[level-membership-for-orthopaedics-category]
Chapter 18 Gender Differences in Muscular Protection of the Knee
PROPRIOCEPTION
Proprioception refers to an individual’s awareness of joint and body movement and their position in space. Motor control feedback via the gamma motor system can modify muscle stiffness or transjoint resistance of muscles to control joint movement and positioning during planned and unexpected events. Therefore, skeletal muscle plays an important role in knee joint proprioception. An individual’s ability to detect knee joint position and motion is a major component required for reflex response, allowing joint stabilization and protection to develop. When errors in these systems occur, or when these systems function at suboptimal levels, increased ligament strain, articular cartilage shear, and/or bone impact may result. High risk positioning of the lower extremity may also occur.13,20
Several authors have reported gender differences in proprioception.21,39,40,53 Rozzi and coworkers40 investigated joint proprioception in 34 (17 male, 17 female) collegiate soccer and basketball athletes by measuring the threshold to detection of passive motion using a device that moved the knee joint at a constant 0.5°/sec velocity through flexion and extension. A rotational transducer provided angular displacement values. Compared with male athletes, females took significantly longer to detect the threshold of knee joint motion in extension (2.11° ± 0.63° and 2.95° ± 1.47°, respectively; P = .039). However, no significant gender difference was observed during flexion. The clinical significance of a mean difference of 0.84° of angular motion between genders is unknown.
Hewett and associates21 assessed proprioception using single-leg postural balance at the knee on a dynamic platform in ACL-deficient subjects. Uninjured females demonstrated greater knee joint stability than males, which the authors attributed to a lower center of gravity. In contrast, males had significantly greater single-leg stability after an ACL rupture, and females took longer to regain adequate levels of single-leg balance postoperatively.21 A clear gender difference cannot be extracted from these results.
Although injury research often focuses on the lower limbs, the core of the torso may be the key to understanding body positioning. Therefore, the core muscle of the torso should not be overlooked in the investigation of proprioception. Zazulak and colleagues53 evaluated core proprioception and knee joint control. Two-hundred seventy-seven collegiate athletes (137 male, 140 female) underwent core proprioceptive measurements by passive trunk rotation in the seated position through 20° in the transverse plane. With auditory and visual stimuli diminished, the athletes were instructed to reproduce the initial position after displacement. The difference between the perceived and the actual angle was calculated as the active proprioceptive repositioning error. After testing, the athletes were followed for 3 years, during which 25 (14 male, 11 female) sustained knee injuries. Analysis of the active proprioceptive repositioning error revealed that females who sustained knee ligament or meniscal injuries demonstrated significantly greater error in active repositioning than uninjured females. Male athletes did not demonstrate this problem. In addition, uninjured female athletes had significantly better core proprioception than uninjured male athletes, which supports previous studies.20,40 Zazulak and coworkers52 also reported that after an unexpected perturbation, the maximal trunk displacement in females who suffered knee ligament injuries was significantly greater than that of females who did not experience injury. No significant difference in maximal trunk displacement between injured and uninjured males was found. Therefore, the core stability of female athletes may be a greater factor in lower extremity injury susceptibility than that in males.52 In fact, lateral trunk displacement was the lone significant predictor of ligament injury in female athletes (P = .001) in this investigation, with 100% sensitivity and 72% specificity rates reported. This was not true for male athletes, because their sole predictor of injury was a history of low back pain.52
Other factors that may influence proprioceptive function include joint laxity and muscle fatigue, both of which also affect muscle function. Rozzi and associates39 reported that female athletes had greater knee laxity that resulted in a decreased sensitivity to knee position change. Many clinicians have suspected that joint laxity is a risk factor for knee injury, but the evidence is not overwhelming. The best evidence may be that provided by Uhorchak and colleagues43 in their risk factor analysis for ACL injury in military cadets.
Regarding muscle fatigue, Rozzi and associates39 showed in male and female collegiate basketball and soccer athletes that induced fatigue altered proprioception, especially in knee extension. Wojtys and coworkers51 evaluated the effects of muscle fatigue on anterior tibial translation, muscle reaction time, and recruitment order in 10 athletes (6 male, 4 female) whose physical activity included jumping, pivoting, and twisting. Each athlete completed baseline measurements and then underwent a vigorous isokinetic workout until quadriceps and hamstrings torques decreased by 50% or greater. Eight of the 10 fatigued athletes demonstrated greater anterior tibial translation during dynamic testing (average percentage increase, 32.5%), indicating that fatigue did increase joint laxity. Fatigued athletes did not alter their muscle recruitment order in response to an anterior tibial translation. However, after fatigue, muscle reaction time slowed significantly in the three response phases (spinal reflex, intermediate, and voluntary). Although the investigation found a change in muscle reaction time and laxity of the knee, no gender difference was reported for these factors, nor was a correlation established between fatigue and a decrease in proprioception.
Earlier studies have evaluated the effect of ACL-deficiency on proprioception, although gender was not specifically examined.6,11,48 More recent studies have focused on gender differences. In general, these studies show that injured female athletes have poorer lower extremity proprioception than their male athlete counterparts.21,40,52 However, uninjured female athletes tend to have higher levels of stability than healthy male athletes.
Considering the consequences of serious knee injury, proprioceptive prescreening of female athletes, especially in high-risk sports, prior to athletic participation may help focus training and conditioning programs.20,52,53
MUSCLE RESPONSE
Time to Peak Torque
Neuromuscular activation patterns influence dynamic knee joint stability potential, which may contribute to knee injury susceptibility.10,19,23,25 Gender-related differences in these activation patterns have been reported by numerous investigators.8,10,27,33,40,41,44,47
Using isokinetic peak torque strength testing of 100 Division I athletes (60 male, 40 female), Huston and Wojtys27 detected significant gender differences. Female athletes and controls generated similar time to peak knee flexion torques, which were slower than male athletes. Male athletes were able to generate peak knee extension and flexion torques faster than male or female controls (Table 18-1). The slowed response of the hamstring in females was most striking.
