CHAPTER 25 Fractures of the Olecranon
INTRODUCTION
The subcutaneous location of the olecranon makes it vulnerable to trauma.7 Isolated fractures of the olecranon comprise approximately 10% of fractures about the elbow,26,38 with an estimated incidence of 1.08 per 10,000 person-years.26 Most result from low energy trauma such as a fall from a height of less than 2 meters, a direct blow to the elbow, or from forced hyperextension.1,17,20,26,27,38 A fall on a partially flexed elbow may generate an avulsion fracture of the olecranon from the pull of the triceps.7 Amis et al investigated variable impact mechanisms and the resultant fracture patterns in a cadaveric model.1 A trend was noted in which radial head and coronoid fractures tended to occur with forearm impacts with the elbow in up to 80 degrees of flexion.1 Olecranon fractures occurred with direct blows at 90 degrees of flexion, whereas injuries occurring with the elbow in greater than 110 degrees of flexion tended to result in distal humerus fractures.1
In general, fractures of the olecranon have a favorable prognosis following treatment,7,10,17,20,25,26 with estimates that ninety-six percent of patients have a good to excellent long-term outcome with only rare adverse events.25,26
ANATOMIC CONSIDERATIONS
The olecranon, together with the coronoid process, forms the semilunar or greater sigmoid notch of the ulna.7 This articulates with the trochlea of the humerus and confers stability and facilitates motion in the anterior-posterior plane.7 A transverse “bare area” devoid of cartilage is found at the midpoint between the coronoid and the tip of the olecranon. The unwary surgeon may inadvertently discard structurally significant portions of the olecranon if this is not considered when reconstructing the fractured olecranon.7 The ossification center of the olecranon generally appears by 9 to 10 years of age, and fuses to the proximal ulna by age 14 years.7,14 Persistence of the physis in adulthood may occur, and is usually bilateral and familial. In addition, patella cubiti, an accessory ossicle embedded in the distal triceps, may be present and likewise should not be confused with a fracture.7
EVALUATION
Because the fracture by nature is intra-articular with the exception of some avulsion-type fractures of the olecranon, hemarthrosis is frequently present in conjunction with olecranon fracture.7 Although this sign may be obfuscated by pain due to the injury, inability to actively extend the elbow against gravity may be an important indication of triceps discontinuity.7 Because of the proximity of the ulnar nerve, the first and each subsequent examination should document the status of the ulnar nerve.7 Anteroposterior and true lateral radiographs should be obtained to aid in diagnosis and treatment considerations.7 The true lateral film should be examined to determine the extent and nature of the fracture pattern and to evaluate for the presence of other lesions such as a radial head fracture or dislocation, or distal humerus or coronoid fractures.7
CLASSIFICATION OF OLECRANON FRACTURES
Colton9 classified olecranon fractures according to the degree of displacement and fracture pattern. Colton type I fractures are nondisplaced fractures, in which displacement remains less than 2 mm with elbow flexion to 90 degrees or extension against gravity. The patient can actively extend the elbow against gravity.7,9 Type II, displaced fractures, may be further subtyped into avulsion fractures, oblique and transverse fractures, comminuted fractures, and fracture-dislocations.9
Horne et al20 proposed a classification system and treatment algorithm for olecranon fractures based on review of 100 cases. In this system, type I fractures are either transverse intra-articular fractures of the proximal third of the olecranon or extra-articular fractures involving the point of the olecranon.20 Type II fractures are oblique or transverse intra-articular fractures involving the middle third of the olecranon fossa with type IIA representing those with a single fracture line and type IIB representing those with a second more distal and posteriorly oriented fracture line.20 Type III fractures include those intra-articular fractures of the distal third of the olecranon fossa.20 From review of these 100 cases, Horne et al made treatment recommendations, including favoring the use of plate and screw with tension band fixation in cases of delay of greater than 1 week to decrease the risk of nonunion.20 Extra-articular type I fractures were best treated with excision, whereas intra-articular type I and II fractures should be treated with open reduction and internal fixation with tension band wiring. Recommendations for type IIB fractures involved elevation of the depressed intra-articular fracture and buttressing with bone graft, followed by tension band wiring.20 Type III fractures were best treated with plate and screw fixation to provide optimum rigidity to the construct as tension band wiring was less effective at this location.20
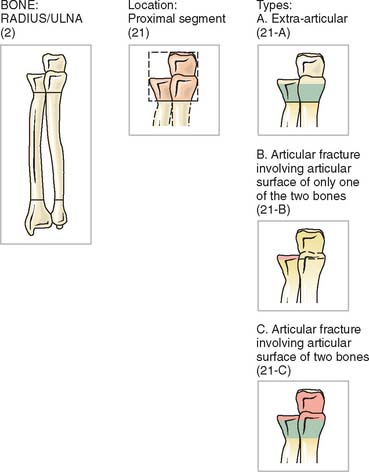
The AO classification system (Fig. 25-1) accounts for both proximal radius and proximal ulna fractures as fracture site 2 for radius/ulna, and 21 for the proximal segment of the radius and ulna. Type A fractures are extra-articular, type B are intra-articular fractures involving the articular surface of either the radius or the ulna, and type C are those involving the articular surface of both bones. Additional subtypes denote comminution, displacement, and location.32 Although the AO classification may be useful for research purposes, it is not commonly used in clinical practice.
