogenesis imperfecta, syndactyly and polydactyly, Sprengel’s deformity (scapular elevation), and mental retardation.
Facies bovina: The cowlike face of Greig’s syndrome: large cranial vault, huge forehead, high bregma, and occasional hypertelorism (widely spaced eyes)—all due to an enlarged sphenoid bone. It is often associated with other congenital deformities, such as osteogenesis imperfecta, syndactyly and polydactyly, Sprengel’s deformity (scapular elevation), and mental retardation.







 Facies antonina: Another face of leprosy, with alterations in the eyelids and the anterior eye.
Facies antonina: Another face of leprosy, with alterations in the eyelids and the anterior eye.




 Graves’ face: A typical and anxious-looking face, with exophthalmos and lid lag.
Graves’ face: A typical and anxious-looking face, with exophthalmos and lid lag.



 Facies of lupus erythematosus: Malar and butterfly-like rash across the bridge of the nose.
Facies of lupus erythematosus: Malar and butterfly-like rash across the bridge of the nose.
 Aortic face: The pale and sallow face of early aortic regurgitation (AR).
Aortic face: The pale and sallow face of early aortic regurgitation (AR).



 Parkinson’s face: The mask-like facies of Parkinson’s. It has a fixed and apathetic look.
Parkinson’s face: The mask-like facies of Parkinson’s. It has a fixed and apathetic look.










Table 1-2 Disease Processes Associated with a Typical Facies
| Etiology | Facies | Disease |
|---|---|---|
| Congenital | Facies bovina | Greig’s syndrome |
| Elfin face | Williams’ syndrome | |
| Cherubic face | Cherubism | |
| Hound-dog face | Cutis laxa | |
| Hurloid face | Hurler’s syndrome | |
| Morquio’s face | Morquio’s syndrome | |
| Potter’s face | Potter’s syndrome | |
| Infectious | Facies leonina | Leprosy |
| Facies antonina | Leprosy | |
| Scaphoid face | Leprosy | |
| Tetanus face | Tetanus | |
| Endocrine-metabolic | Renal face | Chronic renal failure |
| Myxedematous face | Myxedema | |
| Graves’ face | Graves’ disease | |
| Acromegalic face | Acromegaly | |
| Cushing’s face | Cushing’s syndrome | |
| Rheumatologic | Scleroderma face | Progressive systemic sclerosis |
| Lupus face | Systemic lupus erythematosus | |
| Cardiovascular | Aortic face | Aortic regurgitation |
| Corvisart’s face | Aortic regurgitation | |
| De Musset’s face | Aortic regurgitation | |
| Mitral face | Mitral stenosis | |
| Neurologic | Parkinson’s face | Parkinson’s disease |
| Steinert’s face | Myotonic dystrophy | |
| Myasthenic face | Myasthenia gravis | |
| Myopathic face | Various | |
| Traumatic | Battle’s sign | Basilar skull fracture |
| Raccoon eyes | ||
| Miscellaneous | Hippocratic face | Terminal illness |
| Facies adenoid | Adenoids/chronic allergic rhinitis | |
| Rhinophyma | Various | |
| Saddle nose | Congenital syphilis/Wegener’s/polychondritis | |
| Smoker’s face | Tobacco |
E. Apparent Age
57 Which conditions make you look younger than your stated age?





F. Gait
65 How are stance and gait coordinated?





66 What are the two physiologic requirements of walking?


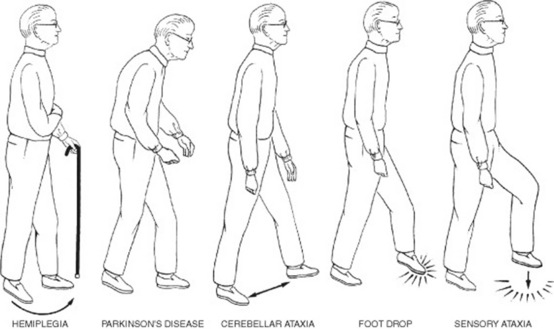
68 What are the four most common reasons for gait disturbance?




