Dilated stomach with decreased or absent peristalsis
TOP DIFFERENTIAL DIAGNOSES
• Gastric outlet obstruction
• Postoperative state, stomach
• Intestinal scleroderma
• Cystic fibrosis, abdominal signs
• Gastric bezoar
PATHOLOGY
• Idiopathic: No identifiable cause in ∼ 50% of cases
• Type 1 diabetes is main identifiable cause
Usually longstanding and poorly controlled
Affects 40% of patients with diabetes
• Narcotic analgesics are 3rd most common cause
Others drugs may also be implicated
• Postsurgical
Prior thoracic or gastric surgery may injure vagus nerve
Some cases are deliberate
– e.g., to reduce gastric acid production
Other cases are unintentional
– e.g., following fundoplication
• Neurologic disorders
• Electrolyte disturbances
CLINICAL ISSUES
• Symptoms
Nausea, vomiting, postprandial bloating, early satiety are all common
• Treatment
Promotility and antiemetic agents
Botulinum toxin injection into gastric pylorus
Gastric electrical stimulation device
(Left) Upper GI series of a 34-year-old man with type 1 diabetes and persistent nausea shows stasis of the barium (after a 20 minute delay) and food debris within the stomach, in spite of no oral intake for > 12 hours. No peristalsis was evident.
(Right) NECT in a 61-year-old man with diabetes shows a markedly distended stomach containing contrast material and food in spite of the patient having fasted for 12 hours. This indicates delayed gastric emptying and proved to be due to diabetic gastroparesis.
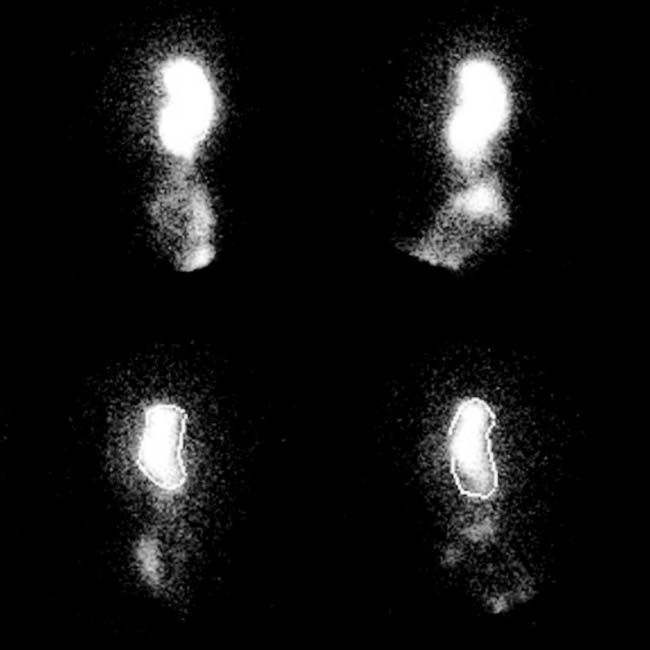
(Left) Gastric emptying scintigraphy in a patient with diabetic gastroparesis shows mild to moderate gastric emptying delay (30% emptied at 120 minutes, 55% at 240 minutes) on this solid-labeled phase. Similar delay was found for liquids.
(Right) Gastric emptying scan shows severe delay in emptying of ingested solids (32% at 120 minutes). This patient had multiple prior surgeries, including vagotomy and Billroth II partial gastrectomy. Multiple factors most likely contribute to delayed emptying in this patient.












 in spite of the patient having fasted for 12 hours. This indicates delayed gastric emptying and proved to be due to diabetic gastroparesis.
in spite of the patient having fasted for 12 hours. This indicates delayed gastric emptying and proved to be due to diabetic gastroparesis.