Morrey classified olecranon fractures according to criteria regarding stability, comminution, and displacement.8,31 The Mayo Classification (Fig. 25-2) thus divides olecranon fractures into three types, facilitating classification and providing an algorithm for treatment.8,31
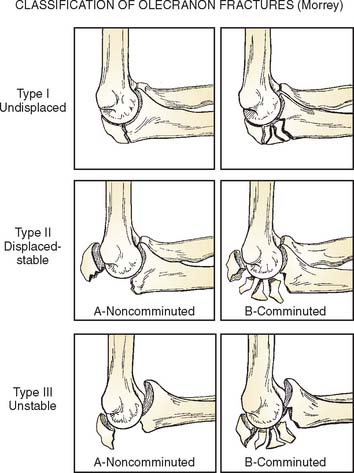
Type I, undisplaced fractures as defined by the Colton criteria earlier, may be subdivided into type IA, noncomminuted fractures, and type IB, comminuted fractures.31 These fractures represent approximately 5% of olecranon fractures. Because these fractures are by definition nondisplaced, the practical significance of the degree of comminution is not significant and types IA and IB may essentially be regarded and treated as the same lesion.31
Mayo type II fractures are the most common type, representing about 85% of olecranon fractures.27,31,38 These fractures, which are stable fractures with greater than 3 mm of displacement, may be noncomminuted (type IIA) or comminuted (type IIB).31 Because the collateral ligaments are intact, the forearm is stable relative to the humerus.31
Mayo Type III fractures are unstable, displaced fractures and represent a fracture-dislocation. Like types I and II, type III fractures may be subclassified into noncomminuted (IIIA) or comminuted (IIIB) types.8,31
COMPLEX OLECRANON FRACTURE-DISLOCATIONS
Olecranon fractures associated with subluxation of the radial head and/or the coronoid process are typically multifragmentary, complex injuries.12,35,37 Anterior fracture dislocations are often referred to transolecranon fracture-dislocations, because the mechanism of injury appears to involve anterior displacement of the forearm, resulting in the trochlea being driven through the olecranon process.12,35,37 The radial head is displaced anteriorly, and this injury is differentiated from the Bado type I Monteggia fracture by the presence of ulnohumeral joint destabilization with preservation of the radioulnar relationship.35,37 Posterior fracture dislocations of the olecranon are more similar to type II Monteggia fractures, with posterior dislocation of the radial head, an apex posterior fracture of the ulna, and similar implications for the stability and function of both the ulnohumeral joint as well as the forearm.12,35 These fractures may be considered a variant of the posterior Monteggia lesion.12 Both posterior and anterior variants are commonly associated with fractures of the coronoid, which are usually basal fractures involving 50% to 100% of the height of the coronoid.35 In anterior olecranon fracture-dislocations, reduction of the olecranon and coronoid fracture fragments results in restoration of stability, with little implication for forearm dysfunction. Posterior olecranon fracture-dislocations, in contrast, have important implications, with elbow instability and forearm dysfunction being common despite fracture reduction.35
TREATMENT
The Mayo Classification provides a basis for a rational treatment algorithm by fracture type and subtype, and conveys prognostic value.31,38
Nondisplaced fractures (Mayo type I) may be treated symptomatically and nonoperatively with 7 to 10 days of immobilization in midflexion and neutral rotation, followed by initiation of an active range of motion program.6,8,17,31 Restrictions on active resisted elbow extension and weight bearing should be maintained for 6 to 8 weeks, with gradual increases in these activities as tolerated.6 Close follow-up with radiographs at 1, 2, and 4 weeks is recommended to assess for displacement and possible need for further intervention.7 Rarely, in select patients, type I fractures may benefit from open reduction and internal fixation to allow immediate motion and stability.8,31 Some type I fractures may be treated with immobilization in a long arm cast at 90 degrees of flexion for 3 to 4 weeks.7 Thereafter, protected range of motion with avoidance of flexion greater than 90 degrees until radiographic evidence of bony healing occurs, usually at 6 to 8 weeks, is recommended.7 Range-of-motion exercises may be commenced at an earlier time point in select patients, such as the elderly, in whom stiffness occurs more frequently.7
Displaced fractures (Mayo type II and III) usually require surgical intervention.6,8,17 Goals of surgical management include restoring the articular congruity and stability of the elbow, maintaining extension power, and providing stable anatomic fixation such that early range of motion is possible, thereby lessening the risk of stiffness.7,16,17,21 Options include excision or open reduction and internal fixation with a variety of devices including tension band wiring, intramedullary screw placement, plate and screw constructs, or bioabsorbable pins.4,6,15,17,27,31,38
SURGICAL MANAGEMENT OPTIONS
Excision