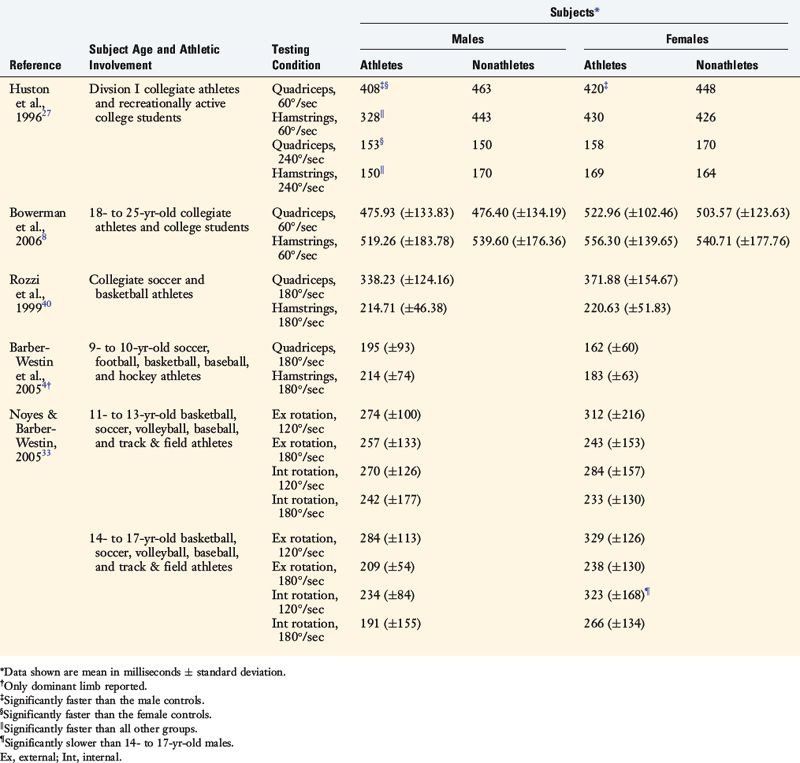
Considering the young age at which many ACL injuries occur, muscle function maturation should be considered in the evaluation of injury susceptibility. Noyes and Barber-Westin33 examined the gender- and age-related differences in time to peak torque for internal and external tibial rotation with isokinetic strength testing. They separated 94 athletes into two age groups: 11 to 13 years of age (20 male, 20 female) and 14 to 17 years of age (27 male, 27 female). Older male athletes were faster (28%) in internal rotation peak torque of the hamstrings than age-matched female athletes (see Table 18-1). In contrast, multiple investigators have reported no gender differences in isokinetic peak torques for quadriceps and/or hamstrings in collegiate athletes,8,40 nonathlete controls,8 and athletes 13 years of age or younger4,33 (see Table 18-1).
Muscle Reaction Time
In an attempt to identify more relevant functional gender differences, several investigators have assessed peak muscle torque during weight-bearing perturbations and athletic tasks. Shultz and associates41 examined muscle response times in 64 collegiate lacrosse and soccer athletes (32 male, 32 female) after applying an unexpected rotational perturbation force to the lower extremity. Female athletes’ muscle response times for the quadriceps muscles were faster than male athletes with comparable recruitment patterns (Table 18-2). The Division I collegiate athletes displayed faster muscle response times than the recreational athletes.
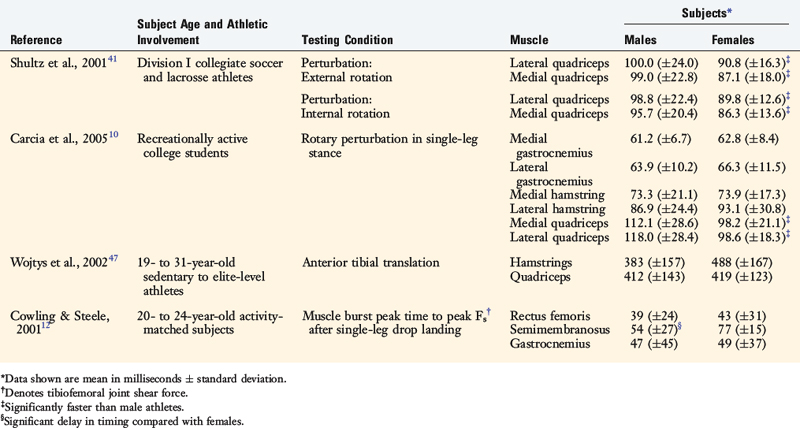
Carcia and colleagues10 measured the response times of the quadriceps, hamstrings, and gastrocnemius muscles after a weight-bearing rotary perturbation in 20 recreationally active adults (10 male, 10 female). Males and females responded with similar muscle recruitment order patterns at various angles of flexion (10°, 20°, 30°), and females generated faster quadriceps muscle response times than males at all angles (see Table 18-2).
Using a posterior force to the calf muscle to simulate anterior tibial translation, Huston and Wojtys27 reported that female athletes activated their quadriceps first and faster than their male counterparts, raising concerns about what role the quadriceps could directly play in ACL injuries. In contrast, Cowling and Steele12 reported a delay in the semimembranosus (hamstring) muscle of male athletes during abrupt single-leg landing compared with athletic level–matched female athletes.
In summary, preferential quadriceps activation and a slowed hamstring response may lead to a neuromuscular imbalance producing ineffective knee stabilization.10,27,41,49 Powerful or unopposed quadriceps contractions, especially close to knee extension, have the potential to cause ACL injury.46 Further research is necessary to better understand these relationships, especially in terms of muscle activity mode injury rates.
Strength
The timely ability to generate high levels of muscle force across the knee joint may decrease functional joint laxity and result in less stress and strain on the passive structures that constrain knee motion.7,8,15,16,27,47,49 A poor muscle strength–to–body weight ratio may be a risk factor for lower extremity injury.30,43
Besides the peak torque–to–body weight ratio, the balance of forces expressed as the hamstring-to-quadriceps (H:Q) ratio is an additional performance measurement that may provide insight into the gender differences in injury susceptibility. Evidence suggests that the hamstring muscles have the potential to unload the ACL,46 whereas the quadriceps appear to function as the ACL antagonist.46 The suspected relationship between the H:Q peak torque ratio and ACL injury susceptibility has been investigated by several authors.2,8,9,22,38 This factor may be critical in ACL protection.2,4,5,8,9,22,38,49
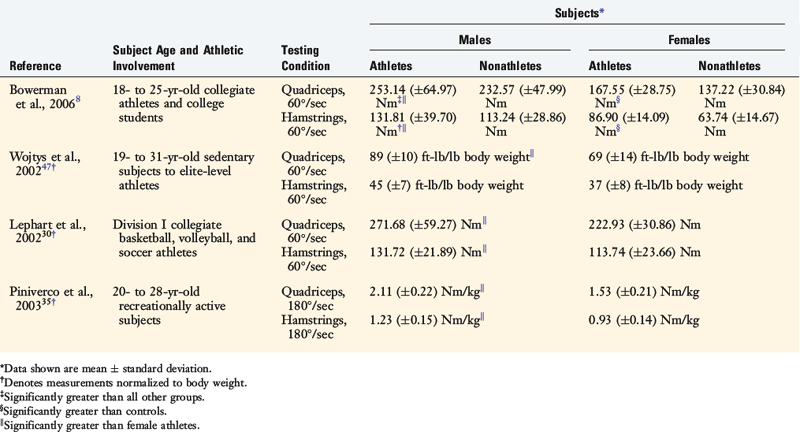
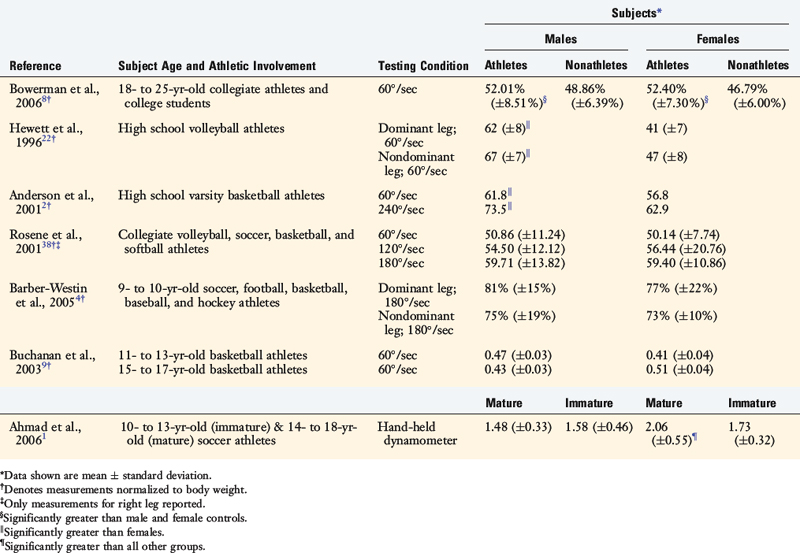
Bowerman and coworkers8 tested the peak isokinetic muscle torque (60°/sec) of 54 healthy collegiate athletes and 53 age-matched nonathletes. Males were stronger than females for both quadriceps and hamstring muscles (Table 18-3). Unfortunately, measurements were not normalized to body weight in this study. Not surprisingly, athletes generated higher quadriceps and hamstring peak torques. Similar findings were reported by Wojtys and associates47 in 23 healthy volunteers (10 male, 13 female) whose activity level ranged from sedentary to elite-level athletes. Lephart and colleagues30 also reported similar results, as did Bowerman and coworkers8 in 15 Division I collegiate athletes and 15 age-matched male controls under the same testing conditions after normalizing for body weight (see Table 18-3). Male recreational athletes generated greater quadriceps and hamstring peak isokinetic torques (180°/sec) than their female counterparts with body weight normalization.35 In addition, Hewett and coworkers22 and Anderson and associates2 reported that female high school athletes had lower H:Q ratios than male athletes. Conversely, Bowerman and coworkers8 and Rosene and colleagues38 found no gender difference in H:Q ratios among collegiate soccer, volleyball, softball, basketball, football, tennis, and track athletes. However, their strength levels were not corrected for body weight (Table 18-4).
