[level-membership-for-radiology-category] GI tract, lungs, heart, kidneys, and nervous system
















 with a distal esophageal stricture
with a distal esophageal stricture  . Esophageal peristalsis was completely absent.
. Esophageal peristalsis was completely absent.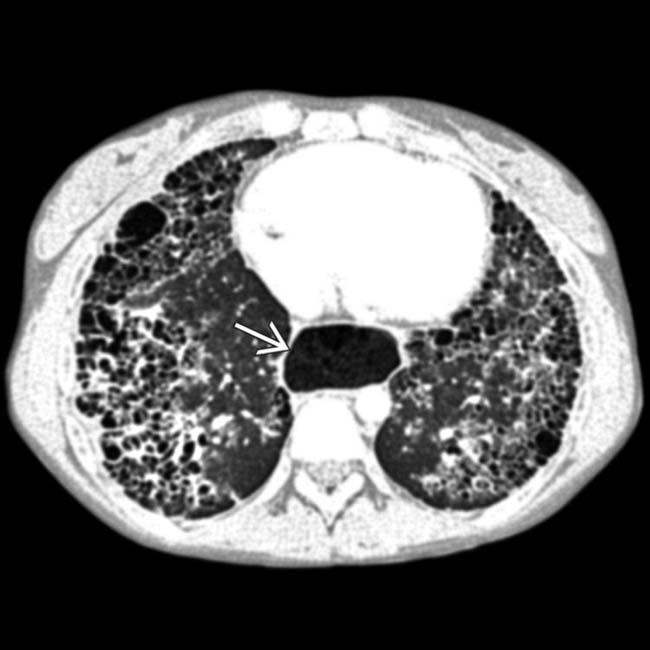
 , all findings due to scleroderma.
, all findings due to scleroderma.
 .
.
IMAGING
General Features




















