Excision of fracture fragments with advancement and reinsertion of the triceps tendon may be indicated in cases of nonunion, patients who are elderly or who have poor soft tissue viability, avulsion-type extra-articular fractures, and in cases with severe comminution as in Mayo type IIB fractures (Fig. 25-3).7,10,11,13,15,31 Disadvantages of excision include subsequent risks of triceps weakness, instability, stiffness, and a theoretical risk for increased arthrosis due to altered contact pressures.2,7,11,24,29 However, excision obviates risk of nonunion, hardware failure, or prominence, and others suggest a decreased risk of post-traumatic arthritis, because the possibility of incongruity of the articular surface reduction is eliminated with excision of the fragment rather than reduction and fixation.11,17,15
McKeever and Buck determined that one may excise up to 80% of the olecranon without sacrificing stability if the coronoid and anterior soft tissues are intact.7,15,28 If anterior damage is present, instability is a sequelae if too much proximal ulna is excised.7 In addition, An et al2 noted increasing instability of the elbow with olecranon excision, and data from the Mayo laboratory suggest that resection should be limited to 30% of the olecranon. Kamineni et al24 investigated the impact of olecranon resection on stability in relation to posteromedial stresses in a cadaveric model. Resection of osteophytes and proximal ulna was performed to simulate treatment of posteromedial osteophytes, such as in throwing athletes. The investigators noted a clinically significant level of instability with valgus stresses following resection of as little as 6 mm of posteromedial olecranon.24 The authors speculated that this instability may not be clinically relevant in low-demand, elderly patients, but it may be problematic in higher demand athletes or active patients or laborers.24 The increased instability may place increased stress upon the medial collateral ligament, predisposing to possible failure.24 However, excision is usually used in older, low demand patients who may not place such demands on their elbows.
Many authorities recommend reattachment of the triceps at the level of the articular surface.7,11 However, one recent study suggests that attachment more posteriorly results in improved extension strength.11 Didonna et al11 studied variable positions for triceps reattachment following partial olecranon (50%) excision for simulated olecranon fracture in a cadaveric model. Loads were applied along the triceps mechanism at 45 degrees, 90 degrees, and 135 degrees, and the resultant forces were recorded. A significant decrease in extension strength with anterior placement of the triceps relative to normal and relative to posterior placement was noted, with the differences greatest with increasing extension. In contrast, posterior reattachment was noted to result in decreased extensor strength only at 90 degrees. Therefore, the authors recommended more posterior reattachment sites to minimize loss of extension strength.11
Although some authors report less post-traumatic arthritis with excision due to avoiding an incongruent joint, some speculate that excision may lead to increased risk of post-traumatic arthrosis.29 In a cadaveric model with 50% olecranon osteotomy to simulate an olecranon fracture, peak forces across the ulnohumeral joint were measured following either excision of the proximal fragment or open reduction and internal fixation with tension band wiring.29 Elbows fixed with tension band wiring had no significant difference in peak ulnohumeral pressures when compared with the intact elbow joint.28 In contrast, elbows with excision of the proximal fragment were noted to have significant increases in joint forces over the medial and lateral articular surfaces.29 The authors theorized that open reduction and internal fixation with tension band wiring restores the normal biomechanics of the elbow, whereas excision results in abnormal joint forces, which may predispose to arthrosis.29 As such, Moed et al29 favored open reduction and internal fixation in cases in which a large proximal fragment is present.
Nevertheless, satisfactory clinical outcomes (see Fig. 25-3A to C) have been described for treatment of olecranon fracture by excision when used in appropriate patient populations.10,13,15,17 Gartsman17 noted equivalent range of motion, functional status, extensor strength, pain, stability, and incidence of degenerative changes in cases of olecranon fracture treated by open reduction and internal fixation or primary excision.17 In addition, local complications (23% versus 4%) and requirements for additional procedures (an additional 23%), such as hardware removal, were more common in the patients treated with open reduction and internal fixation.17 Such studies demonstrate that excision is a good option for treatment of the appropriate fracture in the appropriately selected patient.
