CHAPTER 56 Epidemiology of Disc, Joint, and Root Pain in Whiplash
INTRODUCTION
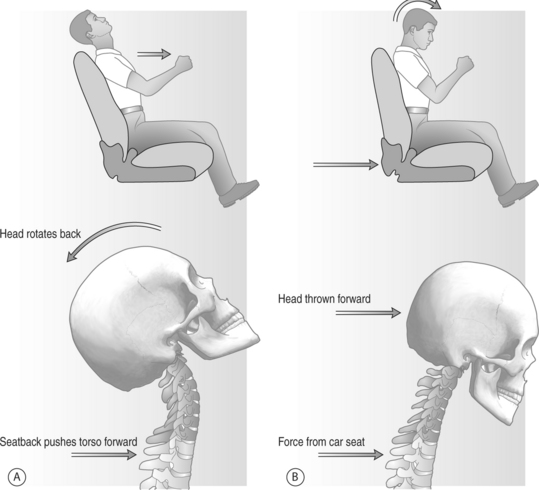
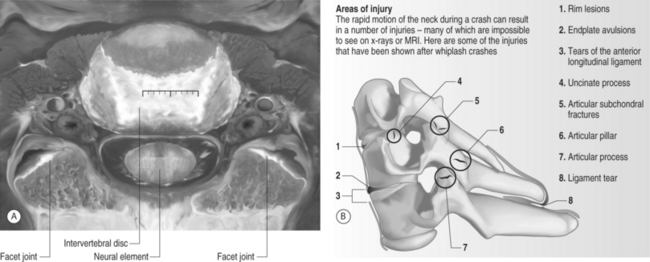
Neck pain resulting from a whiplash mechanism of injury is controversial and has attracted particular attention. A whiplash injury is typically defined as an injury to the cervical spine resulting from hyperextension and flexion of the head during a motor vehicle accident (Fig. 56.1). Sources of pain in whiplash patients are usually multifactorial. The primary affected anatomical structures of the cervical spine are perivertebral soft tissues, neuro-elements, intervertebral disc, and zygapophyseal joint (Fig. 56.2). Most whiplash-related neck pain is usually self-limiting, and can be adequately treated with conservative measures such as rest, nonsteroidal antiinflammatory agents, pain medications, muscle relaxants, and physical therapy. Patients failing to improve with this regimen may require further radiographic and interventional diagnostic work-ups.
Although epidemiology in whiplash has been relatively well studied, few studies have adequately provided detailed analyses of the anatomical structures involved in chronic neck pain in whiplash patients. Increased knowledge about the size and extent of this problem is essential as it may facilitate predictions of the need for medical services.1
EPIDEMIOLOGY OF WHIPLASH
Motor vehicle accidents with a whiplash mechanism of injury are one of the most common causes of neck injuries, with an incidence of perhaps 1 million per year in the United States.2 The social and economic costs are tremendous. Twenty-five to 30 billion dollars are spent annually on treatment for neck discomfort without neurologic signs in whiplash patients in the United States alone.3 The costs of whiplash injury are expected to rise with increasing incidence.
