Chapter 33 EZLoc Femoral Fixation of a Soft Tissue Graft
Introduction
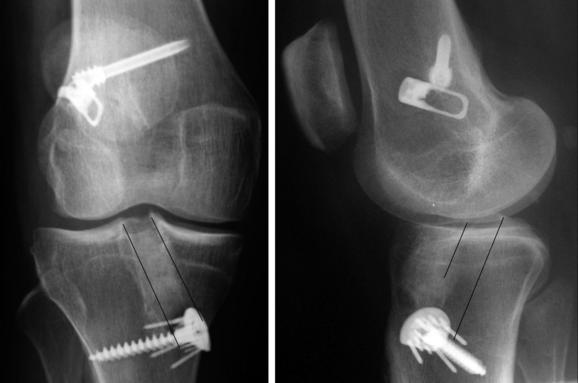
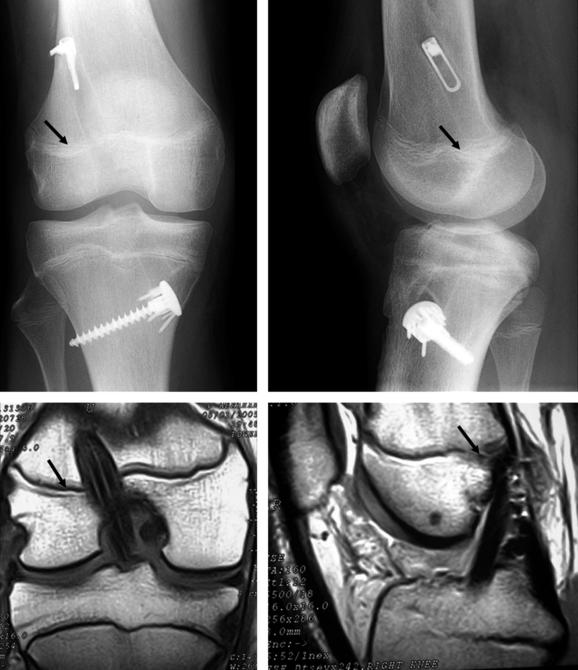
Fixation of the looped end of a soft tissue ACL graft to the femur poses different challenges than fixation of the free ends to the tibia. Metal cross-pin devices such as the Bone Mulch Screw and Transfix have set the standard for femoral fixation because of their superior slippage resistance, stiffness, and strength.1–4 Although these metal cross-pin devices work extremely well, their surgical techniques consists of multiple challenging steps and a lateral incision through the iliotibial band, which can damage the lateral collateral ligament.5 Prominent seating of the head of the cross-pin causes iliotibial band pain,6 and countersinking below the cortex complicates and may prevent hardware removal at the time of revision surgery (Fig. 33-1).
Design, Diameter, Length, Packaging, and Mechanism of the EZLoc
The EZLoc is a cortical fixation device that consists of a deployable lever arm connected to an axle in a slotted body through which the ACL graft is looped. The lever arm grips cortical bone on the anterolateral side of the femur, which provides superior slippage resistance, high stiffness, and strong cortical fixation. The lever arm provides rigid fixation that is better than that of a cross-pin because the lever arm seats on cortical bone on the anterolateral femur, which is 50 times stronger than cancellous bone7 (Fig. 33-2).

The EZLoc comes in different lengths, which control the length of the graft in the femoral tunnel and ensure that enough graft extends beyond the tibial tunnel for secure fixation. The most commonly used EZLoc length is the standard version. The standard version is used in a femoral tunnel from 35 to 50 mm in length, which provides 22 to 37 mm of soft tissue graft in the tunnel, promoting rapid, stiff, and strong tendon tunnel healing.8–10 The long version is used in a femoral tunnel that is longer than 50 mm, and the length of the soft tissue graft in the femoral tunnel is computed by subtracting 22 mm from the length of the lateral wall of the femoral tunnel. The short version is used in a femoral tunnel that is shorter than 35 mm, and the length of the graft in the tunnel is computed by subtracting 7 mm from the length of the lateral wall of the femoral tunnel.
