Chapter 41 Fastlok Device for Tibial Fixation of a Tripled or Quadrupled Semitendinosus Autograft for Anterior Cruciate Ligament Reconstruction
Introduction
The number of surgeons using hamstring tendons for anterior cruciate ligament (ACL) reconstruction has continuously increased in the past years. As a result, various modifications associated with graft preparation and fixation have been introduced. However, despite these variations in technique, the goal of reconstructing a strong and viable graft with a dependable fixation system remains unaltered. The standard means by which mechanical fixation of hamstring grafts is achieved can either be through direct (interference screws) or indirect (Endobutton [Smith & Nephew, Andover, MA] or screw and washer) techniques. Direct fixation is achieved with an interference screw. With this technique, factors such as divergence, direction of screw placement, the geometry and material composition of the screw, and the graft and tunnel characteristics should be considered to increase the likelihood of a successful outcome.1,2
Indirect fixation techniques, on the other hand, require a linkage material (tape or suture) that would connect the graft tissue to the fixation device. Factors to consider with this technique include: (1) the strength and stiffness of the linkage material to minimize both the potential for elongation of the graft-fixation device construct3–5 and graft-tunnel motion6–8 and (2) the distance of graft fixation from the joint line, which can also influence graft-tunnel motion, especially with early stress on the graft during aggressive rehabilitation. The farther the fixation site from the joint line, the greater the creep of the graft-fixation device construct.2,5
Scientific Rationale
A variety of options are available for hamstring tendon graft tibial fixation during ACL reconstruction. These include different types of washers (AO, Washerloc, and Spiked Washer), staples, suture/post, and bioabsorbable screws.9–12 Ideally, the type of fixation chosen should provide the strength and stiffness necessary to withstand failure during cyclical loading, allow the strands to be equally tensioned and compressed into the tibial tunnel wall, and also have the provision for removal when the need arises for revision reconstruction.
The use of only the semitendinosus tendon for ACL reconstruction minimizes the possibility of having subsequent flexor weakness from the disruption of the hamstring muscle. With the quadrupled configuration of this graft construct, indirect fixation is usually required because of the total length of the graft achieved.13,14 In the description of the technique that follows, the Fastlok device is combined with a tibial tunnel bone plug that provides additional tunnel compression, which facilitates tendon to bone healing and at the same time reduces the risk for tunnel widening by limiting the sagittal motion of the graft.15 The Fastlok, on the other hand, offers the ease of using a simple threading technique during application, which helps the graft to retain tension throughout the fixation procedure. In addition, it also minimizes slippage with the staple and buckle fixation, reducing the risk of suture and graft loosening while at the same time maintaining a low profile, which is very important considering the relatively thin soft tissues that cover the involved area of the medial aspect of the proximal tibia.
Surgical Technique
The graft is then prepared at the back table, as described in Chapter 16, “Hamstring Anterior Cruciate Ligament Reconstruction with a Quadrupled or Tripled Semitendinosus Tendon Graft.”
Tunnel Preparations and Graft Fixation
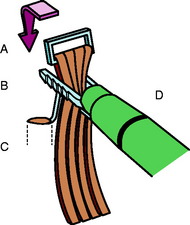
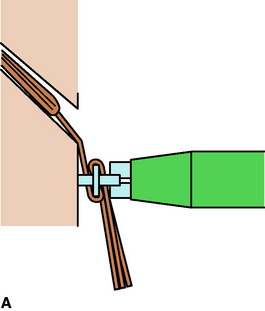
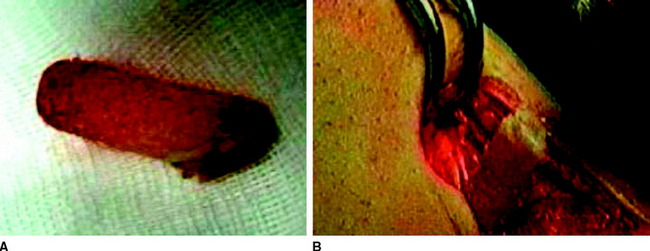
The polyester tapes are initially passed through the buckle component, which is subsequently flipped. The two prongs of the staple are then threaded through the buckle (Fig. 41-1). Then, with the knee in 30 degrees of flexion, the surgical assistant holds the buckle with a forceps in a flipped position while holding the ends of the tape with the other hand. The Fastlok device is then pressed against the tibia. Once the Fastlok is in position, an impactor is used to drive the staple down in a perpendicular manner. During this step, it is important to maintain the graft’s tension. The protruding portion of the tape is trimmed, and the device is further impacted as needed to achieve a low profile for the device (Fig. 41-2, A–C). Finally, the bone plug obtained from reaming the tibial tunnel is impacted back into the tibia (Fig. 41-3, A, B). Arthroscopic assessment of the graft position during flexion and extension is carried out to make sure that no graft impingement exists.