Whiplash injuries usually result in neck pain arising from injury to soft tissue, the disc, or zygapophyseal joint, and the etiology of this pain has been documented in animal and human studies. Headaches, reported in 82% of patients acutely, are usually of the muscle contraction type, and are often associated with greater occipital neuralgia related to C2 cervical nerve root injury, and less often to temporomandibular joint syndrome.4,5 Other frequent complaints include dizziness, paresthesia, postconcussion syndrome, and low back pain.6 Fifteen percent of whiplash patients suffer severe pain for 1–3 years, and 26–44% of patients will develop long-term problems.7 Chronic whiplash has long been a source of controversy, in large part because most patients do not have a readily identifiable injury in either the acute or chronic stage. Chronic unremitting pain occurs in 5% of patients.8
Incidence and prevalence
The incidence and severity of whiplash injury is increasing with the wider use of transport and the development of higher-velocity vehicles.9 Many epidemiologic studies have been reported from a number of countries utilizing automobile insurance company data. Considerable caution is necessary when comparing national statistics. Such statistics are dependent on complex social and legal variables, and cannot be used as an overall measure of incidence.10 The occurrence, severity, and duration of whiplash-related symptoms have been reported differently among different countries. Regional differences within the same country may also impact study results. Wide differences between countries in cultural attitude, insurance systems, or financial compensation may significantly impact statistical analyses. In an analysis of 300 cases showing lower whiplash incidence in Singapore relative to Australia,11 the author suggested that cultural differences in how whiplash was viewed in these two countries (e.g. as an illness, versus as an illness behavior) were a significant variable. A 1987 Quebec study showed increasing whiplash incidence.6 The overall incidence was 70 per 100 000 persons, but the rate in a Saskatchewan study was 700 per 100 000 persons. In this case, differences may be caused by regional variations in the insurance compensation system: a no-fault insurance system in Quebec versus a tort system in Saskatchewan.
Legislation changes in Australia (the claimant now has to report the accident to the police and bear the first $317 of medical expense), afforded a substantial effect upon whiplash incidence. One year following the new law, whiplash reported incidences were 50–70% fewer than previous years, even though there presumably may have been more vehicles on the road. A recent study also supported the idea that financial compensation by insurance systems has a profound effect on the frequency and duration of whiplash claims, and that claimants recover faster if compensation for pain and suffering is not available. Cassidy et al.14 studied a population-based cohort of persons who filed insurance claims for traffic injuries in Saskatchewan, where the insurance system was changed from the tort compensation system to a no-fault system. After the introduction of no-fault, there was a 28% reduction in incidence, and the median time to the closure of claims was reduced by more than 200 days.
Prognosis
Whiplash is associated with high costs and a prognosis that is variable and difficult to predict. A prospective study of 93 patients with cervical whiplash revealed that only 15% had persistent minor discomfort, but 43% of patients still had symptoms sufficiently severe to interfere with their ability to work 2 years after the injury.15
Many studies addressing prognostic factors have been published, but there have been various results. Hildingsson and Toolan15 found that acute symptoms, physical findings, forces and directions of impact, head rests, radiographs, and sex did not show prognostic value. However, Evans2 suggested that some risk factors, including older age, interscapular or upper back pain, occipital headache, paresthesia at presentation, reduced range of cervical spine movement, objective neurologic deficits, preexisting degenerative osteoarthritic changes, and an upper-middle occupational category correlated with less favorable recovery. These data showed long-term disability in over 6% of patients, and patients with those risk factors did not return to work after 1 year. There was, however, only minimal association between poor prognosis and collision speed or severity and the extent of vehicle damage.
In a recent study, risk factors for prolonged recovery time after whiplash injury were introduced.16 All vehicular-related injury reports and medical records of 4759 individuals, who sustained a whiplash injury in the province of Quebec, Canada, in 1987, were recruited, and the author followed these patients for up to 7 years. The author found that sociodemographic factors including older age, female sex, having dependants, and not being employed full-time each decreased the rate of recovery by 14–16%. Factors related to the crash conditions decreased the rate of recovery as follows: being in a truck or bus, 52%; being a passenger in the vehicle, 15%; colliding with a moving vehicle, 16%; and side or frontal collision, 15%. The median recovery time was 32 days, and 12% of subjects had still not recovered after 6 months. Signs and symptoms independently associated with slower recovery besides female gender and older age included neck pain on palpation, muscle pain, pain or numbness radiating from neck to arms, hands or shoulders, and headache. The presence of all these factors in females aged 60 predicted a median recovery time of 262 days, compared with 17 days for younger males aged without any of these factors. The author concluded that sociodemographic and crash-related factors, as well as several signs and symptoms, are predictive of a longer recovery period. An early intervention program was recommended to manage whiplash patients with these prognostic markers.