For ease of use, each EZLoc comes preassembled on a 16-inch-long, sharp-tip passing pin that is secured by a suture tied under tension and is sterile (Figs. 33-3 and 33-4). The suture has two functions: to keep the passing pin in the body of the EZLoc during passing of the graft and to deploy the lever arm once the lever arm clears the femoral tunnel. The suture passes through a hole in the lever arm and through two holes at the sharp end of the passing pin. The suture is tied under tension, which keeps the dull end of the passing pin inside the EZLoc and keeps the lever arm undeployed. The lever arm is positioned laterally, tension is applied to the pin, and the EZLoc and soft tissue graft are pulled across the knee. Once the ACL graft is pulled into the femoral tunnel, the suture is cut, the passing pin is removed, the suture is tensioned, and the lever arm deploys.

Fixation Properties of the EZLoc
A successful ACL reconstruction with a soft tissue graft depends on the use of a femoral fixation device that has superior fixation properties and enhances biological healing of the tendon to the tunnel wall. The fixation properties of the femoral fixation device should provide high strength and high stiffness, be resistant to slippage, and allow circumferential healing of the tendon to the tunnel wall.4,9,11–13 Because a soft tissue graft takes longer to heal to the tunnel than a bone plug, the femoral fixation of a soft tissue graft should be more slippage resistant, stiffer, and stronger than the femoral fixation of a bone plug graft.14
The use of the EZLoc to fix a soft tissue graft in the femur is a sound choice because its fixation properties are second to none and the device allows circumferential healing. The strength of the EZLoc is 1427N, which is stronger than the closed-loop Endobutton (1086N) and the cross-pins (Bone Mulch Screw, 1112N; Transfix, 1303N; RigidFix, 868N).2,15 The stiffness of the lever arm of the EZLoc on cortical bone is infinitely high compared with the stiffness of the more elastic soft tissue graft. A benefit of using a high-stiffness femoral fixation device such as the EZLoc is that the tension applied to the graft to restore anterior laxity is lowered4,12,13,16 and the risk of developing anterior laxity during early motion is lessened.11 The slippage resistance of the EZLoc under cyclical loading has not been measured; however, the slippage with a metal lever arm on cortical bone should be at least as small as a cross-pin because the mechanism of looping the graft over a metal post is identical in both types of fixation methods.17 The EZLoc promotes healing of the tendon to the tunnel wall better than an interference screw because the soft tissue graft fixed with the EZLoc heals circumferentially to the tunnel wall.9
The combination of the EZLoc with the WasherLoc and bone dowel tibial fixation device creates a graft-fixation device construct with superior fixation properties that allow an early, aggressive, and brace-free rehabilitation.18 With this fixation technique and correct tunnel placement, the majority of patients regain sufficient function and confidence in their knee to return to preinjury activity level 4 months after reconstruction, similar to femoral fixation with the Bone Mulch Screw.19
Reliable Surgical Technique with Minimal Steps
The EZLoc provides consistent fixation in bone affected by a variety of conditions. Softening of the cancellous bone in the femur from injury, disuse, increased age, smoking, and alcohol use does not affect the fixation properties because the EZLoc is seated on cortical bone. A posterior wall blowout or a thin, 1-mm back wall to the femoral tunnel, which is required so that the tension in the graft matches that of the intact ACL,20 does not affect the fixation performance of the EZLoc in contrast to the interference screw, which requires excessive anterior placement of the femoral tunnel to provide fixation.
Surgical Technique
The surgical technique for fixing a soft tissue ACL graft to the femur with the EZLoc using a single-tunnel, transtibial technique can be viewed in streaming video online (http://www.drstevehowell.com/ezloc_video.cfm) as well as in the DVD and website that accompany this textbook.
