Individual bullae may resolve or progress to ulceration or stenosis
Oral mucosa involved in all patients, conjunctiva in most patients
• Treatment: Endoscopic dilation may be tried but it may lead to worse strictures
• Colonic interposition: To bypass refractory esophageal lesions
(Left) Oblique esophagram in a 19-year-old man with epidermolysis bullosa shows a tight, long stricture of the proximal esophagus. The proximal end of the stricture is fairly abrupt, while the distal end is more tapered.
(Right) Oblique esophagram in the same patient after attempted dilation shows that the stricture remains , now with extravasation of the contrast material , indicating perforation. The contrast material extends along the esophageal wall within the mediastinum.
(Left) Spot film from an esophagram in a 30-year-old woman with severe epidermolysis bullosa demonstrates a long stricture of the distal esophagus. Other films demonstrated more proximal strictures. These were treated with balloon dilation but have recurred.
(Right) Lateral esophagram in an 18-year-old man shows a web-like stricture near the pharyngoesophageal junction that is the result of repeated episodes of mucosal ulceration, typical of patients with epidermolysis bullosa.










 of the proximal esophagus. The proximal end of the stricture is fairly abrupt, while the distal end is more tapered.
of the proximal esophagus. The proximal end of the stricture is fairly abrupt, while the distal end is more tapered.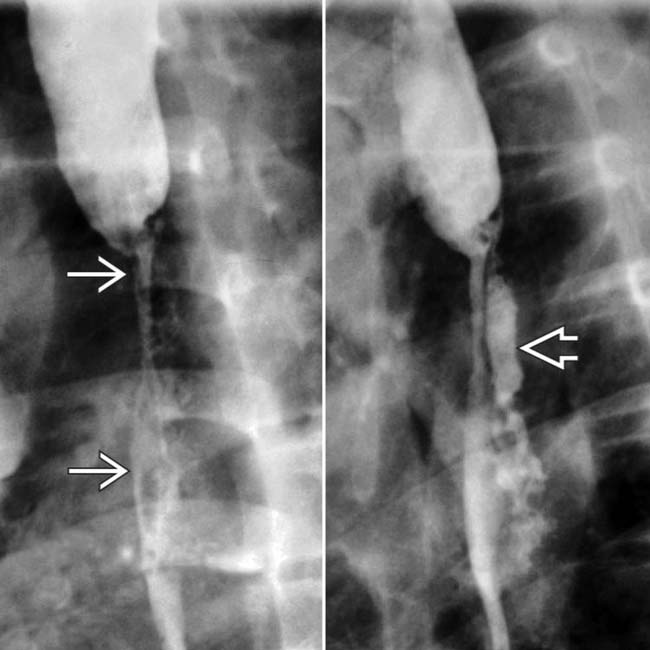
 , now with extravasation of the contrast material
, now with extravasation of the contrast material  , indicating perforation. The contrast material extends along the esophageal wall within the mediastinum.
, indicating perforation. The contrast material extends along the esophageal wall within the mediastinum.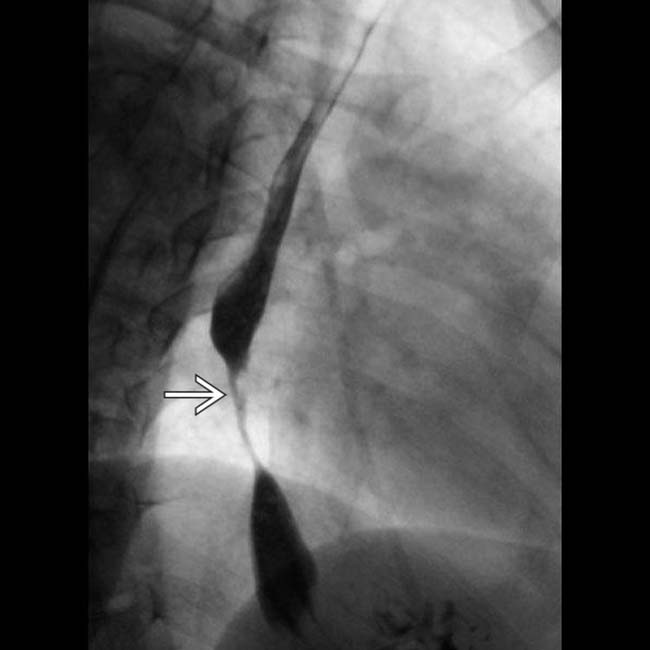
 of the distal esophagus. Other films demonstrated more proximal strictures. These were treated with balloon dilation but have recurred.
of the distal esophagus. Other films demonstrated more proximal strictures. These were treated with balloon dilation but have recurred.
 near the pharyngoesophageal junction that is the result of repeated episodes of mucosal ulceration, typical of patients with epidermolysis bullosa.
near the pharyngoesophageal junction that is the result of repeated episodes of mucosal ulceration, typical of patients with epidermolysis bullosa.


