Enveloped DNA Viruses
• This family comprises large viruses with an enveloped, icosadeltahedral capsid and a linear, double-stranded DNA genome.
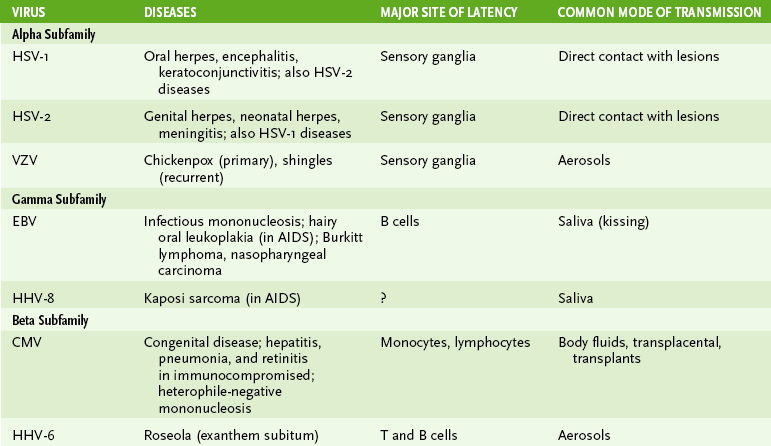
• All three subfamilies (alpha, beta, and gamma) contain significant human pathogens, which can establish primary lytic or persistent infection, as well as latent and recurrent infections (Table 22-1).
TABLE 22-1
A Herpes simplex viruses type 1 (HSV-1) and type 2 (HSV-2)
• Initial infection and viral replication occur in mucoepithelial cells.
• Characteristic HSV lesions associated with lytic infection are due to virus-induced cytopathic effects and inflammatory reactions.
• Latent infection, causing no detectable damage, is established in sensory ganglia (neurotropic) innervating the site of the initial lesion.
• Reactivation of latent HSV may be induced by emotional or physical stress, certain foods, or immune suppression.
a. Clinical manifestations of HSV infection depend on the tissue infected. Recurrent disease is less severe than primary infection and may be asymptomatic.
b. HSV-1 and HSV-2 cause disease at the site of infection and cause similar disease presentations.
• Classic HSV lesions are vesicular with an erythematous base.
• Oral herpes (herpes labialis and gingivostomatosis) is caused primarily by HSV-1 in children and also by HSV-2 in young adults.
• Genital herpes is most commonly caused by HSV-2.
• Encephalitis and keratoconjunctivitis are usually due to HSV-1.
• Disseminated infection and more severe disease occur in individuals with compromised cell-mediated immunity and in neonates.
• Characteristic cytopathic effects are observed in vesicle fluid, biopsy samples from affected tissue (Tzanck smear and Papanicolaou smear), or cultured infected cells.
• Immunoassays for type-specific viral antigens can detect and distinguish HSV-1 and HSV-2.
• Polymerase chain reaction detection of HSV nucleic acids in cerebrospinal fluid is used in diagnosis of encephalitis.
• Direct contact with vesicle fluid or virus-containing mucus (e.g., by kissing, sharing utensils, sexual contact, autoinoculation, and passage through birth canal) spreads HSV.
• HSV-1 is ubiquitous, and more than 90% of the population is infected in childhood.
• HSV-2 is usually transmitted sexually and acquired later in life by about 30% of the population.
B Varicella-zoster virus (VZV)
• Like HSV, VZV causes vesicular lesions and establishes latency in neurons.
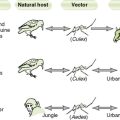
• VZV differs from HSV in its transmission (aerosols), usual site of entry (respiratory tract), and spread within the body (through lymphatics and the bloodstream).
• Primary VZV disease (Fig. 22-1)
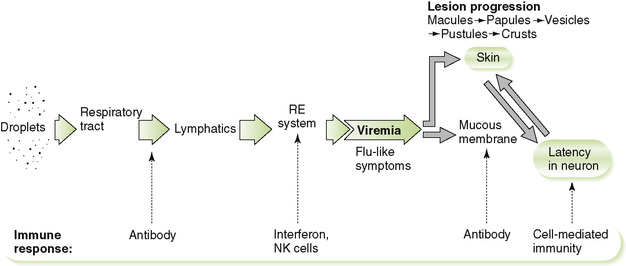
• Skin lesions first appear on the trunk, 10 to 14 days after exposure (maximum, 90 days), and then on the peripheral regions of the body, including the scalp.
a. Lesions progress from initial macule → papule → vesicle → pustule → crusts.
b. A thin-walled vesicle on a maculopapular base (dewdrop on a rose petal) is the hallmark of chickenpox.
• Chickenpox is generally benign and self-limited in otherwise healthy children, but it can be life threatening in immunocompromised children.
• Respiratory spread before the onset of symptoms is the primary mode of transmission of VZV.
• Shingles usually begins with severe pain along a single dermatome, followed by eruption of a belt of maculopapular lesions on an erythematous base.
