[level-membership-for-radiology-category] Majority are due to esophageal instrumentation
Confirmed by contrast esophagram or CT, which are complementary
• Cervical esophageal perforation (EP)
Subcutaneous or interstitial emphysema; neck and mediastinum
Consider perforation of Zenker diverticulum
• Thoracic EP
Chest film: Pneumomediastinum, pleural effusion
• EP of intraabdominal segment of distal esophagus
Abdominal plain film: Pneumoperitoneum
• EP near GE junction
Extravasated contrast from left lateral aspect of distal esophagus into mediastinum, sometimes pleural space, and rarely abdomen (never abdomen alone)
• CT shows extraesophageal air in almost all cases, fluid and contrast medium in most
• Intramural EP: Extravasated gas and contrast remain within esophageal wall
Much better prognosis
• Esophagography: Technique
Esophagram: Videofluoroscopic and rapid sequence filming
Nonionic water-soluble contrast media (e.g., Omnipaque) initially, followed with barium if no leak or fistula seen
Barium (or CT) may detect small leak not visible initially
TOP DIFFERENTIAL DIAGNOSES
• Esophageal diverticulum
• Esophageal ulceration
• Boerhaave syndrome
• Postoperative state, esophagus
• Tracheobronchial aspiration
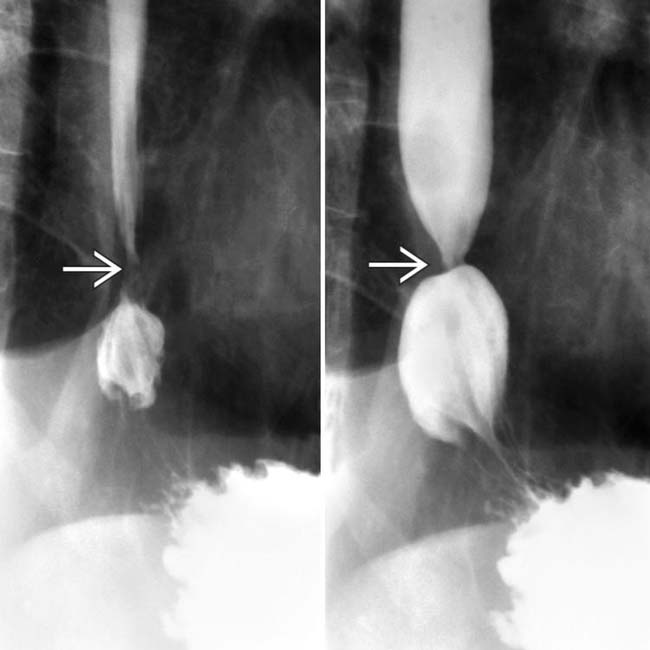
(Left) Barium esophagrams reveal a tight stricture at the gastroesophageal (GE) junction . Due to concern for Barrett metaplasia or early cancer, an endoscopic biopsy of the lesion was performed following balloon dilation of the stricture.
(Right) Postbiopsy esophagram in the same patient illustrates a focal intramural barium collection , indicating a localized perforation. These intramural perforations will usually heal spontaneously.
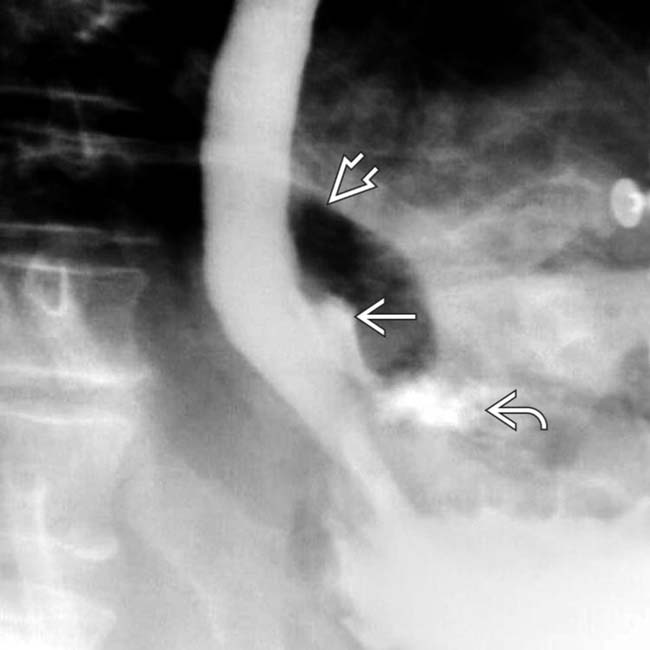
(Left) Esophagram in a 62-year-old man with a history of laparoscopic hiatal hernia repair, now presenting with subsequent chest pain and fever, demonstrates mediastinal and abdominal extraluminal collections of gas and contrast material.