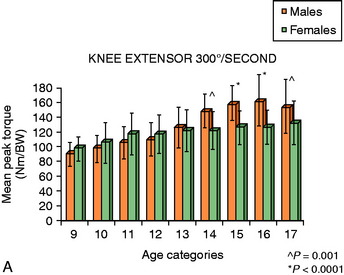
Related studies have focused on the progression of muscle strength through adolescence to maturity. Barber-Westin and coworkers5 reported isokinetic muscle strength data (300°/sec normalized to body weight) on 1140 athletes (177 male, 853 female), ranging in age from 9 to 17 years. An increase in the mean knee extension peak torque was seen for both male and female subjects with maturation (Fig. 18-1A). At age 13 years, females produced 20% more extension peak torque than at age 9, but failed to produce a difference after age 13. Similarly, males at age 14 years produced 38% more extension peak torque than at age 9 with no difference found after age 14. There was no gender difference in the peak extension torque mean until the age of 14, when male athletes surpassed the females.
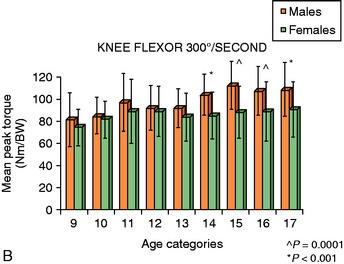
Male athletes demonstrated an increase in mean knee flexion peak torque (23%) from age 9 to 14 years, whereas female athletes produced a much smaller increase (16%), with no difference between ages 9 to 11 years (see Fig. 18-1B). There was no increase in hamstring peak torque after the age of 11 in females, despite an increase in quadriceps strength (see earlier). Similar to the peak extension torque, a gender difference in mean flexion peak torques became evident after the age of 14 years. This hamstring strength deficit in females, along with the increased quadriceps strength that occurs with maturation, may contribute to a muscle force imbalance across the knee and ACL strain patterns during activities. Therefore, hamstring strengthening programs, in particular, for young female athletes appear to be an essential component of knee injury prevention programs.
Ramos and associates37 examined the isokinetic strength (60°/sec) of knee extensor muscles in young athletes. Dominant knees in 57 males and females ages 11 to 18 years were tested and strength levels were corrected for body weight. The female athletes aged 11 to 12 years displayed 95% of the strength of age-matched male athletes. At ages 13 to 14, females generated 90% of male strength. By age 17, male athletes were much stronger in extension than females of the same age. Female athletes displayed only 74% of the strength of age-matched male athletes. Similar to the data reported by Barber-Westin and coworkers,4,5 the strength changes in females in the prepubescent years were similar to that of age-matched males, but the increases in female strength slowed and then essentially stopped after puberty while the strength of male athletes continued to increase. Ahmad and colleagues1 reported similar results for H:Q co-activation ratios in 123 immature and mature soccer players (70 male, 53 female). In contrast, several investigators have found no significant gender or age difference in H:Q ratio in young athletes4,5,9 (see Table 18-4).
FUNCTIONAL BIOMECHANICS
Knee
Excessive joint laxity and the decreased ability to generate muscle resistance across the knee are believed to contribute to injury susceptibility. Several authors1,8,15,16,27,40,47 have demonstrated joint knee laxity differences between male and female athletes that may, in part, reflect passive muscle properties.
The ability to increase active muscular resistance to motion (stiffness) across the knee joint has the potential to dissipate damaging loads across knees that can injure ligaments and other passive structures.7,15,16,47,49 Males are capable of producing greater active stiffness across the knee than females.15,16,47,49
Granata and coworkers16 tested active muscle stiffness at the ankle by applying a perturbation at three different weight load conditions (0 kg, 6 kg, and 20% maximum voluntary exertion). These loads created a knee flexion or extension moment. The 23 healthy subjects (12 male, 11 female) were positioned with their knees at 45° prior to perturbation. Males exhibited a mean stiffness of 25 to 164 Nm/rad greater than the mean values of female subjects. Females produced 56% to 73% of male subjects’ muscles stiffness at each load. Male subjects maintained a higher stiffness in the hamstrings and quadriceps at all weight load conditions tested (Table 18-5).
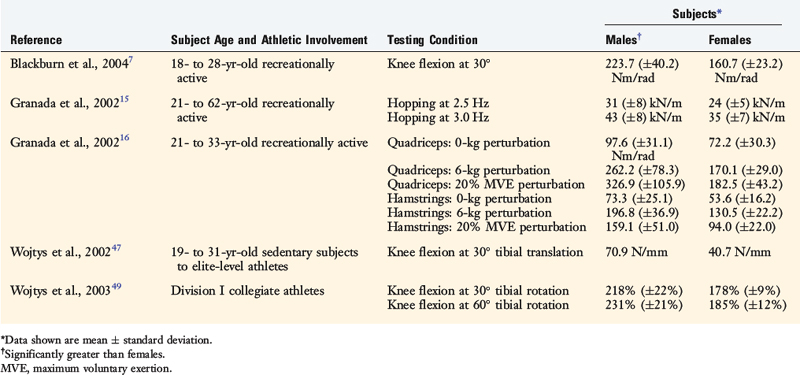
Wojtys and associates47 measured the active and passive sagittal-plane knee stiffness of 23 healthy volunteers (10 male, 13 female) and also concluded that male subjects produced higher levels of knee joint stiffness than female subjects. Most importantly, the dynamic capacity in males was much greater than that measured in females (379% and 212%, respectively; see Table 18-5).