To separate them, always notice whether the disturbance is symmetric (suggesting faulty neurologic control, except for the spasticity of hemiplegia) or asymmetric (suggesting instead pain, a fixed joint, or muscle weakness) (Fig. 1-2 and Table 1-3).
| Mechanism | Gait Disturbance | Disease |
|---|---|---|
| Pain | Antalgic gait | Osteoarthritis hip, knee, ankle |
| Immobile joint | Fixed joint gait | Osteoarthritis; prolonged periods of plaster immobilization |
| Muscle weakness | Trendelenburg gait | Unilateral weakness of hip abductors |
| Anserine gait | Bilateral weakness of hip abductors | |
| High steppage gait | Weakness of hip abductors | |
| Charcot-Marie-Tooth disease | ||
| Foot drop (peroneal paralysis) | ||
| Abnormal neurologic control | Gait of spinal stenosis | Myelopathy (cervical spondylosis) |
| Gait of spastic paraplegia | Scissor gait | |
| Ataxic gait/cerebellar gait | Ataxia (sensory or cerebellar) | |
| Apraxic gait | Apraxia (frontal lobe disease) | |
| Hemiplegic gait | Hemispheric stroke | |
| Parkinsonian gait | Parkinson’s disease |
69 What historic information should be gathered to adequately evaluate an abnormal gait?
In addition to symmetry versus asymmetry (previously discussed), one should inquire about:
 Acute onset (usually suggesting vascular disease versus drugs: alcohol, benzodiazepines, neuroleptics, and agents causing orthostatic hypotension)
Acute onset (usually suggesting vascular disease versus drugs: alcohol, benzodiazepines, neuroleptics, and agents causing orthostatic hypotension)

 Presence of stiffness in the limbs
Presence of stiffness in the limbs
 Difficulty in initiating or terminating walking
Difficulty in initiating or terminating walking
 Presence of bladder or bowel dysfunction
Presence of bladder or bowel dysfunction
 Association with vertigo or light-headedness
Association with vertigo or light-headedness


71 How should one observe a patient with a gait abnormality?
By closely evaluating (from front, back, and side):
 How the patient gets up from a chair (useful in Parkinson’s or limb girdle dystrophy)
How the patient gets up from a chair (useful in Parkinson’s or limb girdle dystrophy)
 How the patient initiates walking (also useful in Parkinson’s)
How the patient initiates walking (also useful in Parkinson’s)
 How the patient walks at a slow pace
How the patient walks at a slow pace
 How the patient walks at a fast pace
How the patient walks at a fast pace


 How the patient walks on heels (diagnostic in motor ataxia, spastic paraplegia, or foot drop)
How the patient walks on heels (diagnostic in motor ataxia, spastic paraplegia, or foot drop)
 How the patient walks a straight line in tandem (i.e., heel to toe) (useful in all gait disorders)
How the patient walks a straight line in tandem (i.e., heel to toe) (useful in all gait disorders)

 How the patient stands erect with eyes first open and then closed (Romberg’s)
How the patient stands erect with eyes first open and then closed (Romberg’s)




(1) Gait Disturbances Due to Pain



(2) Gait Disturbances Due to Immobile Joints
(3) Gait Disturbances Due to Muscle Weakness
75 What is the most common gait abnormality due to muscle weakness?
The one resulting from weak hip abductors (gluteus medius and minimus).




80 Describe the gait of “foot drop.”
 High steppage: This consists of knees raised unusually high to allow the drooping foot to clear the ground. And yet, since the toes of the lifted foot remain pointed downward, they may still scrape the floor, thus resulting in frequent stumbles and falls. A foot drop can often be diagnosed by simply looking at the patient’s shoes, since wears and tears will be typically asymmetric, especially affecting the toes.
High steppage: This consists of knees raised unusually high to allow the drooping foot to clear the ground. And yet, since the toes of the lifted foot remain pointed downward, they may still scrape the floor, thus resulting in frequent stumbles and falls. A foot drop can often be diagnosed by simply looking at the patient’s shoes, since wears and tears will be typically asymmetric, especially affecting the toes.