JOINT PAIN
The zygapophyseal joint has been considered as a possible source of whiplash patient pain (Fig. 56.3). Autopsy studies have shown structural spine damage, including joint injuries such as joint hemarthrosis, cartilage damage, and capsular ligament, in whiplash victims.17,18 Clinical studies have shown that cervical zygapophyseal joint pain is the most common etiology for chronic neck pain after whiplash, and the prevalence of specific cervical zygapophyseal joint involvement has also been reported. However, the studies have been limited, as this zygapophyseal joint-mediated pain was not diagnosed and confirmed using controlled diagnostic joint blocks.19–23
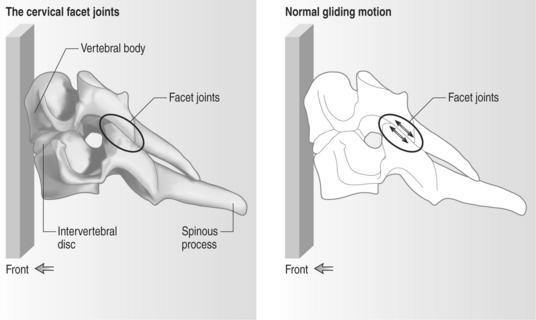
Fig. 56.3 The cervical facet joints.
(Adapted, with permission, from an original image by Michael Melton, www.injuryresources.com)
Barnsley et al.20 studied the prevalence of cervical zygapophyseal joint pain using double-blind, controlled, diagnostic blocks in 50 patients with a history of whiplash injury an average of 4 years prior to evaluation. During separate evaluations, the joint was randomly blocked with either lidocaine or bupivacaine. Fifty-four percent of patients experienced neck pain relief, suggesting that cervical zygapophyseal joint pain was the most common source of chronic neck pain after whiplash. However, this study was limited, as the injection protocol may be compromised by placebo responses. A subsequent double blind, placebo-controlled study by the same group supported the importance of zygapophyseal joint pain.22 Two different local anesthetics and a placebo injection of normal saline were administered in random order in 68 consecutive patients referred for chronic neck pain. A positive diagnosis was made if the patient’s pain was completely and reliably relieved by each local anesthetic, but not by the placebo injection. This study showed that the cervical facet joints were the source of neck pain in 60% of the population with chronic pain after whiplash injury. The prevalence of C2–3 zygapophyseal joint pain was 50%, and the prevalence of lower cervical zygapophyseal joint pain was 49%.
ROOT PAIN
During a whiplash injury, cervical nerve roots may be a secondary injury to disc protrusion or zygapophyseal joint trauma.24–26 The nerve roots are also susceptible to significant injury in the absence of more overt trauma to contiguous structures.25–27 During the extension phase of injury, the nerve root may become entrapped in a transiently narrowed neural foramen.25,26 Statistically significant reductions in the foramen diameter with increasing extension compared to the foraminal diameter at the neutral position have been observed.28 In addition, significant pressure increments have been related to head position. Farmer and Wisneski29 measured pressure in the neural foramina of C5, C6, and C7 nerve roots at various positions of the head and ipsilateral arm in eight fresh cadavers. Increasing neck extension led to significant pressure changes at each root tested, but the results with neck flexion were variable. The nerve initially compressed by neck extension may be subjected to a traction injury as the neck is thrown into a rebound flexion.25,26 This direct root trauma likely leads to intraneural vascular congestion and edema.25,26,30,31 Olmarker et al.30 studied edema formation in spinal nerve roots of the pig cauda equina following experimental compression at various rates, and found that edema formation was more pronounced after rapid onset of compression. They also found that intraneural edema may be more easily formed in nerve roots than peripheral nerves following compression injury.32
Few epidemiologic studies have evaluated root pain after whiplash. In 1953, Gay and Abbott25 reported that the most common complication after whiplash was cervical radiculopathy. In 50 patients who suffered from a whiplash injury to the neck for 4 years, 35 cases (70%) had intense pain in the posterior cervical region, with radiation of pain into the occipital region, shoulder girdle, or upper extremities. Pain was intermittent and often followed a pattern suggesting irritation of the fifth, sixth, or seventh cervical nerve root on one side. Eighteen cases (36%) had persistent cervical radiculopathic pain which was not improved by conservative treatment. Of these 18 cases, 13 had protruded intervertebral discs, and 5 had hypertrophic arthritis of the cervical spine confirmed by radiologic examination. All of these patients showed evidence of lower cervical root involvement. In a prospective outcome study, Jonsson et al.27 assessed the clinical and imaging findings of 50 patients (17 men, 33 women, mean age: 33 years) with whiplash-type neck distortions. Neck pain persisted in 24 patients (48%) and radiating pain developed within 6 weeks in 19 patients (38%). Eight patients with severe radiating pain and large disc protrusions on MRI had surgically confirmed fresh disc herniations.