Prepare and Size the Hamstring or Tibialis Allograft
Regardless of whether an autogenous hamstring graft or a tibialis allograft is used, the preparation of the tendons requires no special suturing or tensioning for use with the EZLoc. Sew a #1 suture to each end of each tendon. Use the 7- to 8-mm and 9- to 10-mm sizing sticks to determine the diameter of the graft. Loop the graft in the slot of the sizing stick. Pass sleeves of different diameters over the graft. Choose the diameter of the smallest sleeve that can be “thrown” rather than pushed over the looped end of the graft to drill the femoral and tibial tunnels. Store the graft inside the sizing sleeve in a saline basin to keep it moist and to prevent swelling until it is used (Fig. 33-5).

Place the Tibial Tunnel without Posterior Cruciate Ligament and Roof Impingement
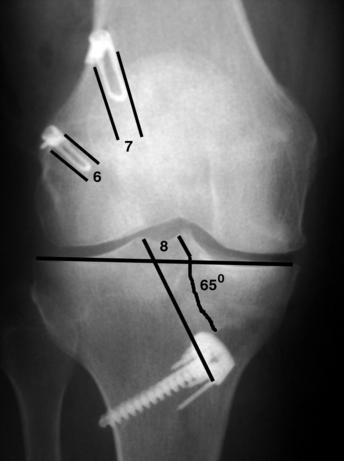
The EZLoc is most easily inserted with use of the transtibial technique, in which the femoral tunnel is drilled through the tibial tunnel (see Chapter 21). Correct placement of the tibial tunnel ensures correct placement of the femoral when the tibial tunnel is drilled with the Howell 65-degree tibial guide (Arthrotek). The 65-degree tibial guide places the ACL graft without posterior cruci-ate ligament (PCL) and roof impingement. A wallplasty is performed until the width between the lateral femoral condyle and PCL exceeds the width of the graft by 1 mm. The tibial tunnel is angled 60 to 65 degrees with the medial joint line, which positions the lateral edge of the tibial tunnel such that it passes through the apex of the lateral tibial spine in the coronal plane to avoid PCL impingement. Because the tibial tunnel is drilled with the knee in full extension and the guide references off the intercondylar roof, the center of the tibial tunnel is placed 5 to 6 mm posterior and parallel to the intercondylar roof with the knee in maximum hyperextension in the sagittal plane, which avoids roof impingement without performing a roofplasty.20–24
Drill the Femoral Tunnel with a 1-Inch Femoral Reamer
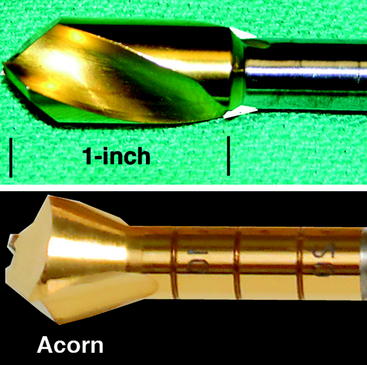
The use of a 1-inch femoral reamer is recommended rather than an acorn-tip reamer because the acorn-tip reamer leaves ridges that can block the passage of the EZLoc. Use a cannulated 1-inch femoral reamer (Arthrotek) that matches the diameter of the ACL graft, and drill the femoral tunnel through the anterolateral cortex of the femur. Draw the reamer in and out along the entire length of the femoral tunnel, including the cortex, two to three times to smooth the tunnel (Fig. 33-6). The EZLoc does not hang up when the femoral tunnel is drilled with the 1-inch femoral reamer.
Measure the Femoral Tunnel and Choose the Length of the EZLoc
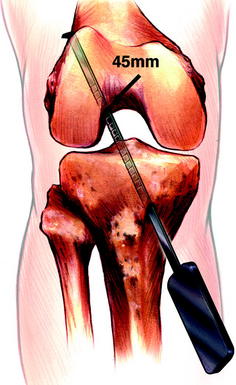
Insert the depth gauge through the tibial tunnel into the femoral tunnel. Hook a tip of the depth gauge on the lateral cortex of the femur. Read the length of the lateral wall of the femoral tunnel at the point where the depth gauge enters the femoral tunnel (Fig. 33-7). Choose a standard EZLoc when the femoral tunnel length is between 35 and 50 mm, a short EZLoc when the femoral tunnel length is less than 35 mm, and a long EZLoc when the femoral tunnel length is greater than 50 mm.