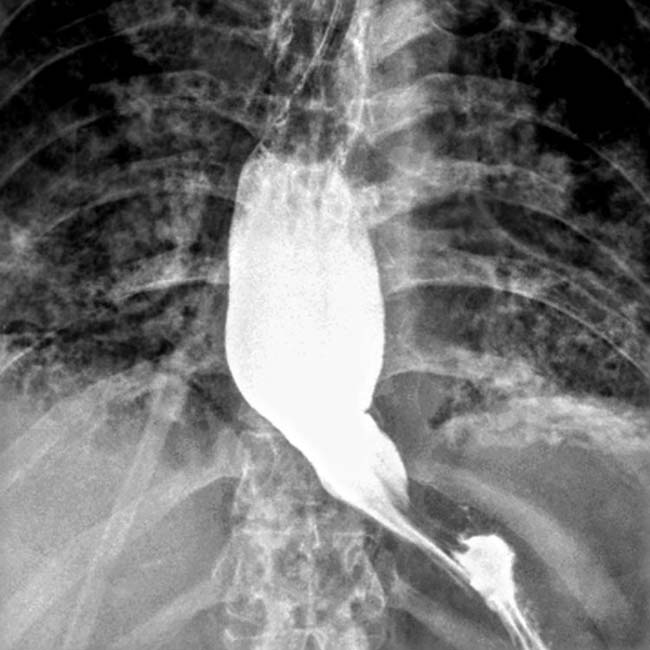
 . The esophageal lumen is mildly dilated, and there is a stricture at the GE junction
. The esophageal lumen is mildly dilated, and there is a stricture at the GE junction  .
.
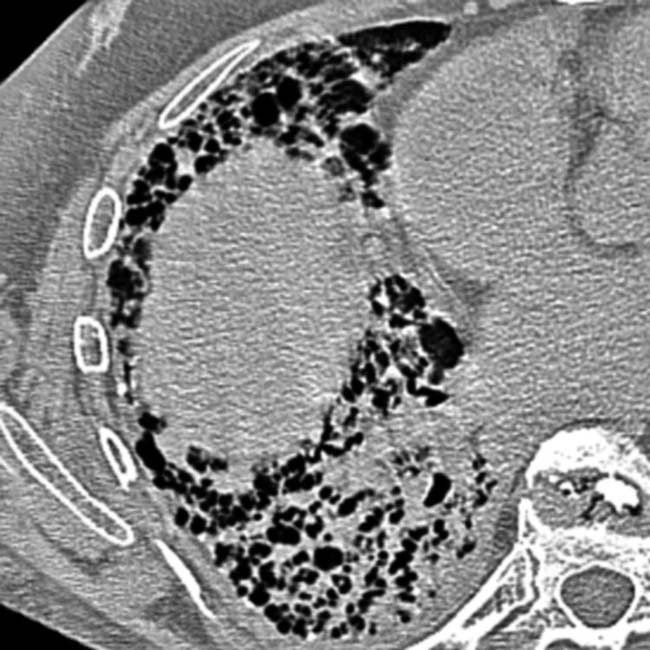
 , and the lumen is dilated with minimal peristalsis in this classic “hidebound” bowel.
, and the lumen is dilated with minimal peristalsis in this classic “hidebound” bowel.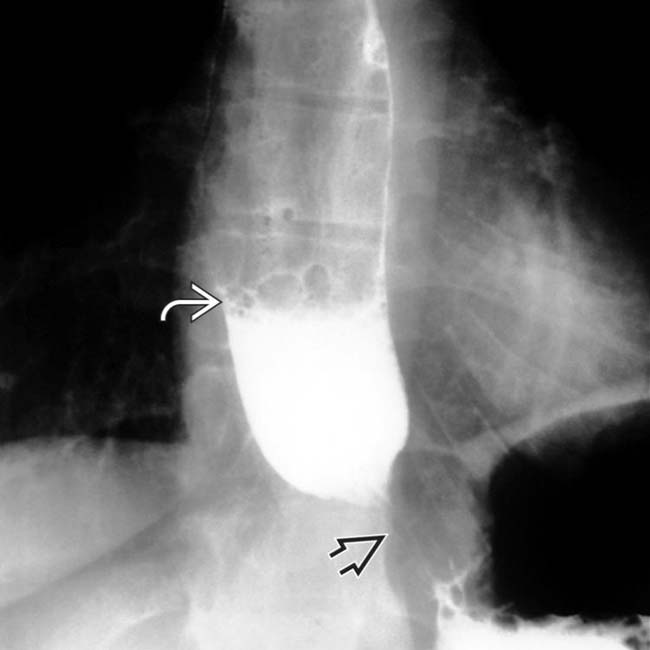
 at the GE junction. The esophagus was slow to empty, even in the upright position, with a fluid-barium level seen
at the GE junction. The esophagus was slow to empty, even in the upright position, with a fluid-barium level seen  .
.
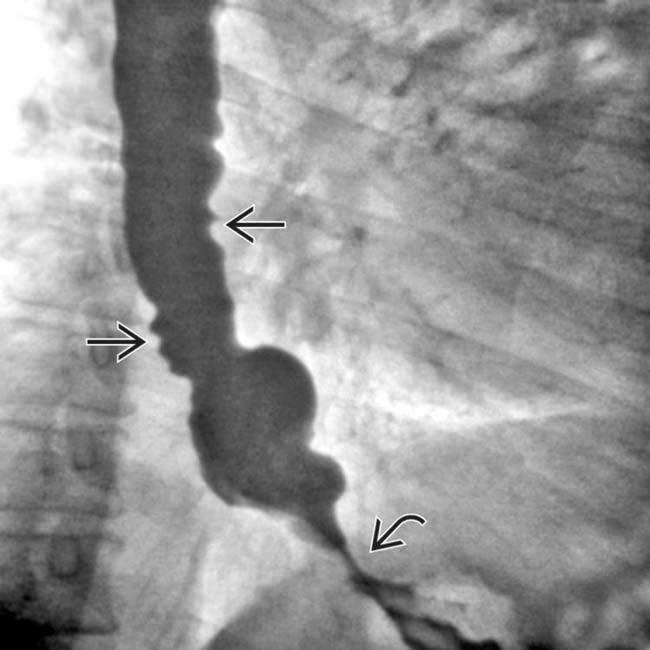
 , with abrupt narrowing as it crosses the spine. The duodenum is the most frequently affected part of the GI tract beyond the esophagus.
, with abrupt narrowing as it crosses the spine. The duodenum is the most frequently affected part of the GI tract beyond the esophagus.
 . The esophagus had no primary peristalsis. These are relatively early signs of scleroderma, and no stricture or ulcerations have yet developed.
. The esophagus had no primary peristalsis. These are relatively early signs of scleroderma, and no stricture or ulcerations have yet developed.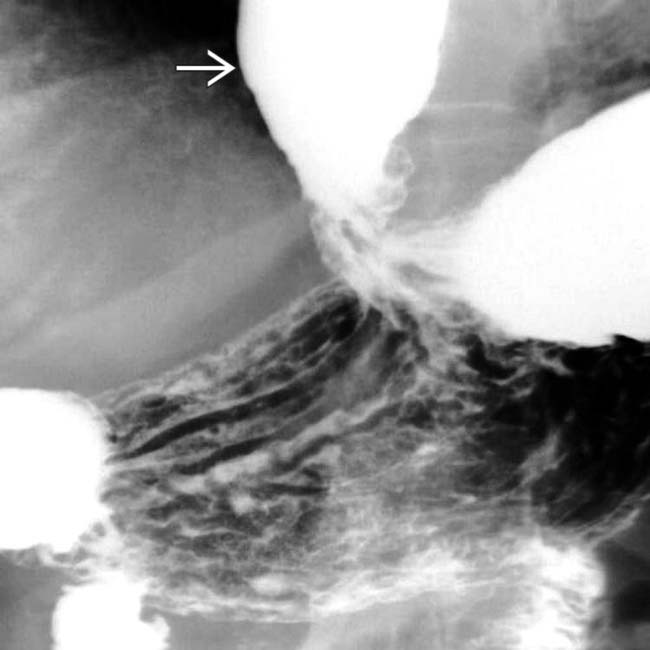
 .
.





[/level-membership-for-radiology-category][not-level-membership-for-radiology-category] GI tract, lungs, heart, kidneys, and nervous system
with a distal esophageal stricture . Esophageal peristalsis was completely absent., all findings due to scleroderma..IMAGING
General Features
Radiographic Findings
•
Buy Membership for Radiology Category to continue reading. Learn more here
[/not-level-membership-for-radiology-category]