INTERNAL FIXATION
Biomechanics of Internal Fixation
Fyfe et al16 investigated rigidity of various methods of fixation of transverse, oblique, and simulated comminuted olecranon fractures in a cadaveric model. Tension band wiring with two knots was the most stable fixation construct for simulated transverse fractures, whereas intramedullary screw fixation with or without tension banding was unreliable in restoring stability.16 Oblique osteotomies were best repaired with one-third tubular plate fixation or tension band wiring with two knots; whereas the comminuted fractures were most rigidly fixed with five-hole AO plate and screw fixation. In all cases, either tension band wiring or plate-and-screw fixation yielded fixation sufficiently rigid to withstand forces equivalent to those experienced in vivo with active mobilization of the elbow. For comminuted fractures, plate-and-screw fixation was recommended due to the greater stability noted in this in vitro study.16
Hume et al22 studied outcomes of displaced olecranon fractures treated with either plate or tension band wiring fixation in a prospective randomized trial. Plate fixation was superior with respect to maintenance of reduction without step off or gap (95% versus 47%), radiographic outcomes (86% versus 47% good) and clinical outcomes (63% versus 37% good). Range of motion at 6 months was equivalent.39 Plate fixation required longer operative times but was associated with no increase in complication rates.22 Tension band wiring was complicated with symptomatic hardware prominence in 42%.22
Horner et al21 investigated use of tension band wiring versus one-third tubular plate and screws for fixation of simulated fractures of the most distal portion of the olecranon (Colton type III and Horne type III) in a cadaveric model. These fractures, due to the deforming forces of the forearm flexors, tend to be more unstable than their more proximal counterparts.21 The study demonstrated increased fixation stiffness in those fractures treated with one-third tubular plate fixation (163 N/mm versus 53 N/mm) versus tension band wiring. Therefore, the authors concluded that fixation with plate and screws would better counteract forces exerted by the brachioradialis and the biceps than tension band wiring in this fracture pattern.21
Specific Fixation Techniques
Tension Band Wiring
Tension band wiring is widely used as treatment for most olecranon fracture types (Fig. 25-4).31,38 This technique converts tensile forces across the fracture to compressive forces, which with motion, exert compression across the fracture site.7 Also compared with plate and screw fixation, less soft tissue dissection and periosteal stripping is required.18,20 However, this fixation technique may be associated with hardware complications.38 Owing to the subcutaneous nature and location of the elbow, prominent hardware may be problematic, with large numbers of patients in one series reporting hardware-related pain (24%) and functional difficulties (32%) relieved by hardware removal. Also, pain and functional difficulties post removal were reported by 13% and 15% of patients, respectively.38 Nevertheless, up to 97% good to excellent results have been widely reported with use of tension band wiring using proper technique.41
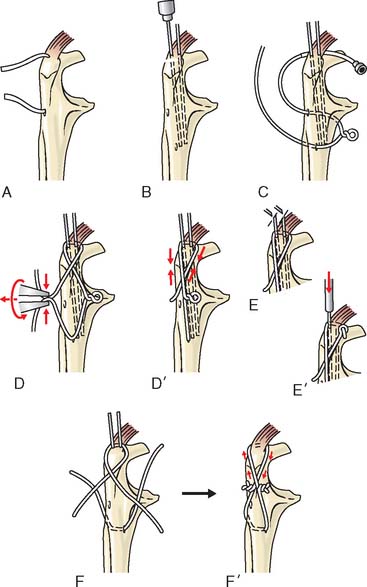
Although there are several proposed modifications of the AO technique that have been suggested to result in increased load to failure, technically easier insertion, and fewer complications, several studies suggest no benefit over the traditional AO technique. Wu et al42 found no difference in the rate of K-wire extrusion or load to failure in a series of cadaveric simulated transverse olecranon fractures fixed either with the traditional AO technique or new modifications. Furthermore, results suggested that loads less than 5.5 kg could be borne postoperatively during repetitive activities of daily living, with single loads not to exceed 8 kg, without adverse consequences.42 Paremain et al36 investigated biomechanics of tension band wiring for fixation of olecranon fractures in a cadaveric model. Simulated transverse olecranon fractures were repaired using two techniques of tension band wiring: the two tightening knot AO technique espoused by Weber and Vasey,40 and the modification to this technique proposed by Rowland and Burkhart.39 Similar mechanisms of failure occurred in both groups, with no statistical significance in load to failure between the groups.39
Tension band wiring may be performed using the standard AO technique (Fig. 25-4).18 Bone reduction clamps reduce the fracture; superficial drill holes in the distal fragment may provide a useful traction site for the jaws of the bone reduction forceps. Following reduction, two parallel 1.6-mm K wires are introduced from the posterior aspect of the olecranon, aiming anteriorly and obliquely just through the anterior cortex. A 2.5-mm hole is drilled transversely in the distal fragment for placement of a 1.0-mm or 1.2-mm cerclage wire with a prefabricated loop; alternatively, two cerclage wires may be used. The wire is then routed under the triceps tendon and K-wires to create a figure-of-eight construct. Tensioning is performed symmetrically on each side. The K-wires are pulled back slightly, cut and bent, and finally the bend ends are impacted into bone.18
Intramedullary Screw Fixation
Intramedullary screw fixation involves placement of a screw down the long axis of the ulnar canal. Ideally, the length of the screw and the width of the threads, which may catch the side cortices, confer sufficient stability for this fixation. However, the screw may compress the fragments, or the fragments may be malrotated. Although stability may be an issue, biomechanical studies suggest favorable features of intramedullary screw fixation for olecranon fractures. Molloy et al30 studied biomechanical features of olecranon fracture fixation with tension band wiring or with intramedullary nail in a cadaveric model. Intramedullary nail fixation was stiffer and had a higher maximum load to failure than did tension band wiring fixation. However, the authors note that this in vitro study fails to replicate important in vivo considerations, such as the potential for damage to the triceps and soft tissues, and the effect of cyclical loading as well as union rate.30 In addition, with intramedullary nailing, the potential for fracture malreduction secondary to off-axis placement of the nail exists.30 Others have reported on unlocked intramedullary screw fixation for olecranon fractures, but higher rates of fixation loss than in tension band wiring have been noted (Fig. 25-5A).19,30 Some have used tension band wiring in conjunction with unlocked intramedullary screws.30
Molloy et al30 investigated biomechanical features of tension band wiring versus intramedullary nail fixation of transverse olecranon fractures. Both tension band wiring and plate-and-screw fixation have high success and union rates; however, owing to painful or prominent hardware, 80% of tension band wiring and 20% of plate-and-screw constructs require removal.30 Intramedullary screw prominence is rarely problematic.
