







 , lymph nodes
, lymph nodes  , and omentum
, and omentum  .
.
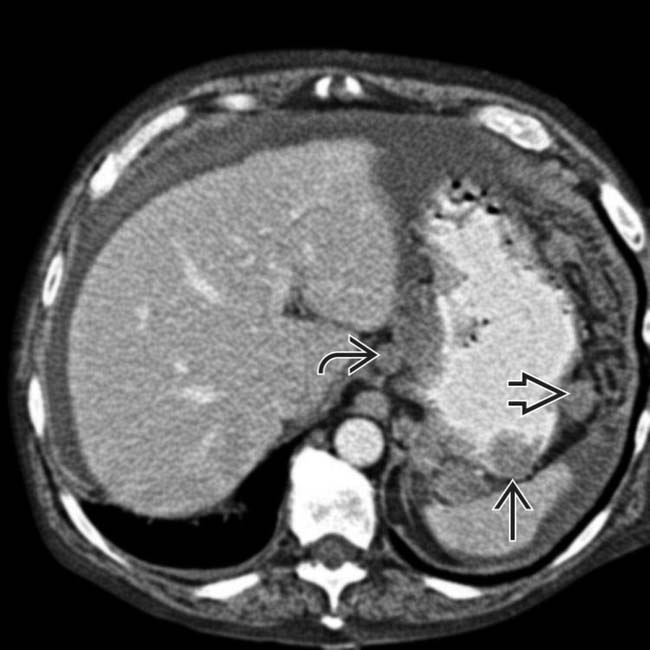
 , lymph nodes
, lymph nodes  , and omentum
, and omentum  , with both nodular and diffuse metastases seen. In addition, the left ureter was obstructed due to a ureteral/retroperitoneal metastasis.
, with both nodular and diffuse metastases seen. In addition, the left ureter was obstructed due to a ureteral/retroperitoneal metastasis.

 . These findings are typical of primary gastric lymphoma.
. These findings are typical of primary gastric lymphoma.IMAGING
General Features

Fluoroscopic Findings
• Fluoroscopic-guided barium study
 Breast carcinoma metastases
Breast carcinoma metastases
 Breast carcinoma metastases
Breast carcinoma metastases







CT Findings
• Multiplanar reformation (MPRs) very useful to judge full extent of disease and relation to adjacent organs, nodes







