Results
In a biomechanical study conducted to analyze the mechanical properties of linkage systems used in hamstring tendon ACL reconstruction,10 three constructs (5-mm braided polyester [Mersilene], double-loop; 3-mm woven polyester [Orthotape], double-loop; and 3-mm Orthotape, single-loop—all connected to the Fastlok fixation device in bovine bone sections) were compared using an Instron tensile test machine to document their pull tensile strength, residual tensile strength, and fatigue strength at a loading regimen of 540,000 cycles at 25-Hz frequency.
Troubleshooting
Achieving a stable and reproducible technique for tibial fixation is always a challenge for most surgeons. Although good results have been obtained with the use of conventional staples, certain aspects of both the device and the technique of achieving fixation can be improved. One of the main concerns when using staples for tibial fixation involves the occurrence of slippage. Because this is not immediately apparent at the time of surgery, the surgeon can only do so much in averting this problem. However, in cases in which proper tension is not achieved or the graft is found to be loose after the staple has been placed, the surgeon has no choice but to remove the staple and reapply it with proper tension. To minimize this problem, we recommend the use of a staple device in combination with a buckle (e.g., Fastlok). The addition of this simple component facilitates tensioning and locks the graft in position while the staple is driven down the tibia (see Figs. 41-1 and 41-2). The device can be easily fixed, assuming the surgeon maintains a perpendicular position while driving the Fastlok to the tibia. Concerns regarding the prominence of the device are addressed by allowing sufficient soft tissue coverage over the staple prior to skin closure. Moreover, once the graft has healed, removal of the staple remains an option.
1 Bickerstaff D. BASK instructional lecture 4: anterior cruciate ligament graft fixation. Knee. 2001;8:79-81.
2 Kurosaka M, Yoshiya S, Andrish JT. A biomechanical comparison of different surgical techniques of graft fixation in anterior cruciate ligament reconstruction. Am J Sports Med. 1987;15:225-229.
3 Brand JJr, Weiler A, Caborn DNM, et al. Graft fixation in cruciate ligament reconstruction. Am J Sports Med. 2000;28:761-774.
4 Cooley VJ, Deffner KT, Rosenberg TD. Quadrupled semitendinosus anterior cruciate ligament reconstruction: 5 year results in patients without meniscus loss. Arthroscopy. 2001;17:795-800.
5 Ishibashi, Y, Rudy TW, Kim HS, et al. The effect of anterior cruciate ligament graft fixation site at the tibia on knee stability: evaluation using robotic testing system. Arthroscopy. 1997;13:177-182.
6 Frank CB, Jackson DW. The science of reconstruction of the anterior cruciate ligament. J Bone Joint Surg. 1997;79A:1556-1576.
7 Gobbi A, Panuncialman I. Quadrupled bone-semitendinosus ACL reconstruction: a prospective clinical investigation in 100 patients. J Orthop Traumatol. 2003;3:120-125.
8 Hoher J, Livesay GA, Ma CB, et al. Hamstring graft motion in the femoral bone tunnel when using titanium button/polyester tape fixation. Knee Surg Sports Traumatol Arthrosc. 1999;7:215-219.
9 Brown CHJr, Sklar JH. Endoscopic anterior cruciate ligament reconstruction using quadrupled hamstring tendons and Endobutton femoral fixation. Tech Orthop. 1998;13:281-298.
10 Gobbi A, Mahajan S, Tuy B, et al. Hamstring graft tibial fixation: biomechanical properties of different linkage systems. Knee Surg Sports Traumatol Arthrosc. 2002;10:330-334.
11 Magen HE, Howell SM, Hull ML. Structural properties of six tibial fixation methods for anterior cruciate ligament soft tissue graft. Am J Sports Med. 1999;24:35-43.
12 Weiler A, Scheffler S, Gockenjau A, et al. Different hamstring tendon graft fixation techniques under incremental loading conditions [abstract]. Arthroscopy. 1998;14:425-426.
13 Gobbi A, Domzalski M, Pascual J, et al. Hamstring anterior cruciate ligament reconstruction: is it necessary to sacrifice the gracilis? Arthroscopy. 2005;21:275-280.
14 Gobbi A, Francisco R. Fastlok tibial fixation for hamstring anterior cruciate ligament reconstruction. Tech Orthop. 2005;20:274-277.
15 Fu FH, Bennett CH, Ma B, et al. Current trends in anterior cruciate ligament reconstruction. Part II: operative procedures and clinical correlations. Am J Sports Med. 2000;28:124-130.
Aune AK, Holm I, Risberg MA, et al. Four-strand hamstring tendon autograft compared with patellar tendon autograft for anterior cruciate ligament reconstruction: a randomized study with two year follow-up. Am J Sports Med. 2001;29:722-728.
Höher 1998 Höher J, Moller HD, Fu FH. Bone tunnel enlargement after anterior cruciate ligament reconstruction: fact or fiction? Knee Surg Sports Traumatol Arthrosc. 1998;6:231-240.
Kousa P, Jarvinen TL, Vihavainen M, et al. The fixation strength of six hamstring tendon graft fixation devices in anterior cruciate ligament reconstruction. Part II: tibial site. Am J Sports Med. 2003;31:182-188.