Plate-and-Screw Fixation
Multiple plate-and-screw constructs have been described for the treatment of olecranon fractures (Fig. 25-6).34 Advantages of plate fixation include favorable biomechanics, which can act as a tension band and as a buttress.34 In addition, hardware prominence is less problematic in plate-and-screw constructs relative to tension band wiring fixation.27 Nowinski et al34 described results of treatment of comminuted olecranon fractures with an AO limited contact dynamic compression plate formerly used for wrist fusion. They noted the low-profile but rigid characteristics of this plate were favorable for adaptation to olecranon fracture fixation, and described satisfactory clinical outcomes.34 Bailey et al4 retrospectively reviewed outcomes of plate fixation of olecranon fractures in 25 patients. All of these patients had Mayo type II or III fractures, and satisfactory anatomic reduction was maintained to bony union. Only supination was statistically poorer in the fractured side relative to the normal side; side-to-side differences in range of motion and strength were not statistically significantly different between the fractured and unfractured sides.21 Mayo Elbow Performance Index (MEP) scores were 88% good to excellent, and the DASH scores were consistent with almost normal upper extremities.4 The Short-Form 36 (SF-36) demonstrated no impairment relative to the average American population.4 Twenty percent of patients required hardware removal due to plate prominence, but outcomes were satisfactory with minimal pain and a high degree of patient satisfaction in most cases (see Figs. 25-4 and 25-5).4 Likewise, Anderson et al3 described satisfactory outcomes in 32 patients treated with a congruent elbow plating system following olecranon fracture. At mean 2.2-year follow-up, union rate was 94%. Nine percent of patients had symptomatic hardware, requiring removal. At final follow-up, MEP scores demonstrated 92% good or excellent results, with average arc of motion of 120 degrees.3
Bioabsorbable Fixation
Bioabsorbable fixation may be desirable because of the potential to avoid future operations for hardware removal.5 Patients treated with conventional metal fixation devices have a high likelihood of requiring an additional procedure for removal of bothersome and/or prominent hardware. Bostman et al5 explored costs associated with need for hardware removal. Savings averaged $410 for use of bioabsorbable implants in olecranon fractures when total costs for metallic fixation and subsequent removal were considered. The break-even point was 46% of fractures requiring removal, so that only at more than a 46% removal rate would use of bioabsorbable implants be financially favorable.5 Juutilainen et al23 found equivalent outcomes in patients with olecranon fracture treated with either bioabsorbable implants (poly-L-lactide wire with self-reinforced polyglycolide screws or self-reinforced poly-L-lactide plugs) versus metallic implants (tension band wiring or K-wire plus cerclage wire fixation) and noted cost savings due to avoiding a second operation for hardware removal.23 Further clinical experience is needed to determine the role that bioabsorbable fixation techniques will assume in the future.
PREFERRED TECHNIQUES
For Mayo type I fractures, conservative nonoperative management is preferred (Box 25-1). The patient is placed in sling immobilization for comfort with early active gentle range-of-motion exercises. Close weekly follow-up with radiographs is essential to rule out displacement and need for alternative treatment.
BOX 25-1 Preferred Techniques of Olecranon Fracture Management
Type II and III fractures are best treated surgically with either excision or open reduction and internal fixation (see Figs. 25-3 and 25-5). For fractures with fragments distal to the coronoid, plate-and-screw osteosynthesis is preferred, because these more distal fragments are usually not adequately fixed by tension band wiring. Likewise, more comminuted fractures or oblique patterns are best treated with plate-and-screw fixation to optimize stability.16,21
Excision of fracture fragments is preferred for elderly, low-demand patients (see Fig. 25-3A to C) or those with extensive fracture comminution, or for treatment of nonunions. Tension band wiring using the standard AO technique may be performed for selected patterns amenable to this fixation technique. Otherwise, plate-and-screw osteosynthesis provides the optimal fixation stability with minimal complications (see Fig. 25-4).