• Thoracic and lumbar dermatomes are most commonly involved, but recurrence can occur along the trigeminal nerve or any dermatome.
• Diagnosis of VZV is generally made on the basis of clinical symptoms.
• Multinucleated giant cells and Cowdry type A nuclear inclusion bodies are present in VZV-infected cells from clinical specimens.
• Live attenuated varicella vaccine is recommended for children at 15 months and for nonimmune adults.
• Stronger varicella vaccine is recommended for adults at risk for zoster (>60 years of age)
• Antiviral drugs: acyclovir, famciclovir, or valacyclovir
• Varicella-zoster immunoglobulin is used for immunocompromised children who have been exposed.
• Infects B cells in the oropharynx (e.g., tonsils) after attaching to CD21 (C3d receptor)
a. Initial lytic infection of the B cells leads to shedding of virions into the saliva and surrounding lymphoid tissue.
• Nonproductive infection of B cells induces their proliferation with production of immunoglobulin M (IgM) heterophile antibodies
• Cell-mediated response to EBV-infected B cells is essential for resolving infection and is largely responsible for lymphocytosis and other symptoms associated with acute disease.
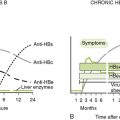
2. Heterophile antibody-positive infectious mononucleosis (Fig. 22-2)
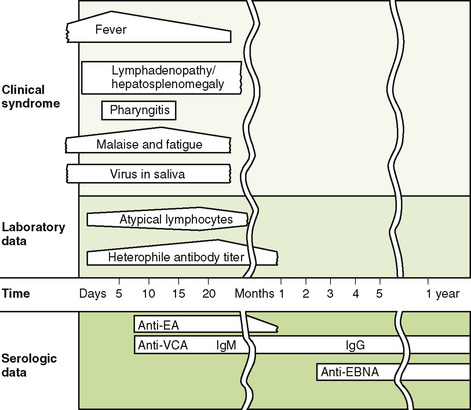
• Disease is milder in children than in adolescents or adults.
a. Symptom triad of lymphadenopathy, splenomegaly, exudative pharyngitis
b. Rash appears if the patient is given ampicillin (not an allergic reaction).
c. Saliva containing shed virions is the usual means of spreading EBV, most commonly during kissing or shared drinking glasses, bottles, and so forth.
• Asymptomatic infection or recurrence with virion production in oropharynx is common and promotes transmission.
• Much of the population is seropositive by 30 years of age.
• Atypical lymphocytes (Downey cells) are antigenically activated T cells on blood smear.
• Heterophile antibody is detected by heterophile antibody test or enzyme-linked immunosorbent assay.
a. Heterophile antibody, an early IgM response from EBV-activated B cells, cross-reacts with the Paul-Bunnell antigen on sheep, horse, or bovine (not guinea pig) erythrocytes, causing agglutination.
• Epstein-Barr nuclear antigen (EBNA) is a late marker of infection present in all infected cells.
• Antibodies to early antigen (EA) and viral capsid antigen (VCA) are detectable during active infection.
• Antibodies to EBNA are produced after resolution of infection after release of EBNA due to T cell killing of infected cells.
4. Other diseases caused by EBV
a. Raised, corrugated white lesions that do not scrape off in mouth, especially on the tongue
b. Occurs only in immunosuppressed patients, especially patients with acquired immunodeficiency syndrome (AIDS)
• CMV infects most cell types.
• Initial nonlytic infection primarily of epithelial cells is followed by latent infection of monocytes, macrophages, and lymphocytes.
• Cytopathic effects detectable in infected cells
• Cell-mediated immune response generally controls and resolves infection in immunocompetent individuals.
• CMV infection of children and adults is usually asymptomatic.
a. Virions produced in the mother can cross the placenta and infect the fetus.
b. Symptoms include rash, periventricular cerebral calcification, hepatosplenomegaly, deafness, microcephaly (small head), and mental retardation.
c. Most severe manifestations are associated with primary maternal infection during pregnancy.
d. Less severe manifestations are associated with recurrent infection in a seropositive mother.
• Opportunistic diseases in immunosuppressed individuals, especially AIDS patients and transplant recipients
1. This family consists of large, complex, brick-shaped viruses with a linear, double-stranded DNA genome.
2. Unlike all other DNA viruses, poxviruses replicate in the cytoplasm. Virions carry RNA polymerase for synthesizing messenger RNAs, and virus-encoded DNA polymerase produces progeny genomes.
1. Human virus causing smallpox, which is now eradicated
2. Vaccination with vaccinia virus was used in eradication efforts against smallpox.
C Animal pox viruses (e.g., vaccinia, orf, monkeypox)
1. Human virus that causes small raised, umbilicated lesions on the trunk, genitals, and proximal extremities
2. Lesions occur singly or in groups and have a central granular plug containing virions (molluscum bodies)
3. Infection is benign, usually self-limited, and transmitted by close contact or fomites.
4. All populations are susceptible.
5. May be disseminated in human immunodeficiency virus (HIV)