13 Femoral Block
Traditional Block Technique
Placement
Anatomy
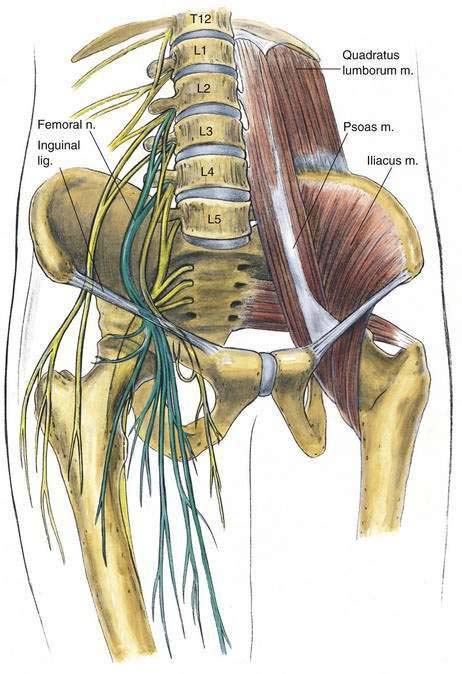
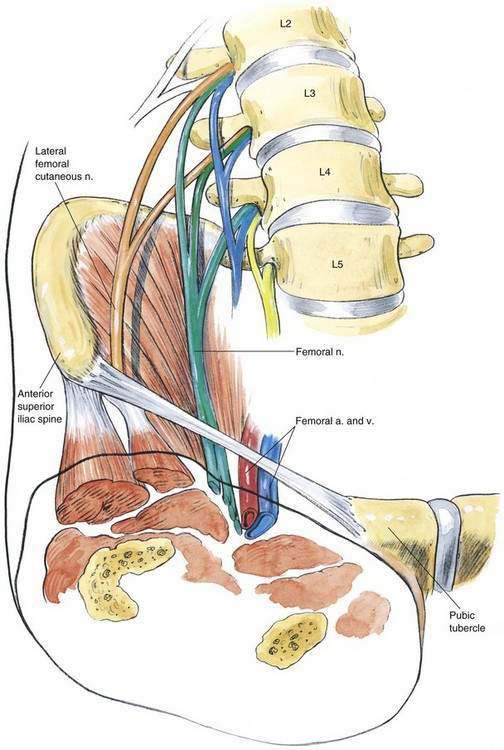
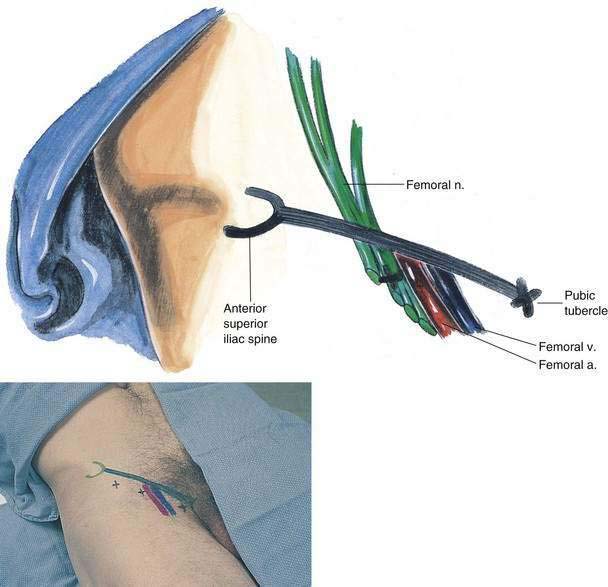
The femoral nerve travels through the pelvis in the groove between the psoas and the iliacus muscles, as illustrated in Figure 13-1. It emerges beneath the inguinal ligament, posterolateral to the femoral vessels, as illustrated in Figure 13-2. It frequently divides into its branches at or above the level of the inguinal ligament.