Technique for Excision or Open Reduction and Internal Fixation
A midline longitudinal incision is curved over the olecranon to avoid placing the incision over the subcutaneous bone.17 Excision may be performed by sharp dissection of fracture fragments from the triceps aponeurosis, and longitudinal drill holes made through the proximal ulna to secure the triceps tendon down to bone.17 Tension band wiring or plate-and-screw osteosynthesis may be performed using the standard AO technique. The wound is then closed in the standard fashion, and a posterior plaster dressing is applied in full extension. The arm should be elevated overnight and the initial dressing changed on the second day. Active and passive motion is then initiated. Alternatively, if for any reason the operative fixation was believed to be less than optimal, splinting may be continued for 3 to 4 weeks to allow for bony healing at the expense of motion. Protected use of the extremity is maintained with minimal weight bearing and no resistance greater than that of gravity for 6 weeks or until radiographic evidence of healing is seen.
OTHER CONSIDERATIONS
Olecranon fracture-dislocations require special considerations for treatment. Because of inherent instability of these fracture patterns, they are best treated with plate-and-screw osteosynthesis.12,35 One-third tubular plates lack the stiffness necessary to withstand early range of motion and have been associated with early loosening or fatigue fractures.37 Medial and lateral flaps may be raised to access other pathology to bone or ligamentous structures, or concomitant radial head or coronoid fractures may be treated through the window created by the olecranon fracture.35 The plate may be applied over part of the triceps insertion without muscle or periosteal elevation to optimize bone healing, or the triceps may be split longitudinally and mobilized.35 If a concomitant anteromedial coronoid fracture fragment is present, it should be fixed to optimize stability of the elbow.35 When comminution is extensive, a skeletal distractor or temporary external fixation device may be helpful to facilitate reduction; after satisfactory reduction is obtained, definitive fracture fixation using plate and screws with or without augmentation with tension band wiring is usually possible.35,37 If extensive comminution is present such that plate-and-screw fixation does not provide sufficient fracture stability, augmentation with tension band wiring through the triceps insertion may facilitate stable fixation.35
Range-of-motion exercises are ideally initiated within the first 1 to 2 days postoperatively if fracture stability allows.35 More tenuous fixation or fractures in osteoporotic bone, particularly the inherently less stable posterior fracture dislocation patterns, may require support with splinting for up to 4 weeks after surgery.35 The integrity of the lateral collateral ligament and the anteromedial coronoid are important factors in stability of the fracture.35 Ring et al37 noted mostly good to excellent elbow scores following fixation of transolecranon fractures and attributed their low incidence of post-traumatic arthrosis to the nature of the articular surface of the olecranon.37 Restoration of the olecranon and coronoid facets is key because the intervening segment, the transverse ridge of the olecranon, contributes little surface contact area to the articular interface.37
RESULTS
Complications of olecranon fracture include nonunion (see Fig. 25-4A), infection, loss of motion, ulnar nerve symptoms, arthrosis, and need for additional procedures, such as hardware removal.17,26,27,31,33,38 Contracture, especially loss of the terminal 10 to 15 degrees of extension, is particularly common, and appears to be related to immobilization.31 Radiographic evidence of degenerative changes in the ulnohumeral joint has been documented in 20% to 50% of patients up to 15 to 25 years following olecranon fracture.17,26
The risk of prominent and bothersome hardware following tension band fixation may be diminished if wires are bent 180 degrees and impacted into bone, with the triceps securely sutured over wires.27,31 Mullett et al34 noted the effect of K-wire position on backing out of the wire in a clinical series.33 They described an increased risk of back-out when wires were placed down the long axis of the ulna as opposed to crossing the anterior cortex with a concomitant increase in symptomatic hardware, requiring hardware removal (42% versus 11.4%).33 In addition, Mullett et al found a higher pullout strength in a cadaveric investigation in those K-wires placed according to optimal AO specification with transcortical contact (122.7 N versus 56.3 N).33 These clinical and biomechanical data reinforce the importance of use of proper transcortical rather than shaft K-wire placement and adherence to AO technique to avoid potential hardware complications.33