Granata and associates15 studied a two-legged-hopping task at frequencies of 2.5 Hz and 3.0 Hz while testing 30 subjects (15 male, 15 female) whose ages ranged from 21 to 62 years. Males maintained greater knee joint stiffness than females. A subgroup of younger and more physically active subjects (ages 21–31 yr) demonstrated results similar to that of the group at large: males produced greater knee joint stiffness (see Table 18-5). The lower extremity stiffness of athletic female subjects was 77% and 81% of that observed in male athletic and nonathletic subjects, respectively. Blackburn and colleagues7 reported similar results in physically active males and females (see Table 18-5).
Because there is a rotational component to many knee injuries in sports, Wojtys and coworkers49 tested the dynamic rotational stiffness of 24 Division I athletes (12 male, 12 female) who competed in high-risk ACL injury pivoting sports. The data were compared with those of 28 collegiate athletes (14 male, 14 female) participating in low injury–risk nonpivoting sports such as running, bicycling, and crew. Males generated a larger percentage increase in dynamic knee joint resistance to rotation at both 30° and 60° of knee flexion. Male athletes who participated in pivoting sports had a greater percentage increase (275% at 30° knee flexion) in dynamic knee joint resistance than the other three groups (159% females in pivoting sports, 191% control females, and 170% males in nonpivoting sports). Female athletes participating in pivoting sports had the lowest percentage increase in active knee joint resistance to rotation (see Table 18-5). These findings raised concerns about the current training and conditioning of female athletes in these high-risk sports. Because it was unlikely that these sports at the Division I level attracted a group of weaker female athletes, the current training routines may not be effective in producing muscle use patterns that resist undesirable rotational movements at the knee. Differences in muscle tendon unit stiffness can be attributed to muscle, tendon, or both. Most recent studies have focused on muscle. Interestingly, investigations using ultrasound have documented impressive gender differences in the gastrocnemius muscle28 and patellar tendon.34 More importantly, tendon viscoelastic performance has been linked to postural balance and may be the mechanism by which muscle-tendon stiffness plays a role in injury risk.34
Lower Extremity
Biomechanical factors and neuromuscular responses in the lower extremity both above and below the knee may influence knee injury susceptibility. Muscle use patterns while performing dynamic athletic tasks, such as drop-landings, cutting, and, pivoting have been studied with mixed results in terms of gender.22,25,26,36,42
One viewpoint is that muscle strength often predicts activity characteristics and joint positioning in vivo. For example, landing from a jump with the knee joint near full extension may be the result of weak quadriceps muscles. Unfortunately, the increased percentage of ground reaction force transferred through the knee because of a more extended knee position may increase the likelihood of knee injury. Because noncontact jump-landings are one of the most frequent mechanisms of ACL injury in females, Huston and associates26 assessed knee flexion angle in 20 healthy activity level–matched individuals (10 male, 10 female) during drop landings. Even though it is not a very challenging task, when starting from heights of 40 cm and 60 cm, females landed in more knee extension than their age- and size-matched male counterparts (Table 18-6).
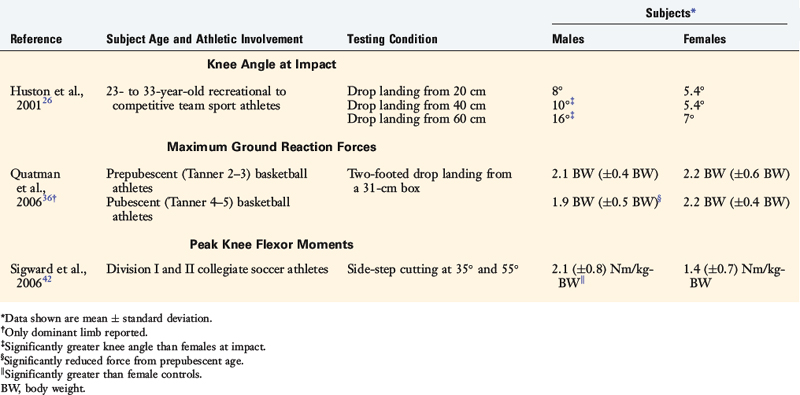
Quatman and colleagues36 examined landing forces of 33 adolescent basketball athletes (17 male, 16 female) during a drop-landing followed by a vertical jump looking for gender and maturation differences. At baseline testing, all athletes were Tanner stage 2 or 3. In the following year, all athletes were Tanner stage 4 or 5. Male athletes were more efficient at reducing ground reaction forces during landing as they matured (9.5% on the dominant side and 18.2% on the nondominant side). Unfortunately, female athletes did not demonstrate this favorable trend, producing higher ground reaction forces and higher loading rates than the mature male athletes (see Table 18-6). This lack of adaptation suggests a generalized phenomenon: males improve their neuromuscular efficiency more than females as they mature. Therefore, targeting these age groups of athletes in the high-risk sports for focused training and conditioning appears to be a worthwhile approach as the athlete approaches puberty.
In a more specific athletic task–related muscle strength test, 30 Division I or II soccer athletes (15 male, 15 female) were tested at a 35° and 55° cutting maneuver after a 5-m run.42 After adjusting for body weight, male athletes produced a greater peak knee flexor moment during early deceleration than their female counterparts who demonstrated a greater average quadriceps activation than male athletes (191% and 151% maximum voluntary isometric contraction, respectively; see Table 18-6).
Core
Core stability can be defined as the capacity of the lumbar-pelvic-hip muscle complex to control lower trunk movement and maintain stability of the vertebral column after skeletal perturbation.45 Therefore, the core musculature may influence the kinematics and load-bearing capacity of the knee by determining what loads are transmitted from the torso.17,19,29 Core stabilization potential and muscle endurance should not be overlooked in investigations of lower extremity injury potential.17,19,29,52 Several clinical tests of core stability (e.g., isometric side-bridge) have been conducted to test these relationships.14,31
Leetun and coworkers29 explored the relationship between core strength and the injury rate of 139 collegiate basketball and cross-country athletes (60 male, 79 female) during a competitive athletic season. During the season, 28 female and 13 male (41 of 139) athletes experienced back or lower extremity injuries. Injured athletes were weaker in hip abduction and hip external rotation strength (Table 18-7). Gender differences were seen in hip abduction, hip external rotation strength, and side-bridge endurance (quadratus lumborum strength). Male athletes displayed greater core stability strength (see Table 18-7) similar to results for side-bridge endurance testing.14,31 It is noteworthy that, of the 139 athletes in Leetun and coworkers’ study,29 only 1 athlete (a female) experienced a season-ending ACL injury. This individual’s core strength was significantly lower than the average female athlete.