(Right) Axial CECT in the same patient reveals mediastinal and abdominal extraluminal collections of gas and contrast material, indicating perforation near the GE junction. Surgical drainage was successful.
TERMINOLOGY
Abbreviations
• Esophageal perforation (EP)
Synonyms
• Esophageal rupture or transection
Definitions
• Transmural esophageal tear
IMAGING
General Features
• Best diagnostic clue
Diagnosis depends on high degree of suspicion and recognition of clinical features
– Confirmed by contrast esophagram or CT
• Location
Cervical EP: Posterior wall of esophagus at level of cricopharyngeus muscle
– Or through Zenker diverticulum
Thoracic EP: At or near gastroesophageal (GE) junction
– Areas of anatomic narrowing, sites of extrinsic compression by aortic arch or L main bronchus
At or above benign or malignant strictures
Site of ruptured anastomosis or after esophageal surgery
Radiographic Findings
• Radiography
Cervical EP: Anteroposterior, lateral films of neck
Rarely, thoracic EP heals spontaneously without surgical intervention
– Especially if intramural or very localized
• Surgical
Cervical esophageal perforation (EP): Cervical mediastinotomy, open drainage
Thoracic EP: Immediate thoracotomy, primary closure of EP, mediastinal drainage
• Covered metallic stents for leaks and fistulas
Growing in use
May still require drain placement in mediastinum ± pleural space
• Nonsurgical interventional drainage techniques; transesophageal drainage of abscesses
DIAGNOSTIC CHECKLIST
Consider
• Clinical and radiographic signs of EP may be subtle
Active investigation is needed to establish diagnosis
Image Interpretation Pearls
• Esophagram: Rapid sequence filming in multiple obliquities
• Esophagography and CT are complementary; either can “miss” perforation
(Left) Esophagram in a 54-year-old man with esophageal cancer and chest pain following endoscopic biopsy demonstrates a long, irregular, eccentric stricture of the distal esophagus , characteristic of carcinoma. Focal extravasation of contrast indicates perforation.
(Right) Film from an esophagram in a 67-year-old man with chest pain following repair of an epiphrenic diverticulum shows a persistent, linear, focal collection of contrast medium , representing a small leak. This healed with antibiotic therapy alone.
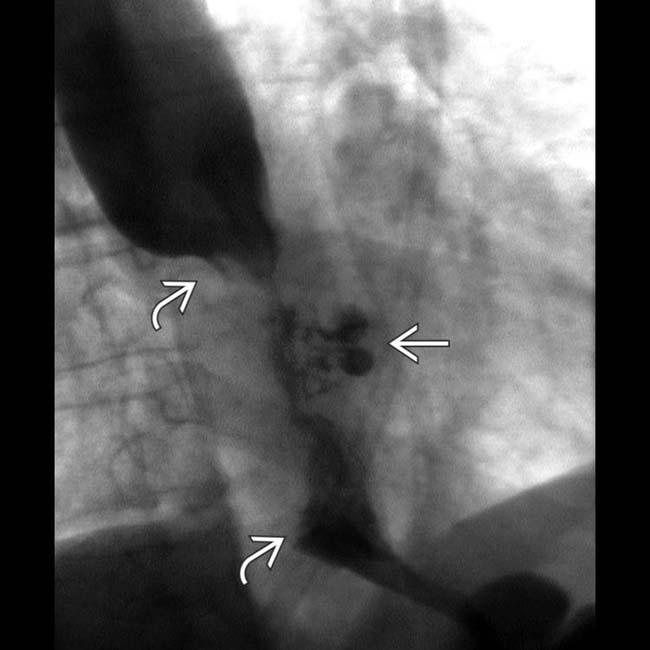
(Left) Esophagram film in a patient with neck and chest pain following attempted placement of a feeding tube shows a retroesophageal (mediastinal) collection of gas and water-soluble contrast medium . This resulted from perforation of a Zenker diverticulum by the feeding tube. The track runs posterior and parallel to the course of the proximal esophagus.
