Chapter 46 Gastrointestinal Bleeding in the Critically ill Patient
2 What are hematemesis, coffee-ground emesis, hematochezia, and melena? Are these features helpful in determining the site and rate of bleeding?




4 What are the most common causes of upper and lower GI bleeding?
See Tables 46-1 and 46-2.
| Cause | Prevalence (%) |
|---|---|
| Peptic ulcer disease | 55 |
| Gastritis-duodenitis | 20 |
| Esophageal varices | 12 |
| Mallory-Weiss tears | 8 |
| Neoplasm | 3 |
| Angiodysplasia | 2 |
Table 46-2 Causes of Lower Gastrointestinal Bleeding
| Cause | Prevalence (%) |
|---|---|
| Diverticular disease | 40 |
| Angiodysplasia | 20 |
| Colitis | 20 |
| Anorectal bleeding (hemorrhoids, anal fissures) | 7 |
| Neoplasm | 7 |
| Small bowel bleeding | 6 |
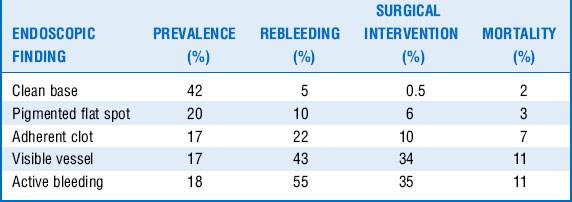
5 What risk factors are associated with higher mortality in patients with upper GI tract hemorrhage?










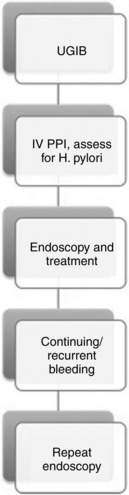
7 What are the immediate actions that need to be taken in an acute GI tract hemorrhage in the ICU?
 Ensure patient has at least two large-bore (at least 18 gauge) intravenous catheters.
Ensure patient has at least two large-bore (at least 18 gauge) intravenous catheters.



 If UGIB, initiate medical therapy with intravenous proton pump inhibitors.
If UGIB, initiate medical therapy with intravenous proton pump inhibitors.
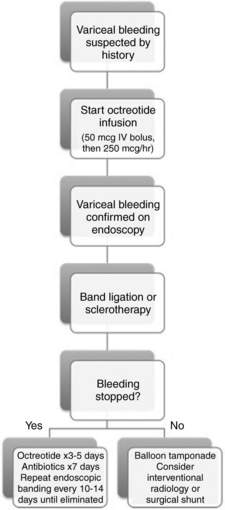
 If suspicious of bleeding varices, start an octreotide infusion.
If suspicious of bleeding varices, start an octreotide infusion.
 Consult the endoscopy and/or radiology and surgical services as needed.
Consult the endoscopy and/or radiology and surgical services as needed.
 For more details on managing acute GI tract bleeding, see algorithms in Figures 46-1 to 46-3.
For more details on managing acute GI tract bleeding, see algorithms in Figures 46-1 to 46-3.
9 What medical therapies are available for the management of GI bleeding?
 Somatostatin analogs: Octreotide is a long-acting somatostatin analog that inhibits glucagon-induced mesenteric vasodilation and has been shown to decrease the risk for persistent bleeding and rebleeding in patients with both variceal and nonvariceal upper tract bleeding. Although somatostatin analogs do not improve mortality rates, they are helpful in reducing bleeding and minimizing transfusion requirements. The recommended dose for octreotide is 250 mcg IV bolus followed by a 250 mcg/hr infusion.
Somatostatin analogs: Octreotide is a long-acting somatostatin analog that inhibits glucagon-induced mesenteric vasodilation and has been shown to decrease the risk for persistent bleeding and rebleeding in patients with both variceal and nonvariceal upper tract bleeding. Although somatostatin analogs do not improve mortality rates, they are helpful in reducing bleeding and minimizing transfusion requirements. The recommended dose for octreotide is 250 mcg IV bolus followed by a 250 mcg/hr infusion.








23 What is the treatment of IC?
Key Points Gi Bleeding
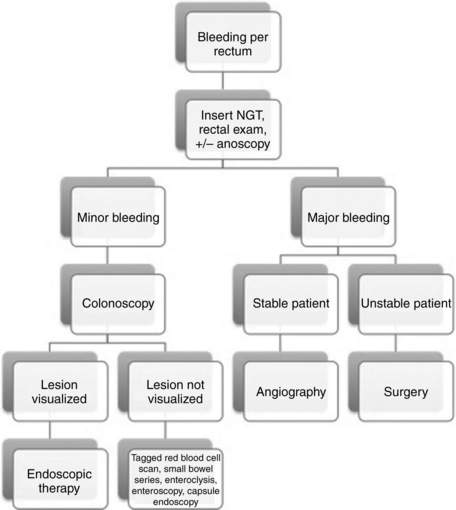
1. Always insert a nasogastric tube to rule out UGIB, even in cases that present with copious fresh blood from the rectum.
2. Early endoscopy is key in both upper and lower GI tract bleeding for diagnosing, risk-stratifying, localizing, and treating bleeding.
3. Do not forget about stress ulcer prophylaxis in critically ill patients with the appropriate indications. Remember to discontinue it when the indications cease to exist.
4. A systematic approach is key in managing all patients with GI bleeding.
1 Barnert J., Messmann H. Diagnosis and management of lower gastrointestinal bleeding. Nat Rev Gastroenterol Hepatol. 2009;6:637–646.
2 Cappell M., Friedel D. Initial management of acute upper gastrointestinal bleeding: from initial evaluation up to gastrointestinal endoscopy. Med Clin North Am. 2008;92:491–509.
3 Ferguson C.B., Mitchell R.M. Nonvariceal upper gastrointestinal bleeding: standard and new treatment. Gastroenterol Clin North Am. 2005;34:607–621.
4 Green B.T., Rockey D.C. Lower gastrointestinal bleeding-management. Gastroenterol Clin North Am. 2005;34:665–678.
5 Laine L., Peterson W.L. Bleeding peptic ulcer. N Engl J Med. 1994;331:717–727.
6 Reissfelder C., Sweiti H., Antolovic D., et al. Ischemic colitis: Who will survive? Surgery. 2011;149:585–592.
7 Rockey D.C. Gastrointestinal bleeding. Gastroenterol Clin North Am. 2005;34:581–588.
8 Spirt M.J. Stress-related mucosal disease: risk factors and prophylactic therapy. Clin Ther. 2004;26:197–213.
9 Yüksel I., Ataseven H., Köklü S., et al. Intermittent versus continuous pantoprazole infusion in peptic ulcer bleeding: a prospective randomized study. Digestion. 2008;78:39–43.
10 Zaman A., Chalasani N. Bleeding caused by portal hypertension. Gastroenterol Clin North Am. 2005;34:623–642.