Fix the Soft Tissue Graft to the Femur
The first step in fixing the soft tissue ACL graft to the femur is to insert the passing pin attached to the EZLoc through the tibial tunnel, intercondylar notch, femoral tunnel, and skin overlying the anterolateral thigh. Rotate the passing pin until the gold lever arm faces laterally. Loop the soft tissue ACL graft through the slot in the body of the EZLoc, and tie together the sutures at the end of each tendon. Mark the length of the femoral tunnel on the graft by measuring from the tip of the lever arm (Fig. 33-8). Pull the passing pin proximally until the lever arm enters the notch, and confirm that the lever arm is still facing laterally. Pull the passing pin until the mark of the graft enters the femoral tunnel. Cut the suture, remove the passing pin, and tension the suture, which deploys the lever arm. Pull on the distal end of the graft until the sudden, firm grip of the lever arm on cortical bone is felt. The lever arm rests laterally and in low profile on the anterolateral cortex of the femur (see Fig. 33-1).

EZLoc and the Skeletally Immature Patient
ACL reconstruction with a soft tissue graft is considered the treatment of choice in the skeletally immature patient to prevent uncorrectable injury to the menisci and articular cartilage.25 The EZLoc is designed to function without causing a growth plate arrest in the skeletally immature patient in contrast to the interference screw and cross-pin (Fig. 33-9). The EZLoc grips the femoral cortex several centimeters proximal to the growth plate. The body of the EZLoc is centered in the femoral tunnel and does not purchase bone on either side of the growth plate; therefore interference with growth is unlikely. In contrast to the EZLoc, the placement of an interference screw across the growth plate seems unwise, and oblique placement of the cross-pin has caused valgus angulation.26
EZLoc and Drilling through the Femoral Cortex
Drilling a 7- to 10-mm diameter tunnel through the lateral femoral cortex to pass the EZLoc produces a temporary stress riser that has not been reported to cause a femur fracture. Drilling through the lateral femoral cortex with a soft tissue graft and looping the graft around a fixation post outside the tunnel was the standard femoral fixation technique from the 1970s to early 1990s.27,28 During that time period, there were no published reports of femoral fracture around the drill hole. One reason that drilling the femoral tunnel across the femur did not cause a reportable femoral fracture is that the bone remodels along the length of the tunnel. Remodeling is especially rapid with the EZLoc because the titanium body encourages bone ingrowth that obliterates the tunnel within 4 to 6 months (Fig. 33-10).

Revision Surgery with the EZLoc
Because of the rapid growth of bone around the EZLoc, revision surgery may seem to be a challenge. Surprisingly, removal of the EZLoc is straightforward because the lever arm sits on the cortical bone and is easily located through a small anterolateral incision (Fig. 33-11). First, the distal end of the EZLoc should be freed by removing the remnant of the soft tissue ACL graft from the femoral tunnel with either a reamer on slow speed or a tissue ablation device. Next, a small curved gouge is used around the periphery of the proximal end to separate the ingrowth of cortical bone from the EZLoc. A small towel clip is used to grab the lever arm, and the EZLoc is pulled free of the tunnel. If the femoral tunnel was positioned correctly, and because we believe there is no tunnel widening with the EZLoc, the same tunnel and a new EZLoc can then be used to place and fix the revision ACL graft.
