Chapter 7 Fluid Therapy
2 What are sensible and insensible fluid losses? How are maintenance fluid requirements calculated?







3 What are fluid maintenance requirements for children?
Twenty-four–hour fluid requirements for children have been formulated on the basis of weight:












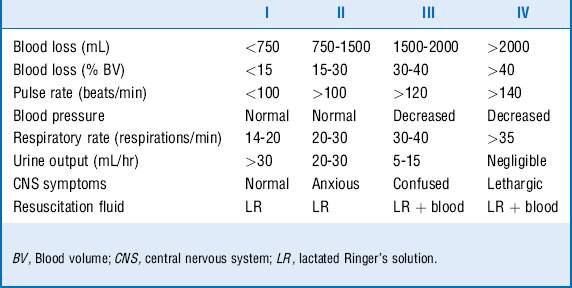
6 What is the 3:1 rule in fluid therapy after acute blood loss?
Three milliliters of crystalloid is given for each milliliter of blood loss to compensate for administered fluid that is lost into the interstitial and intracellular spaces. This is a starting dose. Most patients need more than this and will need 5:1 to restore normovolemia. Please see Chapter 54 for description of blood replacement in patients who require massive transfusions (greater than 10 U of packed red blood cells).




8 What is the difference between crystalloids and colloids? Give examples of each


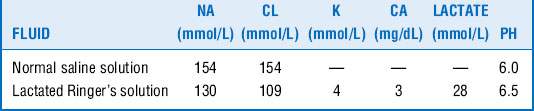
9 Describe the composition of normal saline and lactated Ringer’s solution. Which should be used for acute resuscitation?
Table 7-2 summarizes the composition of normal saline and lactated Ringer’s solution. Lactated Ringer’s solution is preferable for acute volume replacement because normal saline solution can result in hyperchloremic metabolic acidosis.



Acknowledgement
Key Points Fluid Therapy
1. Total body water is 60% of body weight (40% intracellular and 20% extracellular). Plasma (blood) volume is 5% of body weight.
2. Diagnose volume deficit or excess by clinical examination, not laboratory study results.
3. Avoid fluid and electrolyte abnormalities by measuring and replacing ongoing gastrointestinal losses with appropriate fluids.
4. Use lactated Ringer’s solution for acute volume resuscitation.
5. There is no proved benefit to colloid over crystalloid in acute resuscitation.
1 Alderson P., Bunn F., Lefebvre C., et al. Albumin Reviewers: Human albumin solution for resuscitation and volume expansion in critically ill patients. Cochrane Database System Rev. 4, 2004. CD001208
2 Fan E., Stewart T.E. Albumin in critical care: SAFE but worth the salt? Crit Care. 2004;8:297–299.
3 Perel P., Roberts I. Colloids versus crystalloids for fluid resuscitation in critically ill patients. Cochrane Database System Rev. 3, 2011. CD000567
