Chapter 379 Foreign Bodies of the Airway
Epidemiology and Etiology
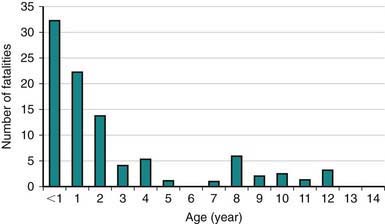
Infants and toddlers use their mouths to explore their surroundings. Most victims of foreign body aspiration are older infants and toddlers (Fig. 379-1). Children <3 yr of age account for 73% of cases. Preambulatory toddlers can aspirate objects given to them by older siblings. One third of aspirated objects are nuts, particularly peanuts. Fragments of raw carrot, apple, dried beans, popcorn, and sunflower or watermelon seeds are also aspirated, as are small toys or toy parts.
Clinical Manifestations
Three stages of symptoms may result from aspiration of an object into the airway:
379.1 Laryngeal Foreign Bodies
Complete obstruction asphyxiates the child unless it is promptly relieved with the Heimlich maneuver (Chapter 62 and Figs. 62-6 and 62-7). Objects that are partially obstructive are usually flat and thin. They lodge between the vocal cords in the sagittal plane, causing symptoms of croup, hoarseness, cough, stridor, and dyspnea.
379.3 Bronchial Foreign Bodies
Radiologic evaluation—posteroanterior and lateral chest radiographs—are standard in the assessment of infants and children suspected of having aspirated a foreign object. The abdomen is included. A good expiratory posteroanterior chest film is most helpful. During expiration the bronchial foreign body obstructs the exit of air from the obstructed lung, producing obstructive emphysema, air trapping, with persistent inflation of the obstructed lung and shift of the mediastinum toward the opposite side (Fig. 379-2). Air trapping is an immediate complication, in contrast to atelectasis, which is a late finding. Lateral decubitus chest films or fluoroscopy can provide the same information but are unnecessary. History and physical examination, not radiographs, determine the indication for bronchoscopy.

American Academy of Pediatrics Committee on Injury, Violence, and Poison Prevention. Policy statement—prevention of choking among children. Pediatrics. 2010;125:601-607.
Cohen S, Avital A, Godfrey S, et al. Suspected foreign body inhalation in children: what are the indications for bronchoscopy? J Pediatr. 2009;155:276-280.
Kadmon G, Stenr T, Bron–Harley E, et al. Computerized scoring system for the diagnosis of foreign body aspiration in children. Ann Otol Rhinol Laryngol. 2008;117(11):839-843.
Milkovich SM, Altkorn R, Chen X, et al. Development of the small parts cylinder: lessons learned. Laryngoscope. 2008;118(11):2082-2086.
Nova A, Muntz H, Clary R. Utility of conventional radiography in pediatric airway foreign bodies. Ann Otol Rhinol Laryngol. 1998;107:834-838.
Shah RK, Patel A, Lander L, et al. Management of foreign bodies obstructing the airway in children. Arch Otolaryngol Head Neck Surg. 2010;136(4):373-379.
Wang K, Harnden A, Thomson A. Foreign body inhalation in children. BMJ. 2010;341:455-456.