Needle Puncture
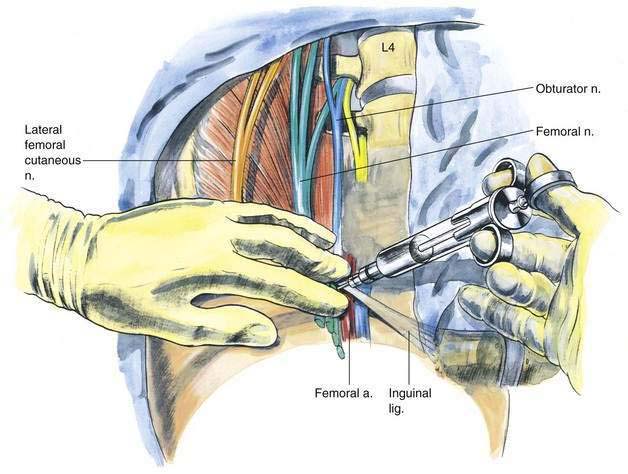
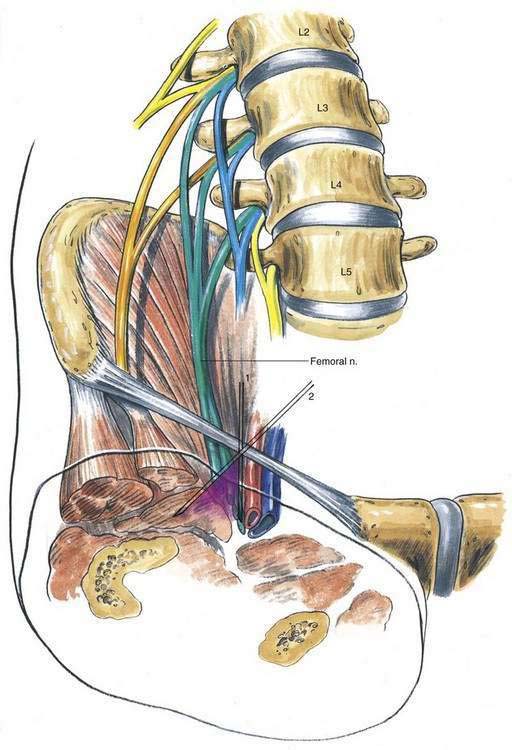
A line is drawn connecting the anterior superior iliac spine and the pubic tubercle, as illustrated in Figure 13-3. The femoral artery is palpated on this line, and a 22-gauge, 4-cm needle is inserted, as illustrated in Figure 13-4. The initial insertion should abut the femoral artery in a perpendicular fashion, as shown in Figure 13-5 (position 1); a “wall” of local anesthetic is developed by redirecting the needle in a fanlike manner in progressive steps to position 2. (Ultrasonography highlights that the nerve is deep to the fascia iliaca, something difficult to appreciate without imaging guidance.) Approximately 20 mL of local anesthetic is injected incrementally in this fashion. It may also be useful to displace the needle entry site laterally 1 cm, direct the needle tip to lie immediately posterior to the femoral artery, and then inject an additional 2 to 5 mL of drug. This allows block of those fibers that may be in a more posterior relationship to the femoral artery. Elicitation of paresthesia is variable with this block; however, if one does occur, the mediolateral injection should still be carried out because the nerve often divides into branches cephalad to the inguinal ligament.