Rommens et al38 described outcomes of surgical fixation of 95 consecutive olecranon fractures treated from 1992 to 2000.38 By type and subtype, 14% were type IA, 8% type IB, 20% IIA; 29% IIB; 11% IIIA; 19% IIIB.38 About one third of patients had concomitant upper extremity fractures.38 Ninety-five percent were treated with tension band wiring constructs, whereas the remainder were treated with plate osteosynthesis.38 Approximately 10% experienced implant migration, 3.2% had delayed union, 2.1% had infection, and 14.7% required additional surgical procedures for complications.38 In addition, two thirds underwent hardware removal at an average of 12 months postoperatively.38 Radiographic changes included intra-articular stepoff without frank arthrosis in 7%; mild to moderate arthrosis in 20%, severe arthrosis in 12%, and pseudoarthrosis in 1%.38 Most patients experienced little or no limitations in pronation or supination (>90% had normal or less than a 10 degree deficit) or flexion (81% had no or less than 10 degrees of deficit); but 46% of patients had a more than 10-degree extension deficit.38 In addition, many patients experienced decreased strength in extension (50%) or flexion (37%).38 Patients with Mayo type III fractures or coexisting lesions of the ipsilateral upper extremity were more likely to have larger deficits in the flexion extension arc than patients with type I or II lesions.38 Likewise, suboptimal fixation was noted to be a risk factor for development of arthrosis, although this may be a confounding factor because both were more commonly seen in more complex fracture patterns.38
Karlsson et al25 investigated long-term outcomes of tension band wiring and figure-of-eight wiring techniques for fixation of olecranon fractures. With respect to all fractures, 96% of patients had a good or excellent outcome up to 25 years after injury and fracture fixation.25 No significant difference between fracture fixation type and subjective outcome was noted.25 Fractures fixed with figure-of-eight wiring were more likely to have impaired pronation, but contralateral reduced pronation was also noted in this group, indicating a possible difference between the groups unrelated to the surgical technique.25 No significant differences in other parameters of range of motion were noted between the groups.25 Follow-up radiographs demonstrated degenerative changes in most of the injured elbows, with subchondral cysts in 45%, subchondral sclerosis in 73%, osteophyte formation in 45%, and joint incongruity in 36%.25 Frank osteoarthritis was noted in 7%.25 When the two groups were compared, subchondral cyst formation (50% versus 39%), subchondral sclerosis (93% versus 54%), and radiographic frank arthrosis (16% versus 5%) were more common in the figure-of-eight wiring group, whereas osteophyte formation 61% versus 50% and joint incongruity (43% versus 29%) were more common in the tension band group.25 Hardware removal was performed in 81% of those elbows treated by tension band wiring and 43% of elbows treated with figure-of-eight fixation.25 Because there were no significant clinical differences between the groups regarding outcome, Karlsson et al recommend use of figure-of-eight wiring for fixation of olecranon fractures because the hardware removal rate was half that of elbows treated with tension band wiring.25
1 Amis A.A., Miller J.H. The mechanisms of elbow fractures: an investigation using impact tests in vitro. Injury. 1995;26:163.
2 An K.N., Morrey B.F., Chao E.Y. The effect of partial removal of the proximal ulna on elbow restraint. Clin. Orthop. Relat. Res. 1986;209:270.
3 Anderson M.L., Larson A.N., Merten S.M., Steinmann S.P. Congruent elbow plate fixation of olecranon fractures. J. Orthop. Trauma. 2007;21:386.
4 Bailey C.S., MacDermid J., Patterson S.D., King G.J. Outcome of plate fixation of olecranon fractures. J. Orthop. Trauma. 2001;15:542.
5 Bostman O.M. Metallic or absorbable fracture fixation devices. A cost minimization analysis. Clin. Orthop. Relat. Res. 1996;329:233.
6 Boyer M.I., Galatz L.M., Borrelli J.Jr., Axelrod T.S., Ricci W.M. Intra-articular fractures of the upper extremity: new concepts in surgical treatment. Instr. Course Lect. 2003;52:591.
7 Bucholz R.W., Heckman J.D., editors. Rockwood and Green’s Fractures in Adults, 5th ed., Philadelphia: Lippincott, Williams & Wilkins, 2001.
8 Cabenela M.E., Morrey B.F. Fractures of the olecranon. In: Morrey B.F., editor. The Elbow and its Disorders. Philadelphia: W. B. Saunders Co; 2000:365-379.
9 Colton C.L. Fractures of the olecranon in adults: classification and management. Injury. 1973;5:121.
10 Compton R., Bucknell A. Resection arthroplasty for comminuted olecranon fractures. Orthop. Rev. Relat. Res. 1989;18:189.
11 Didonna M.L., Fernandez J.J., Lim T.H., Hastings H.2nd, Cohen M.S. Partial olecranon excision: the relationship between triceps insertion site and extension strength of the elbow. J. Hand Surg. Am. 2003;28:117.
12 Doornberg J., Ring D., Jupiter J.B. Effective treatment of fracture-dislocations of the olecranon requires a stable trochlear notch. Clin. Orthop. Relat. Res. 2004;429:292.
13 Estourgie R.J., Tinnemans J.G. Treatment of grossly comminuted fractures of the olecranon by excision. Neth. J. Surg. 1982;34:127.
14 Evans M.C., Graham H.K. Olecranon fractures in children: Part 1: a clinical review; Part 2: a new classification and management algorithm. J. Pediatr. Orthop. 1999;19:559.
15 Fern E.D., Brown J.N. Olecranon advancement osteotomy in the management of severely comminuted olecranon fractures. Injury. 1993;24:267.
16 Fyfe I.S., Mossad M.M., Holdsworth B.J. Methods of fixation of olecranon fractures. An experimental mechanical study. J. Bone Joint Surg. Br. 1985;67:367.
17 Gartsman G.M., Sculco T.P., Otis J.C. Operative treatment of olecranon fractures. Excision or open reduction with internal fixation. J. Bone Joint Surg. Am. 1981;63:718.