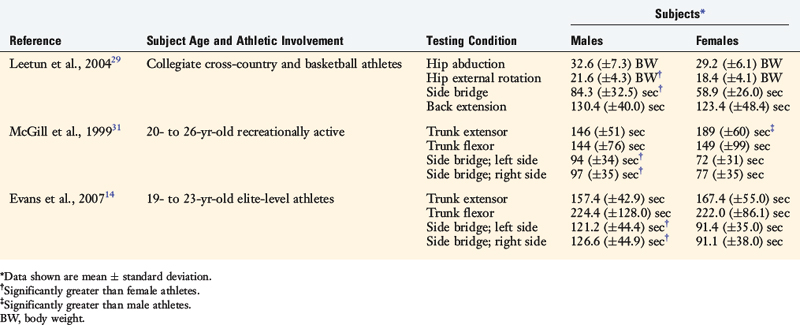
Core muscle fatigue can affect lower extremity muscle performance. McGill and associates31 compared isometric endurance values for low back stabilization in male and female athletes participating in soccer, rowing, and golf. Lateral endurance (side-bridge) was not sports-specific, but it was gender-related. Women produced better endurance times in the trunk extensor exercise than males (189 ± 60 sec and 146 ± 51 sec, respectively).31 However, gender differences in trunk extensor exercises were not observed by Evans and colleagues14 and Leetun and coworkers29 (see Table 18-7).
Essential to core stability, the gluteus medius helps stabilize the hip and in turn supports the lumbopelvic complex. A weakness in the hip musculature can result in suboptimal positioning and loading of the lower extremity during athletic activity.19,32 Gender differences in hip muscle activity were reported in 16 Division I soccer athletes (8 male, 8 female) during a single-legged forward take-off and landing task.17 The gluteus medius muscle activity was almost three times higher in males than in females (electromyography root mean square: 7.16 ± 3.16 and 2.62 ± 0.95, respectively).
In summary, females appear to have decreased levels of core stability and hip muscle strength than their male counterparts. Core strengthening (rectus abdominis, quadratus lumborum, and lumbar extensors) can be achieved with curl-ups, side planks, and birddog exercises45 (Figs. 18-2 to 18-4). Particular attention to femoral abduction and external rotation strength appears to be justified because of their potential role in maintaining favorable lower extremity alignment during high-risk athletic tasks.



TRAINING PROGRAMS
Neuromuscular training may be the most efficient route to knee injury prevention.3,18,23,50 Intrinsic factors including neuromuscular balance and dynamic joint laxity appear to be modifiable with appropriate training.19,23,27
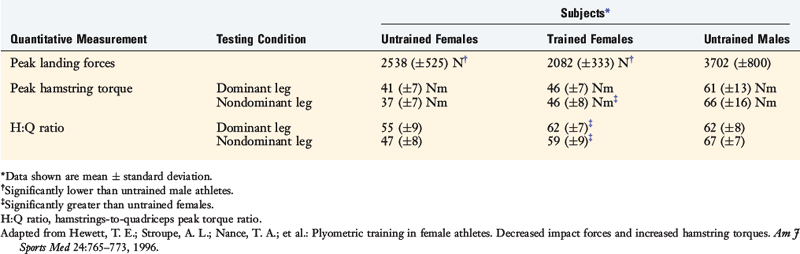
Hewett and coworkers22 developed a jump-training neuromuscular program for female athletes to address perceived deficits in lower extremity strength and poor body positioning during landing (see Chapter 19, Decreasing the Risk of Anterior Cruciate Ligament Injuries in Female Athletes). Eleven female high school volleyball athletes underwent 2-hour training sessions 3 days a week for 6 weeks. Upon completion of training, 10 of the 11 female athletes decreased their peak landing forces by 22%. The peak landing forces before and after training were lower than those of the untrained male athletes (Table 18-8). With training, peak hamstring torque increased 13% in the dominant leg and 26% in the nondominant leg in female athletes (see Table 18-8). Consequently, the H:Q ratio improved to nearly that of the untrained male: 13% in the dominant leg and 26% in the nondominant leg.
Knee muscle resistance to translational movements that generate tibial femoral shear can be examined by determining tibial control characteristics. An analysis of muscle activation patterns in response to an anterior tibial translation in the elite female athletes with excellent quadriceps and hamstring peak torques27 showed that the females favored the initial activation of their hamstrings. Interestingly, the 5 weakest female athletes activated their quadriceps initially in response to the same stimulus. This quadriceps dominance may be a risk factor for ACL injury because the quadriceps is an ACL antagonist. These worrisome findings appear to justify balanced lower extremity muscle conditioning, especially in injured athletes.
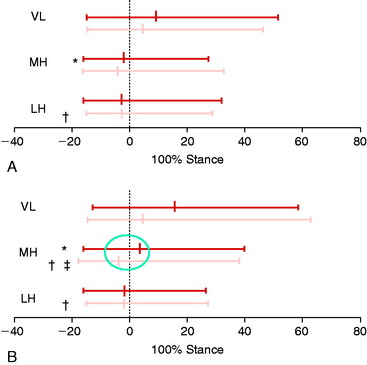
A perturbation-enhanced training program that incorporated strength training and agility drills was able to normalize quadriceps-hamstring balance in female collegiate athletes who presented with the “quadriceps dominant” activation pattern.24 After training, both medial and lateral hamstrings were activated earlier (Fig. 18-5). Most importantly, after 10 1-hour sessions in the perturbation-enhanced training program, female athletes increased their active knee muscle stiffness across the knee (see Fig. 18-5). Theoretically, these results may explain the positive trends seen in some injury prevention programs and they help reduce the risk of injury to the knee.24 Unfortunately, males did not display significant changes with training.
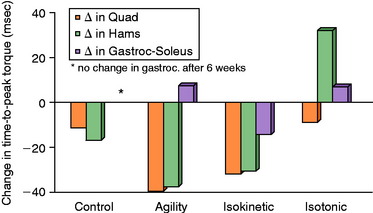
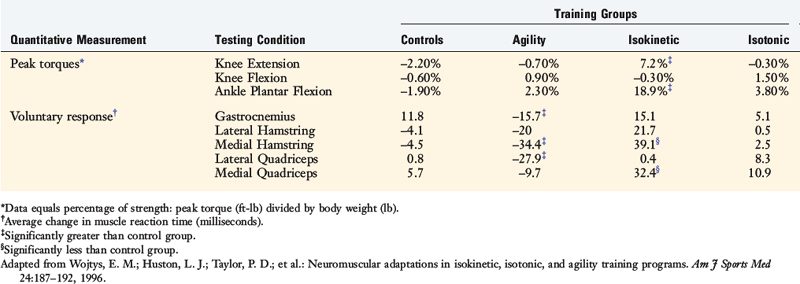
In an effort to determine which type of training might be most beneficial to athletes at risk, Wojtys and associates50 tested the effects of isotonic, isokinetic, and agility exercise regimens on the ability to resist anterior tibial translation, muscle reaction time, and time to peak muscle torque. Thirty-two healthy active volunteers trained for 30 minutes, 3 times a week for 6 weeks. After normalizing strength values with respect to body weight, the isokinetic group was stronger in knee extension and ankle plantar flexion peak torques after training. The isokinetic protocol was the only training regimen that decreased the time to peak torque in the quadriceps, hamstrings, and gastrocnemius muscles (Fig. 18-6). Surprisingly, the muscle reaction times for the isokinetic-training groups were significantly slower in the medial hamstrings (39.1 msec) and medial quadriceps (32.4 msec) muscles (Table 18-9). The isotonic and agility groups predictably showed no increase in isokinetic strength after completing the training regimen (see Table 18-9). The agility-training group generated the greatest decrease (38 msec) in time to peak hamstring torque among the groups. The muscle reaction time of the agility-trained group displayed significant improvements at all levels of function: spinal cord, intermediate, and voluntary response.