One recent study evaluated the outcome of therapeutic selective nerve root blocks for whiplash-induced cervical radicular pain. Of 21 patients with diagnosis confirmed by diagnostic selective nerve root injection, 12 patients (57%) demonstrated involvement of a single root, 8 patients (38%) of two roots, and 1 patient (5%) of three roots. The most commonly involved nerve root was C7 (40.6%) followed by C8 (25%), C6 (21.9%), C5 (9.4%), and T1 (3.1%). Of these patients, only 36.4% were working full time, and 81.8% were taking medication including opiates (22.7%) and prescription NSAIDs (31.8%). However, clinical efficacy of selective nerve root block for radicular pain after whiplash was not demonstrated.33
DISC PAIN
Cervical discs have been suggested as one of the factors causing pain in both acute and late-phase whiplash. The most common site of disc injury is C5–6 in studies using radiographic evidence.27,34,35 This finding was supported by a recent kinematic analysis of cervical intervertebral discs during simulated whiplash.36 The authors suggested that whiplash trauma could potentially injure the cervical discs posteriorly via excessive 150° fiber strain and disc shear strain, or anteriorly via axial elongation. The 150° fiber and disc shear strains were the greatest at the posterior region of the C5–6 disc, consistent with previous reports that the vast majority of the disc injuries occurred at C5–6.
Intervertebral disc damage has been consistently documented in pathologic and clinical investigations of whiplash injury patients. In an autopsy study, Taylor and Twomey18 showed clefts in the cartilage plates of the intervertebral discs in 15 of 16 spines from whiplash victims. Posterior disc herniation through a damaged anulus fibrosus was also found, suggesting that common disc injuries could cause the pain experienced by whiplash patients. Jonsson et al.27 demonstrated a high incidence of discoligamentous injuries in whiplash-type distortion through a 5-year follow-up outcome study. Fresh disc herniation was surgically confirmed in 20% of whiplash patients with persistent, severe radiating pain. In another long-term follow-up study, Watkinson et al.37 reviewed 10 years of whiplash patient follow-up data, and found that radiographically documented degenerative changes of the cervical spine were present in 68% of patients, of whom 87% were symptomatic. The disc degeneration rate was higher in the whiplash patients when compared with age-matched controls.