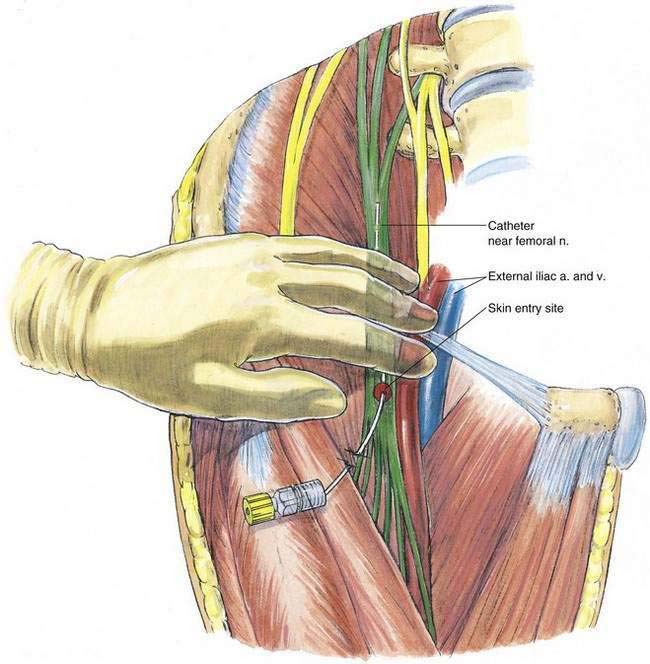
When using a continuous catheter technique, either stimulating catheter block kits or traditional epidural needles and matched catheters may be used in adults (Fig. 13-6). In the latter situation, the epidural needle is positioned either with the assistance of a nerve stimulator or with paresthesia elicitation as an end point. After the needle is positioned, 20 mL of preservative-free normal saline solution is injected through the needle, and then the appropriate-size catheter is inserted approximately 10 cm past the needle tip. Once the catheter has been secured with a plastic occlusive dressing, the initial bolus injection of drug is carried out and the infusion is started.
Ultrasonography-Guided Technique
The transducer should be placed in the infrainguinal region (Fig. 13-7) with the goal of imaging the femoral artery in its true short axis (i.e., it appears as a complete circle). If the patient is obese or there is difficulty locating the femoral artery, engaging the Doppler function may help in locating the femoral artery as a pulsatile structure.
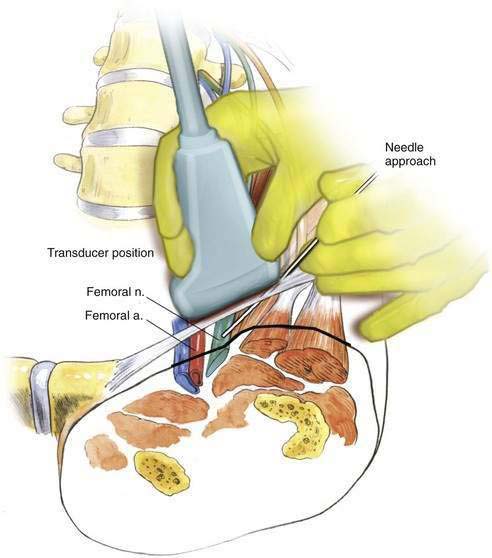
Once the artery has been located, the nerve can be identified as an oval hyperechoic structure lying just lateral to the artery (Fig. 13-8). A key structure to identify is the fascia iliaca, which appears as a hyperechoic line extending off the iliopsoas muscle. The local anesthetic must be injected below the fascia iliaca to generate an effective block.
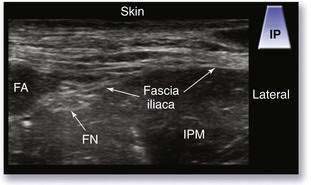
The needle is inserted at a roughly 45-degree angle using the in-plane technique, as depicted in Figure 13-7. The primary objective for this block is to visualize the needle or needle-related motion puncturing below the fascia iliaca and adjacent to the femoral nerve (see Fig. 13-7). There is a characteristic spread of local anesthetic (Fig. 13-9; see Fig. 13-8), which confirms correct needle tip location (see Video 10: Femoral Nerve Block: Correct Spread of Local Anesthetic Under the Fascia Iliaca on the Expert Consult Website). 

Figure 13-9. Ultrasonography-guided femoral nerve block: spread of local anesthetic. FA, femoral artery; FN, femoral nerve.
Pearls
There is no reason the needle must contact the femoral nerve with this block. When the local anesthetic is deposited under the fascia iliaca, a solid block should result. As shown in Figure 13-7, I often inject 1 to 3 cm lateral to the femoral nerve (see Video 11: Femoral Nerve Block: In-Plane Technique on the Expert Consult Website).