18 Heim U. Forearm and hand/miniimplants. In: Mueller M.E., editor. Manual of Internal Fixation: Techniques Recommended by the AO ASIF Group. New York: Springer Verlag, 1991.
19 Helm R.H., Hornby R., Miller S.W. The complications of surgical treatment of displaced fractures of the olecranon. Injury. 1987;18:48.
20 Horne J.G., Tanzer T.L. Olecranon fractures: a review of 100 cases. J. Trauma. 1981;21:469.
21 Horner S.R., Sadasivan K.K., Lipka J.M., Saha S. Analysis of mechanical factors affecting fixation of olecranon fractures. Orthopedics. 1989;12:1469.
22 Hume M.C., Wiss D.A. Olecranon fractures. A clinical and radiographic comparison of tension band wiring and plate fixation. Clin. Orthop. Relat. Res. 1992;285:229.
23 Juutilainen T., Pätiälä H., Rokkanen P., Törmälä P. Biodegradable wire fixation in olecranon and patella fractures combined with biodegradable screws or plugs and compared with metallic fixation. Arch. Orthop. Trauma Surg. 1995;114:319.
24 Kamineni S., Hirahara H., Pomianowski S., Neale P.G., O’Driscoll S.W., ElAttrache N., An K.N., Morrey B.F. Partial posteromedial olecranon resection: a kinematic study. J. Bone Joint Surg. Am. 2003;85-A:1005.
25 Karlsson M.K., Hasserius R., Besjakov J., Karlsson C., Josefsson P.O. Comparison of tension-band and figure-of-eight wiring techniques for treatment of olecranon fractures. J. Shoulder Elbow Surg. 2002;11:377.
26 Karlsson M.K., Hasserius R., Karlsson C., Besjakov J., Josefsson P.O. Fractures of the olecranon: a 15- to 25-year followup of 73 patients. Clin. Orthop. Relat. Res. 2002;403:205.
27 McKay P.L., Katarincic J.A. Fractures of the proximal ulna olecranon and coronoid fractures. Hand Clin. 2002;18:43.
28 McKeever F.M., Buck R.M. Fracture of the olecranon process of the ulna: treatment by excision of fragment and repair of triceps tendon. J. A. M. A. 1947;135:1.
29 Moed B.R., Ede D.E., Brown T.D. Fractures of the olecranon: an in vitro study of elbow joint stresses after tension-band wire fixation versus proximal fracture fragment excision. J. Trauma. 2002;53:1088.
30 Molloy S., Jasper L.E., Elliott D.S., Brumback R.J., Belkoff S.M. Biomechanical evaluation of intramedullary nail versus tension band fixation for transverse olecranon fractures. J. Orthop. Trauma. 2004;18:170.
31 Morrey B.F. Current concepts in the treatment of fractures of the radial head, the olecranon, and the coronoid. Instr. Course Lect. 1995;44:175.
32 Muller M.E., Allgower M., Schneider R., Willenegger H. Comprehensive classification of fractures of long bones. In Manual of Internal Fixation: Techniques Recommended by the AO-ASIF Group, 3rd ed., New York: Springer-Verlag; 1991:118-150.
33 Mullett J.H., Shannon F., Noel J., Lawlor G., Lee T.C., O’Rourke S.K. K-wire position in tension band wiring of the olecranon—a comparison of two techniques. Injury. 2000;31:427.
34 Nowinski R.J., Nork S.E., Segina D.N., Benirschke S.K. Comminuted fracture-dislocations of the elbow treated with an AO wrist fusion plate. Clin. Orthop. Relat. Res. 2000;378:238.
35 O’Driscoll S.W., et al. Difficult elbow fractures: pearls and pitfalls. Instr. Course Lect. 2003;52:113.
36 Paremain G.P., et al. Biomechanical evaluation of tension band placement for the repair of olecranon fractures. Clin. Orthop. Relat. Res. 1997;335:325.
37 Ring D., Jupiter J.B., Sanders R.W., Mast J., Simpson N.S. Transolecranon fracture-dislocation of the elbow. J. Orthop. Trauma. 1997;11:545.
38 Rommens P.M., Schneider R.U., Reuter M. Functional results after operative treatment of olecranon fractures. Acta Chir. Belg. 2004;104:191.
39 Rowland S.A., Burkhart S.S. Tension band wiring of olecranon fractures. A modification of the AO technique. Clin. Orthop. Relat. Res. 1992;277:238.
40 Weber B.G., Vasey H. [Osteosynthesis in olecranon fractures.]. Z. Unfallmed. Berufskr.. 1963;56:90.
41 Wolfgang G., Burke F., Bush D., Parenti J., Perry J., LaFollette B., Lillmars S. Surgical treatment of displaced olecranon fractures by tension band wiring technique. Clin. Orthop. Relat. Res. 1987;224:192.
42 Wu C.C., Tai C.L., Shih C.H. Biomechanical comparison for different configurations of tension band wiring techniques in treating an olecranon fracture. J. Trauma. 2000;48:1063.