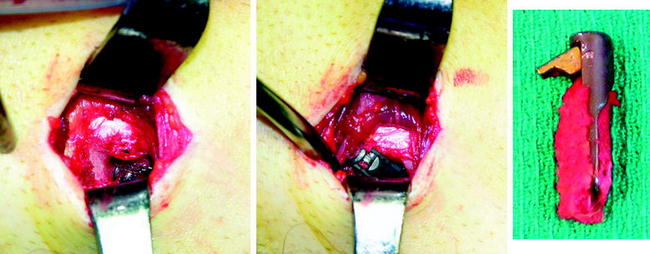
Fig. 33-11 Removal of the EZLoc is straightforward because the lever arm, which seats on the cortex of the anterolateral femur, is easily palpated through a small skin incision (left). The cortical bone that has grown in and around the proximal end of the EZLoc is freed with a small curved gouge. A small towel clip is used to grab the lever arm, and the EZLoc is removed (center).27,28 Dense bone has grown into the titanium EZLoc (right).
Conclusion
The EZLoc is a femoral fixation device for soft tissue ACL reconstruction that is simple and reliable for both the high-volume and occasional ACL surgeon and surgical team. The EZLoc combines superior fixation properties (1427N strength, 8 N/mm stiffness, and high resistance to slippage) and allows circumferential healing of the tendon graft to the tunnel wall, which allows aggressive rehabilitation without a brace and return to sport at 4 months.19,27,29 The EZLoc works well in patients with hard and soft bone and in the skeletally immature knee. Revision is straightforward, although a small anterolateral incision is required to identify and remove the EZLoc.
1 Brown CHJr, Wilson DR, Hecker AT, et al. Graft-bone motion and tensile properties of hamstring and patellar tendon anterior cruciate ligament femoral graft fixation under cyclic loading. Arthroscopy. 2004;20:922-935.
2 Kousa P, Jarvinen TL, Vihavainen M, et al. The fixation strength of six hamstring tendon graft fixation devices in anterior cruciate ligament reconstruction. Part I: femoral site. Am J Sports Med. 2003;31:174-181.
3 Kudo T, Tohyama H, Minami A, et al. The effect of cyclic loading on the biomechanical characteristics of the femur-graft-tibia complex after anterior cruciate ligament reconstruction using Bone Mulch screw/WasherLoc fixation. Clin Biomech (Bristol, Avon). 2005;20:414-420.
4 To JT, Howell SM, Hull ML. Contributions of femoral fixation methods to the stiffness of anterior cruciate ligament replacements at implantation. Arthroscopy. 1999;15:379-387.
5 Pujol N, David T, Bauer T, et al. Transverse femoral fixation in anterior cruciate ligament (ACL) reconstruction with hamstrings grafts: an anatomic study about the relationships between the transcondylar device and the posterolateral structures of the knee. Knee Surg Sports Traumatol Arthrosc. 2006;14:724-729.
6 Pelfort X, Monllau JC, Puig L, et al. Iliotibial band friction syndrome after anterior cruciate ligament reconstruction using the transfix device: report of two cases and review of the literature. Knee Surg Sports Traumatol Arthrosc. 2006;14:586-589.
7 Amis AA. The strength of artificial ligament anchorages. A comparative experimental study. J Bone Joint Surg. 1988;70B:397-403.
8 Greis PE, Burks RT, Bachus K, et al. The influence of tendon length and fit on the strength of a tendon-bone tunnel complex. A biomechanical and histologic study in the dog. Am J Sports Med. 2001;29:493-497.
9 Singhatat W, Lawhorn KW, Howell SM, et al. How four weeks of implantation affect the strength and stiffness of a tendon graft in a bone tunnel: a study of two fixation devices in an extraarticular model in ovine. Am J Sports Med. 2002;30:506-513.
10 Zacharias I, Howell SM, Hull ML, et al. In vivo calibration of a femoral fixation device transducer for measuring anterior cruciate ligament graft tension: a study in an ovine model. J Biomech Eng. 2001;123:355-361.
11 Grover DM, Howell SM, Hull ML. Early tension loss in an anterior cruciate ligament graft. A cadaver study of four tibial fixation devices. J Bone Joint Surg. 2005;87A:381-390.