(Right) Axial NECT in the same patient shows subcutaneous gas , extraluminal gas, and contrast medium in the prevertebral region .
(Left) Esophagram in a 58-year-old man with chest pain following endoscopic removal of an impacted food bolus shows perforation of the distal esophagus with extravasation of contrast material and gas into the upper abdomen and mediastinum and free air under the diaphragm.
(Right) Axial NECT in the same patient shows free intraperitoneal gas and extraluminal gas along the esophagus and proximal stomach . The imaging findings are identical to those seen in Boerhaave syndrome.
Axial NECT shows extraluminal oral contrast medium in the upper abdomen following placement of a nasogastric tube that perforated the esophagogastric junction.
Esophagram shows a left mediastinal collection of contrast medium following balloon dilatation for achalasia.
Esophagram shows a contained leak following balloon dilatation of an esophageal stricture.
[/level-membership-for-radiology-category][not-level-membership-for-radiology-category] Majority are due to esophageal instrumentation
Confirmed by contrast esophagram or CT, which are complementary
• Cervical esophageal perforation (EP)
Subcutaneous or interstitial emphysema; neck and mediastinum
Consider perforation of Zenker diverticulum
• Thoracic EP
Chest film: Pneumomediastinum, pleural effusion
• EP of intraabdominal segment of distal esophagus
Abdominal plain film: Pneumoperitoneum
• EP near GE junction
Extravasated contrast from left lateral aspect of distal esophagus into mediastinum, sometimes pleural space, and rarely abdomen (never abdomen alone)
• CT shows extraesophageal air in almost all cases, fluid and contrast medium in most
• Intramural EP: Extravasated gas and contrast remain within esophageal wall
Much better prognosis
• Esophagography: Technique
Esophagram: Videofluoroscopic and rapid sequence filming
Nonionic water-soluble contrast media (e.g., Omnipaque) initially, followed with barium if no leak or fistula seen
Barium (or CT) may detect small leak not visible initially
TOP DIFFERENTIAL DIAGNOSES
• Esophageal diverticulum
• Esophageal ulceration
• Boerhaave syndrome
• Postoperative state, esophagus
• Tracheobronchial aspiration
(Left) Barium esophagrams reveal a tight stricture at the gastroesophageal (GE) junction . Due to concern for Barrett metaplasia or early cancer, an endoscopic biopsy of the lesion was performed following balloon dilation of the stricture.
(Right) Postbiopsy esophagram in the same patient illustrates a focal intramural barium collection , indicating a localized perforation. These intramural perforations will usually heal spontaneously.
(Left) Esophagram in a 62-year-old man with a history of laparoscopic hiatal hernia repair, now presenting with subsequent chest pain and fever, demonstrates mediastinal and abdominal extraluminal collections of gas and contrast material.
(Right) Axial CECT in the same patient reveals mediastinal and abdominal extraluminal collections of gas and contrast material, indicating perforation near the GE junction. Surgical drainage was successful.
TERMINOLOGY
Abbreviations
• Esophageal perforation (EP)
Synonyms
• Esophageal rupture or transection
Definitions
• Transmural esophageal tear
IMAGING
General Features
• Best diagnostic clue
Diagnosis depends on high degree of suspicion and recognition of clinical features
– Confirmed by contrast esophagram or CT
• Location
Cervical EP: Posterior wall of esophagus at level of cricopharyngeus muscle
– Or through Zenker diverticulum
Thoracic EP: At or near gastroesophageal (GE) junction
– Areas of anatomic narrowing, sites of extrinsic compression by aortic arch or L main bronchus
At or above benign or malignant strictures
Site of ruptured anastomosis or after esophageal surgery
Radiographic Findings
• Radiography
Cervical EP: Anteroposterior, lateral films of neck










 . Due to concern for Barrett metaplasia or early cancer, an endoscopic biopsy of the lesion was performed following balloon dilation of the stricture.
. Due to concern for Barrett metaplasia or early cancer, an endoscopic biopsy of the lesion was performed following balloon dilation of the stricture.
 , indicating a localized perforation. These intramural perforations will usually heal spontaneously.