1 Ahmad C.S., Clark A.M., Heilmann N., et al. Effect of gender and maturity on quadriceps-to-hamstring strength ratio and anterior cruciate ligament laxity. Am J Sports Med. 2006;34:370-374.
2 Anderson A.F., Dome D.C., Gautam S., et al. Correlation of anthropometric measurements, strength, anterior cruciate ligament size, and intercondylar notch characteristics to sex differences in anterior cruciate ligament tear rates. Am J Sports Med. 2001;29:58-66.
3 Baratta R., Solomonow M., Zhou B.H., et al. Muscular coactivation. The role of the antagonist musculature in maintaining knee stability. Am J Sports Med. 1988;16:113-122.
4 Barber-Westin S.D., Galloway M., Noyes F.R., et al. Assessment of lower limb neuromuscular control in prepubescent athletes. Am J Sports Med. 2005;33:1853-1860.
5 Barber-Westin S.D., Noyes F.R., Galloway M. Jump-land characteristics and muscle strength development in young athletes: a gender comparison of 1140 athletes 9 to 17 years of age. Am J Sports Med. 2006;34:375-384.
6 Barrett D.S. Proprioception and function after anterior cruciate reconstruction. J Bone Joint Surg Br. 1991;73:833-837.
7 Blackburn J.T., Riemann B.L., Padua D.A., et al. Sex comparison of extensibility, passive, and active stiffness of the knee flexors. Clin Biomech (Bristol, Avon). 2004;19:36-43.
8 Bowerman S.J., Smith D.R., Carlson M., King G.A. A comparison of factors influencing ACL injury in male and female athletes and non-athletes. Phys Ther Sport. 2006;7:144-152.
9 Buchanan P.A., Vardaxis V.G. Sex-related and age-related differences in knee strength of basketball players ages 11–17 years. J Athl Train. 2003;38:231-237.
10 Carcia C.R., Shultz S.J., Granata K.P., et al. Females recruit quadriceps faster than males at multiple knee flexion angles following a weight-bearing rotary perturbation. Clin J Sport Med. 2005;15:167-171.
11 Corrigan J.P., Cashman W.F., Brady M.P. Proprioception in the cruciate deficient knee. J Bone Joint Surg Br. 1992;74:247-250.
12 Cowling E.J., Steele J.R. Is lower limb muscle synchrony during landing affected by gender? Implications for variations in ACL injury rates. J Electromyogr Kinesiol. 2001;11:263-268.
13 Dugan S.A. Sports-related knee injuries in female athletes: what gives? Am J Phys Med Rehabil. 2005;84:122-130.
14 Evans K., Refshauge K.M., Adams R. Trunk muscle endurance tests: reliability and gender differences in athletes. J Sci Med Sport. 2007;10:447-455.
15 Granata K.P., Padua D.A., Wilson S.E. Gender differences in active musculoskeletal stiffness. Part II. Quantification of leg stiffness during functional hopping tasks. J Electromyogr Kinesiol. 2002;12:127-135.
16 Granata K.P., Wilson S.E., Padua D.A. Gender differences in active musculoskeletal stiffness. Part I. Quantification in controlled measurements of knee joint dynamics. J Electromyogr Kinesiol. 2002;12:119-126.
17 Hart J.M., Garrison J.C., Kerrigan D.C., et al. Gender differences in gluteus medius muscle activity exist in soccer players performing a forward jump. Res Sports Med. 2007;15:147-155.
18 Hewett T.E., Lindenfeld T.N., Riccobene J.V., et al. The effect of neuromuscular training on the incidence of knee injury in female athletes. A prospective study. Am J Sports Med. 1999;27:699-706.
19 Hewett T.E., Myer G.D., Ford K.R. Anterior cruciate ligament injuries in female athletes: part 1, mechanisms and risk factors. Am J Sports Med. 2006;34:299-311.
20 Hewett T.E., Paterno M.V., Myer G.D. Strategies for enhancing proprioception and neuromuscular control of the knee. Clin Orthop Relat Res. 2002;402:76-94.
21 Hewett T.E., Paterno M.V., Noyes F.R. Differences in single leg balance on an unstable platform between female and male normal, ACL-deficient and ACL-reconstructed knees. Paper presented at the 25th Annual Meeting of the American Orthopaedic Society for Sports Medicine, June 19–22, Traverse City, MI. 1999.
22 Hewett T.E., Stroupe A.L., Nance T.A., et al. Plyometric training in female athletes. Decreased impact forces and increased hamstring torques. Am J Sports Med. 1996;24:765-773.
23 Hewett T.E., Zazulak B.T., Myer G.D., et al. A review of electromyographic activation levels, timing differences, and increased anterior cruciate ligament injury incidence in female athletes. Br J Sports Med. 2005;39:347-350.
24 Hurd W.J., Chmielewski T.L., Snyder-Mackler L. Perturbation-enhanced neuromuscular training alters muscle activity in female athletes. Knee Surg Sports Traumatol Arthrosc. 2006;14:60-69.
25 Huston L.J., Greenfield M.L., Wojtys E.M. Anterior cruciate ligament injuries in the female athlete. Potential risk factors. Clin Orthop Relat Res. 2000;372:50-63.
26 Huston L.J., Vibert B., Ashton-Miller J.A., et al. Gender differences in knee angle when landing from a drop-jump. Am J Knee Surg. 2001;14:215-219. discussion 219–220
27 Huston L.J., Wojtys E.M. Neuromuscular performance characteristics in elite female athletes. Am J Sports Med. 1996;24:427-436.
28 Kubo K., Kanehisa H., Azuma K., et al. Muscle architectural characteristics in young and elderly men and women. Int J Sports Med. 2003;24:125-130.
29 Leetun D.T., Ireland M.L., Willson J.D., et al. Core stability measures as risk factors for lower extremity injury in athletes. Med Sci Sports Exerc. 2004;36:926-934.
30 Lephart S.M., Ferris C.M., Riemann B.L., et al. Gender differences in strength and lower extremity kinematics during landing. Clin Orthop Relat Res. 2002;401:162-169.
31 McGill S.M., Childs A., Liebenson C. Endurance times for low back stabilization exercises: clinical targets for testing and training from a normal database. Arch Phys Med Rehabil. 1999;80:941-944.
32 Nadler S.F., Malanga G.A., DePrince M., et al. The relationship between lower extremity injury, low back pain, and hip muscle strength in male and female collegiate athletes. Clin J Sport Med. 2000;10:89-97.
33 Noyes F.R., Barber-Westin S.D. Isokinetic profile and differences in tibial rotation strength between male and female athletes 11 to 17 years of age. Isok Exer Sci. 2005;13:251-259.
34 Onambele G.N., Burgess K., Pearson S.J. Gender-specific in vivo measurement of the structural and mechanical properties of the human patellar tendon. J Orthop Res. 2007;25:1635-1642.