12 Karchin A, Hull ML, Howell SM. Initial tension and anterior load-displacement behavior of high-stiffness anterior cruciate ligament graft constructs. J Bone Joint Surg. 2004;86A:1675-1683.
13 Magen HE, Howell SM, Hull ML. Structural properties of six tibial fixation methods for anterior cruciate ligament soft tissue grafts. Am J Sports Med. 1999;27:35-43.
14 Tomita F, Yasuda K, Mikami S, et al. Comparisons of intraosseous graft healing between the doubled flexor tendon graft and the bone-patellar tendon-bone graft in anterior cruciate ligament reconstruction. Arthroscopy. 2001;17:461-476.
15 Becker R, Voigt D, Starke C, et al. Biomechanical properties of quadruple tendon and patellar tendon femoral fixation techniques. Knee Surg Sports Traumatol Arthrosc. 2001;9:337-342.
16 Eagar P, Hull ML, Howell SM. How the fixation method stiffness and initial tension affect anterior load-displacement of the knee and tension in anterior cruciate ligament grafts: a study in cadaveric knees using a double-loop hamstrings graft. J Orthop Res. 2004;22:613-624.
17 Roos PJ, Hull ML, Howell SM. Lengthening of double-looped tendon graft constructs in three regions after cyclic loading: a study using Roentgen stereophotogrammetric analysis. J Orthop Res. 2004;22:839-846.
18 Matsumoto A, Howell SM. WasherLoc and bone dowel: a rigid slippage-resistant tibial fixation device for a soft tissue anterior cruciate ligament graft. Tech Orthop. 2005;20:278-282.
19 Howell SM, Deutsch ML. Comparison of endoscopic and two-incision techniques for reconstructing a torn anterior cruciate ligament using hamstring tendons. Arthroscopy. 1999;15:594-606.
20 Simmons R, Howell SM, Hull ML. Effect of the angle of the femoral and tibial tunnels in the coronal plane and incremental excision of the posterior cruciate ligament on tension of an anterior cruciate ligament graft: an in vitro study. J Bone Joint Surg. 2003;85A:1018-1029.
21 Cuomo P, Edwards A, Giron F, et al. Validation of the 65 degrees Howell guide for anterior cruciate ligament reconstruction. Arthroscopy. 2006;22:70-75.
22 Howell SM, Barad SJ. Knee extension and its relationship to the slope of the intercondylar roof. Implications for positioning the tibial tunnel in anterior cruciate ligament reconstructions. Am J Sports Med. 1995;23:288-294.
23 Howell SM, Clark JA, Farley TE. A rationale for predicting anterior cruciate graft impingement by the intercondylar roof. A magnetic resonance imaging study. Am J Sports Med. 1991;19:276-282.
24 Howell SM, Lawhorn KW. Gravity reduces the tibia when using a tibial guide that targets the intercondylar roof. Am J Sports Med. 2004;32:1702-1710.
25 Aichroth PM, Patel DV, Zorrilla P. The natural history and treatment of rupture of the anterior cruciate ligament in children and adolescents. A prospective review. J Bone Joint Surg. 2002;84B:38-41.
26 Koman JD, Sanders JO. Valgus deformity after reconstruction of the anterior cruciate ligament in a skeletally immature patient. A case report. J Bone Joint Surg. 1999;81:711-715.
27 Howell SM, Taylor MA. Brace-free rehabilitation, with early return to activity, for knees reconstructed with a double-looped semitendinosus and gracilis graft. J Bone Joint Surg. 1996;78A:814-825.
28 Howell SM, Taylor MA. Failure of reconstruction of the anterior cruciate ligament due to impingement by the intercondylar roof. J Bone Joint Surg Am. 1993;75A:1044-1055.
29 Aglietti P, Giron F, Buzzi R, et al. Anterior cruciate ligament reconstruction: bone-patellar tendon-bone compared with double semitendinosus and gracilis tendon grafts. A prospective, randomized clinical trial. J Bone Joint Surg. 2004;86A:2143-2155.