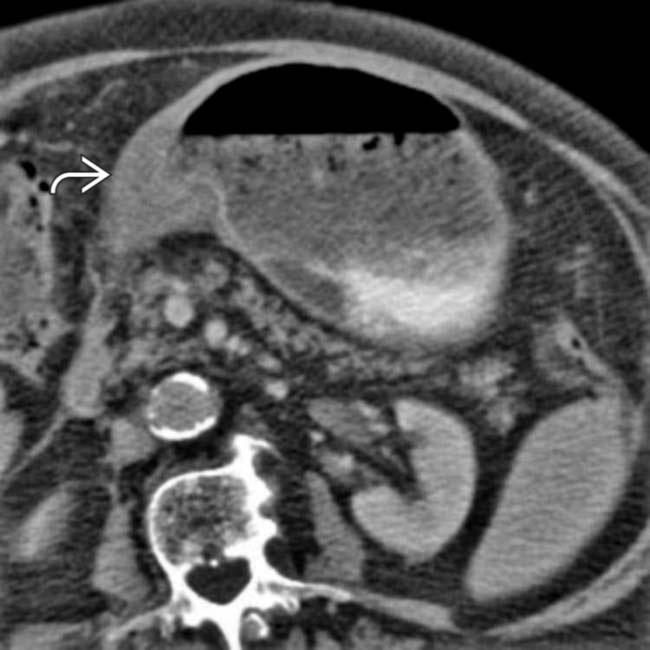
 . The stomach is not well distended or easily assessed.
. The stomach is not well distended or easily assessed.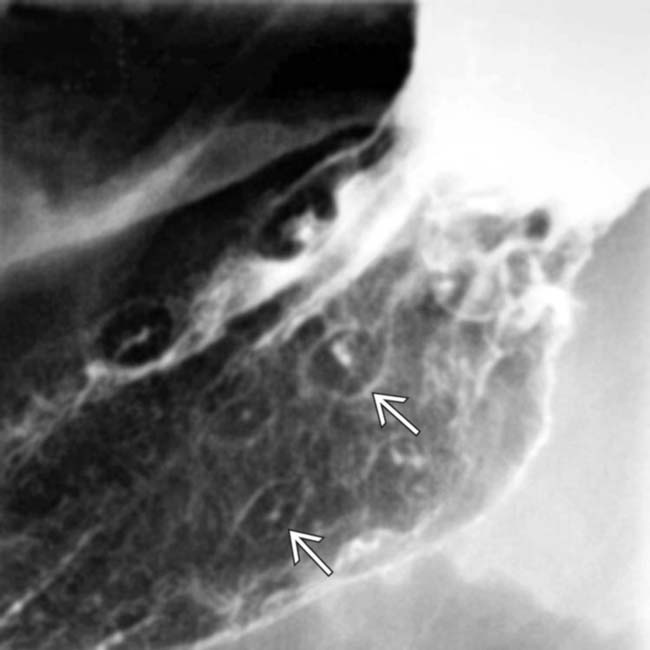
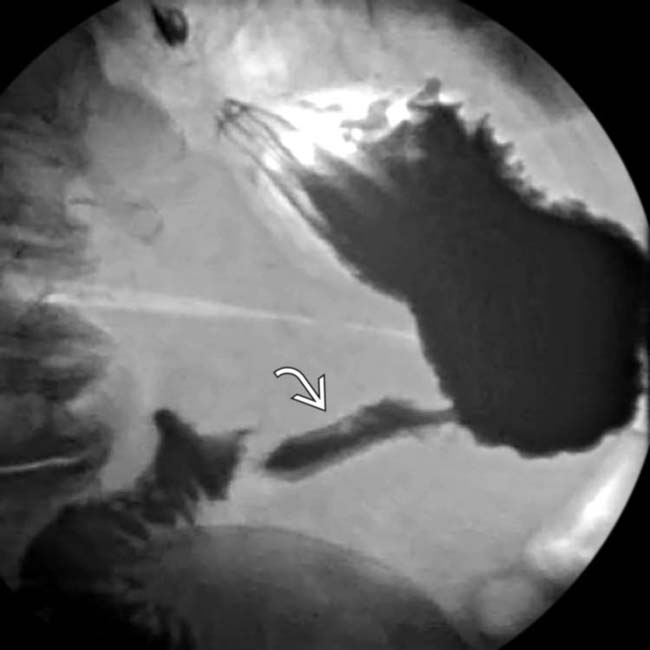
 , consisting of small, intramural masses with a central ulceration.
, consisting of small, intramural masses with a central ulceration.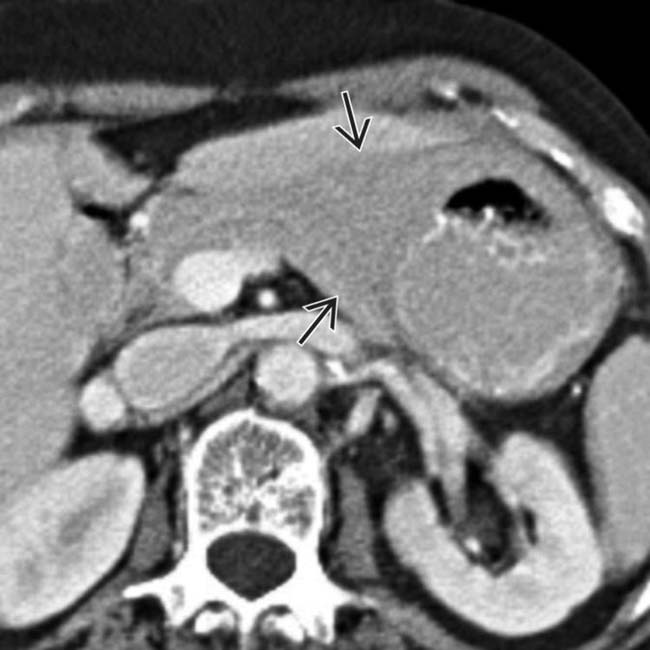
 that diffusely infiltrates the gastric wall. There is no outlet obstruction.
that diffusely infiltrates the gastric wall. There is no outlet obstruction.
 .
.
 causing delayed gastric emptying. These imaging findings are indistinguishable from primary gastric carcinoma.
causing delayed gastric emptying. These imaging findings are indistinguishable from primary gastric carcinoma.

 but no obstruction in this patient with lymphoma.
but no obstruction in this patient with lymphoma.
 but no obstruction.
but no obstruction.

 from metastatic melanoma.
from metastatic melanoma.
 , a discrete intramural polyp with central ulceration in this patient with metastatic melanoma.
, a discrete intramural polyp with central ulceration in this patient with metastatic melanoma.
 in this patient with gastric lymphoma.
in this patient with gastric lymphoma.
 in this patient with gastric lymphoma.
in this patient with gastric lymphoma.