, indicating a localized perforation. These intramural perforations will usually heal spontaneously.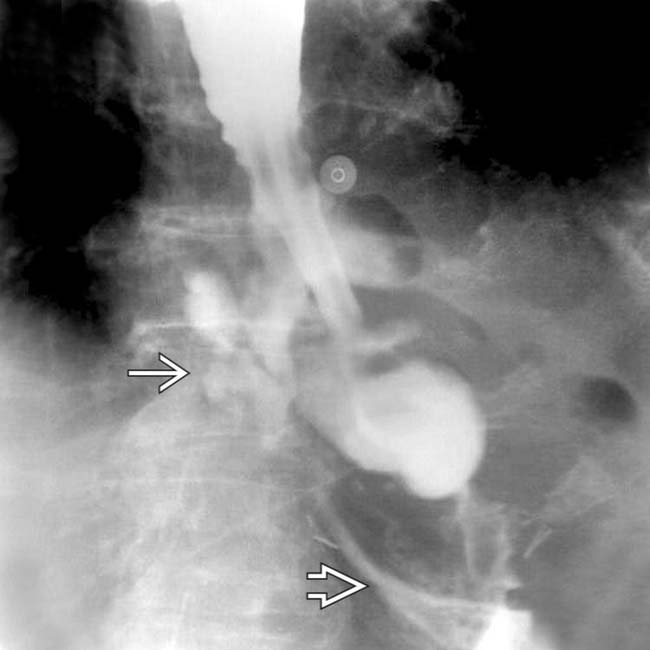
 and abdominal
and abdominal  extraluminal collections of gas and contrast material.
extraluminal collections of gas and contrast material.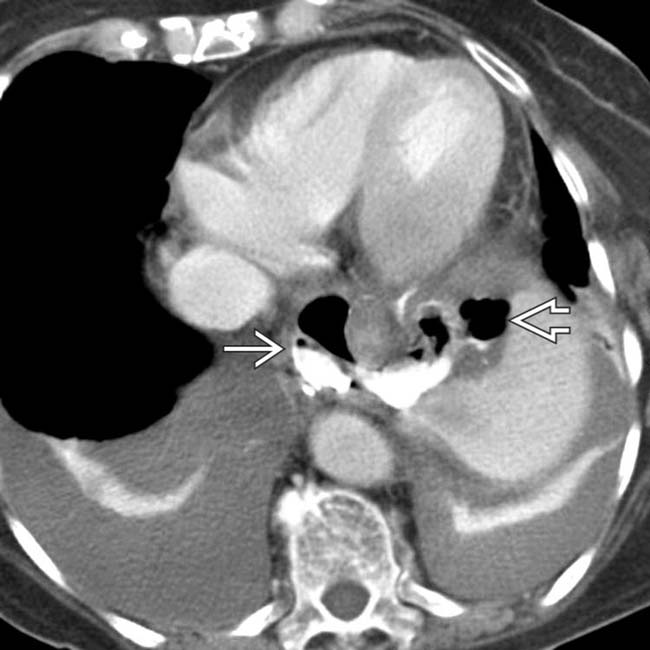
 and abdominal
and abdominal  extraluminal collections of gas and contrast material, indicating perforation near the GE junction. Surgical drainage was successful.
extraluminal collections of gas and contrast material, indicating perforation near the GE junction. Surgical drainage was successful.










































 , characteristic of carcinoma. Focal extravasation of contrast
, characteristic of carcinoma. Focal extravasation of contrast  indicates perforation.
indicates perforation.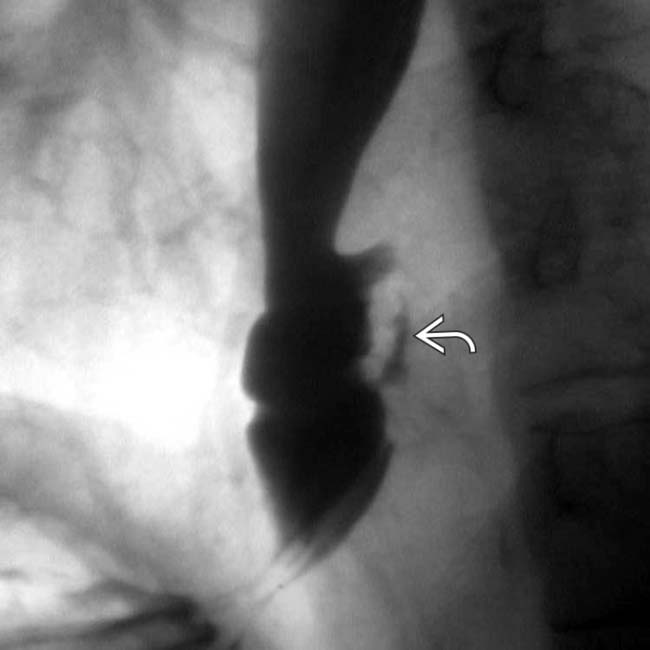
 , representing a small leak. This healed with antibiotic therapy alone.