35 Pincivero D.M., Gandaio C.M., Ito Y. Gender-specific knee extensor torque, flexor torque, and muscle fatigue responses during maximal effort contractions. Eur J Appl Physiol. 2003;89:134-141.
36 Quatman C.E., Ford K.R., Myer G.D., et al. Maturation leads to gender differences in landing force and vertical jump performance: a longitudinal study. Am J Sports Med. 2006;34:806-813.
37 Ramos E., Frontera W.R., Llopart A., et al. Muscle strength and hormonal levels in adolescents: gender-related differences. Int J Sports Med. 1998;19:526-531.
38 Rosene J.M., Fogarty T.D., Mahaffey B.L. Isokinetic hamstrings:quadriceps ratios in intercollegiate athletes. J Athl Train. 2001;36:378-383.
39 Rozzi S.L., Lephart S.M., Fu F.H. Effects of muscular fatigue on knee joint laxity and neuromuscular characteristics of male and female athletes. J Athl Train. 1999;34:106-114.
40 Rozzi S.L., Lephart S.M., Gear W.S., et al. Knee joint laxity and neuromuscular characteristics of male and female soccer and basketball players. Am J Sports Med. 1999;27:312-319.
41 Shultz S.J., Perrin D.H., Adams M.J., et al. Neuromuscular response characteristics in men and women after knee perturbation in a single-leg, weight-bearing stance. J Athl Train. 2001;36:37-43.
42 Sigward S.M., Powers C.M. The influence of gender on knee kinematics, kinetics and muscle activation patterns during side-step cutting. Clin Biomech (Bristol, Avon). 2006;21:41-48.
43 Uhorchak J.M., Scoville C.R., Williams G.N., et al. Risk factors associated with noncontact injury of the anterior cruciate ligament: a prospective four-year evaluation of 859 West Point cadets. Am J Sports Med. 2003;31:831-842.
44 White K.K., Lee S.S., Cutuk A., et al. EMG power spectra of intercollegiate athletes and anterior cruciate ligament injury risk in females. Med Sci Sports Exerc. 2003;35:371-376.
45 Willson J.D., Dougherty C.P., Ireland M.L., et al. Core stability and its relationship to lower extremity function and injury. J Am Acad Orthop Surg. 2005;13:316-325.
46 Withrow T.J., Huston L.J., Wojtys E.M., et al. The relationship between quadriceps muscle force, knee flexion, and anterior cruciate ligament strain in an in vitro simulated jump landing. Am J Sports Med. 2006;34:269-274.
47 Wojtys E.M., Ashton-Miller J.A., Huston L.J. A gender-related difference in the contribution of the knee musculature to sagittal-plane shear stiffness in subjects with similar knee laxity. J Bone Joint Surg Am. 2002;84:10-16.
48 Wojtys E.M., Huston L.J. Neuromuscular performance in normal and anterior cruciate ligament–deficient lower extremities. Am J Sports Med. 1994;22:89-104.
49 Wojtys E.M., Huston L.J., Schock H.J., et al. Gender differences in muscular protection of the knee in torsion in size-matched athletes. J Bone Joint Surg Am. 2003;85:782-789.
50 Wojtys E.M., Huston L.J., Taylor P.D., et al. Neuromuscular adaptations in isokinetic, isotonic, and agility training programs. Am J Sports Med. 1996;24:187-192.
51 Wojtys E.M., Wylie B.B., Huston L.J. The effects of muscle fatigue on neuromuscular function and anterior tibial translation in healthy knees. Am J Sports Med. 1996;24:615-621.
52 Zazulak B.T., Hewett T.E., Reeves N.P., et al. Deficits in neuromuscular control of the trunk predict knee injury risk: a prospective biomechanical-epidemiologic study. Am J Sports Med. 2007;35:1123-1130.
53 Zazulak B.T., Hewett T.E., Reeves N.P., et al. The effects of core proprioception on knee injury: a prospective biomechanical-epidemiological study. Am J Sports Med. 2007;35:368-373.
[/level-membership-for-orthopaedics-category][not-level-membership-for-orthopaedics-category]
Chapter 18 Gender Differences in Muscular Protection of the Knee
PROPRIOCEPTION
Proprioception refers to an individual’s awareness of joint and body movement and their position in space. Motor control feedback via the gamma motor system can modify muscle stiffness or transjoint resistance of muscles to control joint movement and positioning during planned and unexpected events. Therefore, skeletal muscle plays an important role in knee joint proprioception. An individual’s ability to detect knee joint position and motion is a major component required for reflex response, allowing joint stabilization and protection to develop. When errors in these systems occur, or when these systems function at suboptimal levels, increased ligament strain, articular cartilage shear, and/or bone impact may result. High risk positioning of the lower extremity may also occur.13,20
Several authors have reported gender differences in proprioception.21,39,40,53 Rozzi and coworkers40 investigated joint proprioception in 34 (17 male, 17 female) collegiate soccer and basketball athletes by measuring the threshold to detection of passive motion using a device that moved the knee joint at a constant 0.5°/sec velocity through flexion and extension. A rotational transducer provided angular displacement values. Compared with male athletes, females took significantly longer to detect the threshold of knee joint motion in extension (2.11° ± 0.63° and 2.95° ± 1.47°, respectively; P = .039). However, no significant gender difference was observed during flexion. The clinical significance of a mean difference of 0.84° of angular motion between genders is unknown.
Hewett and associates21 assessed proprioception using single-leg postural balance at the knee on a dynamic platform in ACL-deficient subjects. Uninjured females demonstrated greater knee joint stability than males, which the authors attributed to a lower center of gravity. In contrast, males had significantly greater single-leg stability after an ACL rupture, and females took longer to regain adequate levels of single-leg balance postoperatively.21 A clear gender difference cannot be extracted from these results.
Although injury research often focuses on the lower limbs, the core of the torso may be the key to understanding body positioning. Therefore, the core muscle of the torso should not be overlooked in the investigation of proprioception. Zazulak and colleagues53 evaluated core proprioception and knee joint control. Two-hundred seventy-seven collegiate athletes (137 male, 140 female) underwent core proprioceptive measurements by passive trunk rotation in the seated position through 20° in the transverse plane. With auditory and visual stimuli diminished, the athletes were instructed to reproduce the initial position after displacement. The difference between the perceived and the actual angle was calculated as the active proprioceptive repositioning error. After testing, the athletes were followed for 3 years, during which 25 (14 male, 11 female) sustained knee injuries. Analysis of the active proprioceptive repositioning error revealed that females who sustained knee ligament or meniscal injuries demonstrated significantly greater error in active repositioning than uninjured females. Male athletes did not demonstrate this problem. In addition, uninjured female athletes had significantly better core proprioception than uninjured male athletes, which supports previous studies.20,40 Zazulak and coworkers52 also reported that after an unexpected perturbation, the maximal trunk displacement in females who suffered knee ligament injuries was significantly greater than that of females who did not experience injury. No significant difference in maximal trunk displacement between injured and uninjured males was found. Therefore, the core stability of female athletes may be a greater factor in lower extremity injury susceptibility than that in males.52 In fact, lateral trunk displacement was the lone significant predictor of ligament injury in female athletes (P = .001) in this investigation, with 100% sensitivity and 72% specificity rates reported. This was not true for male athletes, because their sole predictor of injury was a history of low back pain.52
Other factors that may influence proprioceptive function include joint laxity and muscle fatigue, both of which also affect muscle function. Rozzi and associates39 reported that female athletes had greater knee laxity that resulted in a decreased sensitivity to knee position change. Many clinicians have suspected that joint laxity is a risk factor for knee injury, but the evidence is not overwhelming. The best evidence may be that provided by Uhorchak and colleagues43 in their risk factor analysis for ACL injury in military cadets.