In a retrospective study, Hamer et al.38 provided evidence that whiplash patients are at an increased risk of premature disc degeneration. The incidence of previous whiplash injury in 215 unselected patients who underwent an anterior cervical discectomy and fusion was twice that of a control population of 800 general orthopedic outpatients. Another retrospective MRI study documented disc herniations causing cord impingement and occult anterior vertebral endplate fractures in whiplash patients.34 A clinical study demonstrated that 39% of whiplash patients without initial radiographic signs of disc degeneration developed degenerative changes within 5–10 years. Although this study was not an age-matched, controlled study, the results may support the hypothesis that whiplash trauma can accelerate disc degeneration.39
Although a few studies have reported pathologic MRI findings after whiplash injuries, there is only one published prospective study. Pettersson et al.35 performed clinical examination and MRI in 39 whiplash patients (20 women and 19 men, mean age: 32 years) at a mean of 11 days after trauma, and repeated the procedure at a 2-year follow-up visit. Thirty-three percent of whiplash patients (13 patients) showed herniated cervical discs with medullary impingement (15.4%) or dura impingement (17.9%) at the 2-year follow-up. Patients with medullary impingement had persistent or increased symptoms. The most common involved levels were C4–6, which corroborates previous studies.27,34,40 The authors suggested that MRI is a reliable study for deciding the treatment plan of patients with persistent arm pain, neurologic deficits, or clinical signs of nerve root compression. However, performing MRI in acute phase was not recommended due to the relatively high proportion of false-positive findings, although disc pathology was clearly one contributing factor to the development of chronic symptoms following whiplash injury.
1 Guez M, Hildingsson C, Nilsson M, et al. The prevalence of neck pain: a population-based study from northern Sweden. Acta Orthop Scand. 2002;73:455-459.
2 Evans RW. Some observations on whiplash injuries. Neurol Clin. 1992;10:975-997.
3 Kwan O, Fiel J. Critical appraisal of facet joint injections for chronic whiplash. Med Sci Monit. 2002;8:RA191-RA195.
4 Keith WS. ‘Whiplash’-injury of the 2nd cervical ganglion and nerve. Can J Neurol Sci. 1986;13:133-137.
5 Packard RC. The relationship of neck injury and post-traumatic headache. Curr Pain Headache Rep. 2002;6:301-307.
6 Spitzer WO, Skovron ML, Salmi LR, et al. Scientific monograph of the Quebec Task Force on Whiplash-Associated Disorders: redefining ‘whiplash’ and its management. Spine. 1995;20:1S-73S.
7 Johnson G. Hyperextension soft tissue injuries of the cervical spine – a review. J Accid Emerg Med. 1996;13:3-8.
8 Macnab I. The ‘whiplash syndrome.’. Orthop Clin North Am. 1971;2:389-403.
9 Schutt CH, Dohan FC. Neck injury to women in auto accidents. A metropolitan plague. JAMA. 1968;206:2689-2692.
10 Mayou R, Radanov BP. Whiplash neck injury. J Psychosom Res. 1996;40:461-474.
11 Balla JI. The late whiplash syndrome: a study of an illness in Australia and Singapore. Cult Med Psychiatry. 1982;6:191-210.
12 Awerbuch MS. Whiplash in Australia: illness or injury? Med J Aust. 1992;157:193-196.
13 McDermott FT. Reduction in cervical ‘whiplash’ after new motor vehicle accident legislation in Victoria. Med J Aust. 1993;158:720-721.
14 Cassidy JD, Carroll LJ, Cote P, et al. Effect of eliminating compensation for pain and suffering on the outcome of insurance claims for whiplash injury. N Engl J Med. 2000;342:1179-1186.
15 Hildingsson C, Toolanen G. Outcome after soft-tissue injury of the cervical spine. A prospective study of 93 car-accident victims. Acta Orthop Scand. 1990;61:357-359.
16 Suissa S. Risk factors of poor prognosis after whiplash injury. Pain Res Manag. 2003;8:69-75.
17 Jonsson HJr, Bring G, Rauschning W, et al. Hidden cervical spine injuries in traffic accident victims with skull fractures. J Spinal Disord. 1991;4:251-263.
18 Taylor JR, Twomey LT. Acute injuries to cervical joints. An autopsy study of neck sprain. Spine. 1993;18:1115-1122.
19 Aprill C, Bogduk N. The prevalence of cervical zygapophyseal joint pain. A first approximation. Spine. 1992;17:744-747.