, representing a small leak. This healed with antibiotic therapy alone.
 . This resulted from perforation of a Zenker diverticulum by the feeding tube. The track
. This resulted from perforation of a Zenker diverticulum by the feeding tube. The track  runs posterior and parallel to the course of the proximal esophagus.
runs posterior and parallel to the course of the proximal esophagus.
 , extraluminal gas, and contrast medium in the prevertebral region
, extraluminal gas, and contrast medium in the prevertebral region  .
.
 with extravasation of contrast material and gas
with extravasation of contrast material and gas  into the upper abdomen and mediastinum and free air
into the upper abdomen and mediastinum and free air  under the diaphragm.
under the diaphragm.
 and extraluminal gas along the esophagus and proximal stomach
and extraluminal gas along the esophagus and proximal stomach  . The imaging findings are identical to those seen in Boerhaave syndrome.
. The imaging findings are identical to those seen in Boerhaave syndrome.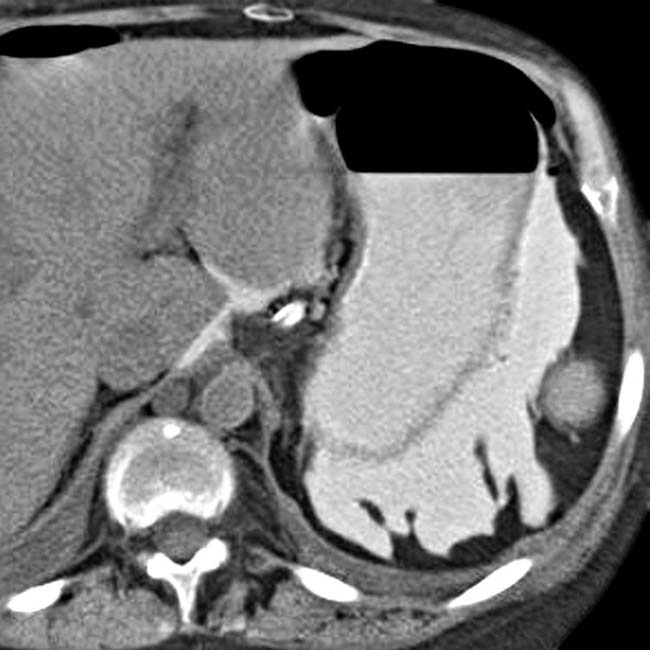

 following balloon dilatation for achalasia.
following balloon dilatation for achalasia.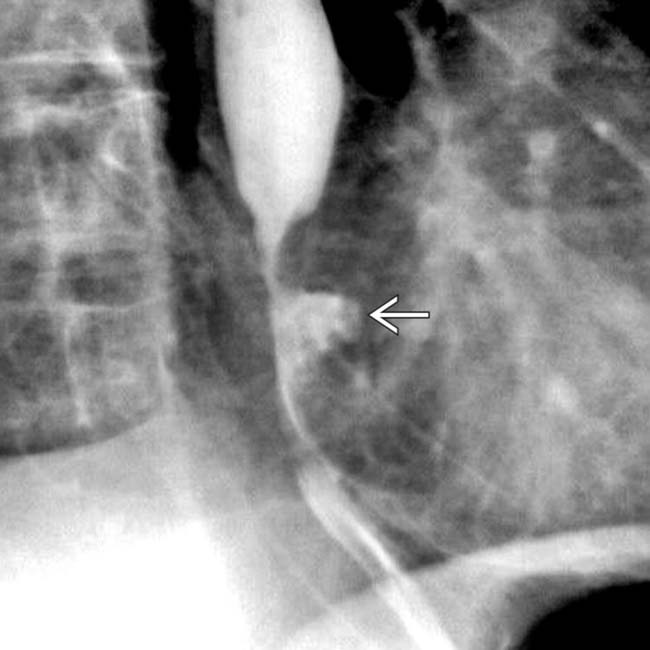
 following balloon dilatation of an esophageal stricture.
following balloon dilatation of an esophageal stricture.