Regarding muscle fatigue, Rozzi and associates39 showed in male and female collegiate basketball and soccer athletes that induced fatigue altered proprioception, especially in knee extension. Wojtys and coworkers51 evaluated the effects of muscle fatigue on anterior tibial translation, muscle reaction time, and recruitment order in 10 athletes (6 male, 4 female) whose physical activity included jumping, pivoting, and twisting. Each athlete completed baseline measurements and then underwent a vigorous isokinetic workout until quadriceps and hamstrings torques decreased by 50% or greater. Eight of the 10 fatigued athletes demonstrated greater anterior tibial translation during dynamic testing (average percentage increase, 32.5%), indicating that fatigue did increase joint laxity. Fatigued athletes did not alter their muscle recruitment order in response to an anterior tibial translation. However, after fatigue, muscle reaction time slowed significantly in the three response phases (spinal reflex, intermediate, and voluntary). Although the investigation found a change in muscle reaction time and laxity of the knee, no gender difference was reported for these factors, nor was a correlation established between fatigue and a decrease in proprioception.
Earlier studies have evaluated the effect of ACL-deficiency on proprioception, although gender was not specifically examined.6,11,48 More recent studies have focused on gender differences. In general, these studies show that injured female athletes have poorer lower extremity proprioception than their male athlete counterparts.21,40,52 However, uninjured female athletes tend to have higher levels of stability than healthy male athletes.
Considering the consequences of serious knee injury, proprioceptive prescreening of female athletes, especially in high-risk sports, prior to athletic participation may help focus training and conditioning programs.20,52,53
MUSCLE RESPONSE
Time to Peak Torque
Neuromuscular activation patterns influence dynamic knee joint stability potential, which may contribute to knee injury susceptibility.10,19,23,25 Gender-related differences in these activation patterns have been reported by numerous investigators.8,10,27,33,40,41,44,47
Using isokinetic peak torque strength testing of 100 Division I athletes (60 male, 40 female), Huston and Wojtys27 detected significant gender differences. Female athletes and controls generated similar time to peak knee flexion torques, which were slower than male athletes. Male athletes were able to generate peak knee extension and flexion torques faster than male or female controls (Table 18-1). The slowed response of the hamstring in females was most striking.
Considering the young age at which many ACL injuries occur, muscle function maturation should be considered in the evaluation of injury susceptibility. Noyes and Barber-Westin33 examined the gender- and age-related differences in time to peak torque for internal and external tibial rotation with isokinetic strength testing. They separated 94 athletes into two age groups: 11 to 13 years of age (20 male, 20 female) and 14 to 17 years of age (27 male, 27 female). Older male athletes were faster (28%) in internal rotation peak torque of the hamstrings than age-matched female athletes (see Table 18-1). In contrast, multiple investigators have reported no gender differences in isokinetic peak torques for quadriceps and/or hamstrings in collegiate athletes,8,40 nonathlete controls,8 and athletes 13 years of age or younger4,33 (see Table 18-1).
Muscle Reaction Time
In an attempt to identify more relevant functional gender differences, several investigators have assessed peak muscle torque during weight-bearing perturbations and athletic tasks. Shultz and associates41 examined muscle response times in 64 collegiate lacrosse and soccer athletes (32 male, 32 female) after applying an unexpected rotational perturbation force to the lower extremity. Female athletes’ muscle response times for the quadriceps muscles were faster than male athletes with comparable recruitment patterns (Table 18-2). The Division I collegiate athletes displayed faster muscle response times than the recreational athletes.
Carcia and colleagues10 measured the response times of the quadriceps, hamstrings, and gastrocnemius muscles after a weight-bearing rotary perturbation in 20 recreationally active adults (10 male, 10 female). Males and females responded with similar muscle recruitment order patterns at various angles of flexion (10°, 20°, 30°), and females generated faster quadriceps muscle response times than males at all angles (see Table 18-2).
Using a posterior force to the calf muscle to simulate anterior tibial translation, Huston and Wojtys27 reported that female athletes activated their quadriceps first and faster than their male counterparts, raising concerns about what role the quadriceps could directly play in ACL injuries. In contrast, Cowling and Steele12 reported a delay in the semimembranosus (hamstring) muscle of male athletes during abrupt single-leg landing compared with athletic level–matched female athletes.
In summary, preferential quadriceps activation and a slowed hamstring response may lead to a neuromuscular imbalance producing ineffective knee stabilization.10,27,41,49 Powerful or unopposed quadriceps contractions, especially close to knee extension, have the potential to cause ACL injury.46 Further research is necessary to better understand these relationships, especially in terms of muscle activity mode injury rates.
Strength
The timely ability to generate high levels of muscle force across the knee joint may decrease functional joint laxity and result in less stress and strain on the passive structures that constrain knee motion.7,8,15,16,27,47,49 A poor muscle strength–to–body weight ratio may be a risk factor for lower extremity injury.30,43
Besides the peak torque–to–body weight ratio, the balance of forces expressed as the hamstring-to-quadriceps (H:Q) ratio is an additional performance measurement that may provide insight into the gender differences in injury susceptibility. Evidence suggests that the hamstring muscles have the potential to unload the ACL,46 whereas the quadriceps appear to function as the ACL antagonist.46 The suspected relationship between the H:Q peak torque ratio and ACL injury susceptibility has been investigated by several authors.2,8,9,22,38 This factor may be critical in ACL protection.2,4,5,8,9,22,38,49
Bowerman and coworkers8 tested the peak isokinetic muscle torque (60°/sec) of 54 healthy collegiate athletes and 53 age-matched nonathletes. Males were stronger than females for both quadriceps and hamstring muscles (Table 18-3). Unfortunately, measurements were not normalized to body weight in this study. Not surprisingly, athletes generated higher quadriceps and hamstring peak torques. Similar findings were reported by Wojtys and associates47 in 23 healthy volunteers (10 male, 13 female) whose activity level ranged from sedentary to elite-level athletes. Lephart and colleagues30 also reported similar results, as did Bowerman and coworkers8 in 15 Division I collegiate athletes and 15 age-matched male controls under the same testing conditions after normalizing for body weight (see Table 18-3). Male recreational athletes generated greater quadriceps and hamstring peak isokinetic torques (180°/sec) than their female counterparts with body weight normalization.35 In addition, Hewett and coworkers22 and Anderson and associates2 reported that female high school athletes had lower H:Q ratios than male athletes. Conversely, Bowerman and coworkers8 and Rosene and colleagues38
[/not-level-membership-for-orthopaedics-category]