20 Barnsley L, Lord SM, Wallis BJ, et al. The prevalence of chronic cervical zygapophyseal joint pain after whiplash. Spine. 1995;20:20-25. discussion 26
21 Bogduk N, Marsland A. The cervical zygapophyseal joints as a source of neck pain. Spine. 1988;13:610-617.
22 Lord SM, Barnsley L, Wallis BJ, et al. Chronic cervical zygapophyseal joint pain after whiplash. A placebo-controlled prevalence study. Spine. 1996;21:1737-1744. discussion 1744–1745
23 Sapir DA, Gorup JM. Radiofrequency medial branch neurotomy in litigant and nonlitigant patients with cervical whiplash: a prospective study. Spine. 2001;26:E268-E273.
24 Borchgrevink GE, Smevik O, Nordby A, et al. MR imaging and radiography of patients with cervical hyperextension–flexion injuries after car accidents. Acta Radiol. 1995;36:425-428.
25 Gay JR, Abbott KH. Common whiplash injuries to the neck. JAMA. 1953;152:1698-1704.
26 Seletz E. Whiplash injuries: Neurophysiologic basis for pain and methods used for rehabilitation. JAMA. 1958;168:1750-1755.
27 Jonsson HJr, Cesarini K, Sahlstedt B, et al. Findings and outcome in whiplash-type neck distortions. Spine. 1994;19:2733-2743.
28 Yoo JU, Zou D, Edwards WT, et al. Effect of cervical spine motion on the neuroforaminal dimensions of human cervical spine. Spine. 1992;17:1131-1136.
29 Farmer JC, Wisneski RJ. Cervical spine nerve root compression. An analysis of neuroforaminal pressures with varying head and arm positions. Spine. 1994;19:1850-1855.
30 Olmarker K, Rydevik B, Holm S. Edema formation in spinal nerve roots induced by experimental, graded compression. An experimental study on the pig cauda equina with special reference to differences in effects between rapid and slow onset of compression. Spine. 1989;14:569-573.
31 Rydevik B, Brown MD, Lundborg G. Pathoanatomy and pathophysiology of nerve root compression. Spine. 1984;9:7-15.
32 Slipman CW, Lipetz JS, DePalma MJ, et al. Therapeutic selective nerve root block in the nonsurgical treatment of traumatically induced cervical spondylotic radicular pain. Am J Phys Med Rehabil. 2004;83:446-454.
33 Slipman CW, Lipetz JS, Jackson HB, et al. Outcome of therapeutic selective nerve root blocks for whiplash-induced cervical radicular pain. Pain Physician. 2001;4:167-174.
34 Davis SJ, Teresi LM, Bradley WGJr, et al. Cervical spine hyperextension injuries: MR findings. Radiology. 1991;180:245-251.
35 Pettersson K, Hildingsson C, Toolanen G, et al. Disc pathology after whiplash injury. A prospective magnetic resonance imaging and clinical investigation. Spine. 1997;22:283-287. discussion 288
36 Panjabi MM, Ito S, Pearson AM, et al. Injury mechanisms of the cervical intervertebral disc during simulated whiplash. Spine. 2004;29:1217-1225.
37 Watkinson A, Gargan MF, Bannister GC. Prognostic factors in soft tissue injuries of the cervical spine. Injury. 1991;22:307-309.
38 Hamer AJ, Gargan MF, Bannister GC, et al. Whiplash injury and surgically treated cervical disc disease. Injury. 1993;24:549-550.
39 Hohl M. Soft-tissue injuries of the neck in automobile accidents. Factors influencing prognosis. J Bone Joint Surg Am. 1974;56:1675-1682.
40 McKenzie JA, Williams JF. The dynamic behaviour of the head and cervical spine during ‘whiplash’. J Biomech. 1971;4:477-490.