(4) Gait Disturbances Due to Abnormal Neurologic Control
88 Describe the gait of spastic paraplegia.
With hips adducted and internally rotated (so that thighs rub together), and legs slightly flexed at the hips and knees. Overall, patients appear to be crouching. Because of their excessive adduction, legs are unable to move straight forward. Instead, they swing across each other in a typical criss-cross motion at the knees (“scissor gait”). Since ankles are plantarflexed, patients walk on tiptoe, with feet scraping the floor (and soles becoming typically worn along the toes). To compensate for the stiff movement of the legs, patients may move the trunk from side to side. For an illustration of the gait of spastic paraplegia, go to http://web.macam98.ac.il/∼shayke/hebrew/ppt/adaptask/adaptation/walk.htm.
98 What is a Parkinsonian gait?




1 Baraff LJ, Schriger DL. Orthostatic vital signs: Variation with age, specificity, and sensitivity in detecting a 450-mL blood loss. Ann Emerg Med. 1992;10:99-103.
2 Bergenwald L, Freyschuss U, Sjostrand T. The mechanism of orthostatic and haemorrhage fainting. Scand Clin Lab Invest. 1977;37:209-216.
3 Detsky AS, Smalley PS, Chang J. The rational clinical examination. Is this patient malnourished? JAMA. 1994;271:54-58.
4 Eaton D, Bannister P, Mulley GP, Conolly MJ. Axillary sweating in clinical assessment of dehydration in ill elderly patients. BMJ. 1994;308:1271.
5 Ebert RV, Stead EA, Gibson JG. Response of normal subjects to acute blood loss. Arch Intern Med. 1941;68:578-590.
6 Eisner LS. Diagnosing Gait Disorders (videotape). Secaucus, NJ: Continuing Medical Education, 1987.
7 Green DM, Metheny D. The estimation of acute blood loss by the tilt test. Surg Gynecol Obstet. 1947;84:1045-1050.
8 Gross CR, Lindquist RD, Woolley AC, et al. Clinical indicators of dehydration severity in elderly patients. J Emerg Med. 1992;10:267-274.
9 Janssen I, Katzmarzyk PT, Ross R. Body mass index, waist circumference, and health risk. Arch Intern Med. 2002;162:2074-2079.
10 Knepp R, Claypool R, Leonardi D. Use of the tilt test in measuring acute blood loss. Ann Emerg Med. 1980;9:72-75.
11 McGee S, Abernathy WB3rd, Simel DL. Is this patient hypovolemic? JAMA. 1999;281:1022-1029.
12 McGee S. Evidence-Based Physical Diagnosis. Philadelphia: W.B. Saunders, 2001.
13 Ralston LA, Cobb LA, Bruce RA. Acute circulatory effects of arterial bleeding as determined by indicator-dilution curves in normal human subjects. Am Heart J. 1961;61:770-776.
14 Sapira JD. The Art and Science of Bedside Diagnosis. Baltimore: Urban & Shwarzenberg, 1990.
15 Shenkin HA, Cheney RH, Govons SR, et al. On the diagnosis of hemorrhage in man. Am J Med Sci. 1944;208:421-436.
16 Skillman JJ, Olson JE, Lyons JH, et al. The hemodynamic effect of acute blood loss in normal man, with observations on the effect of the Valsalva maneuver and breath holding. Ann Surg. 1967;166:713-738.
17 Wahrenberg H, Hertel K, Leijonhufvud BM, et al. Use of waist circumference to predict insulin resistance: Retrospective study. BMJ. 2005;330:1363-1364.
18 Wallace J, Sharpey-Schafer EP. Blood changes following controlled haemorrhage in man. Lancet. 1941;241:393-395.
19 Warren JV, Brannon ES, Stead EAJr, et al. The effect of venesection and the pooling of blood in the extremities on the atrial pressure and cardiac output in normal subjects with observations on acute circulatory collapse in three instances. J Clin Invest. 1945;24:337-344.
20 Willis JL, Schneiderman H, Algranati PS. Physical Diagnosis. Baltimore: Williams and Wilkins, 1994.
21 Witting MD, Wears RL, Li S. Defining the positive tilt test. Ann Emerg Med. 1994;23:1320-1323.



